
Dr. Siddharth Madan, S16243, Dr. Zia Chaudhuri, Dr. Zia Chaudhuri
Abstract
A 55-year female presented with acute onset diplopia. Visual acuity was 6/6 partial OU with +0.5DS. Pupils, extra-ocular movements, colour vision and contrast sensitivity were normal with 30 degrees right comitant esotropia. Fundus examination and optical coherence tomography (OCT) revealed dry age-related macular degeneration (AMD). The patient had HbA1C of 6.3%, deranged lipid profile, normal values for thyroid functions and negative results for anti-nuclear (ANA), anti-acetylcholine receptor antibody and rheumatoid factor. MRI and MRA brain with orbit were normal. The AACE recovered completely in 4 weeks on a diabetic diet, aspirin and rosuvastatin. Single-eye occlusion was prescribed to alleviate symptomatic diplopia. We speculate that micro-angiopathy due to previously undiagnosed pre-diabetic status may have contributed to this spontaneously improving self-limiting AACE as the subject was found to have no other structural or metabolic anomaly than the mildly raised HbA1C levels.
Key-words: Adult-onset acute acquired comitant esotropia (AACE), cerebral microangiopathy
Key Messages:Microangiopathy due to previously undiagnosed pre-diabetic status may contribute to self-limiting acute acquired comitant esotropia(AACE)in patients with no other structural or metabolic anomaly other than the mildly raised HbA1C levels. Neuroimaging and metabolic work up is thus of help.
Introduction
Acute acquired comitant esotropia (AACE) can pose a diagnostic dilemma to the treating ophthalmologists and neurologists because of its clinical association with underlying neurological disorders. Acute onset esotropia with diplopia indicates a newly acquired deviation in a subject usually older than five years, adolescents and young adults with normal pre-existing binocularity. Its presence should incite comprehensive evaluation for any possible evidence of incomitance. AACE is a rare clinical entity and literature is scant regarding its actual incidence or prevalence.1
Case Report
A 55-year old female presented to us with acute onset diplopia for 1 day without any previous systemic or precipitating illness. Visual acuity on presentation was 6/6 partial in both the eyes. Pupillary reactions were normal. She had a right comitant esotropia of 30 prism diopters (Fig. 1E). Refraction under cycloplegia using 2% homatropine eye drops revealed no significant refractive error. She had a +0.50 diopter of simple hypermetropic astigmatism against the rule. Ocular movements (Fig. 1A-1I), colour vision and contrast sensitivity were normal in both the eyes. On fundus examination, occasional drusens could be seen in the right eye with macular hypopigmentation without any obvious optic disc edema. Fundus fluorescein angiography was inconclusive and OCT macula was performed that was suggestive of dry age related macular degeneration in both the eyes. Blood pressure was normal on presentation. On evaluation, fasting blood sugar was 113.12 mg/dl, HbA1C was 6.3 % and serum lipid profile was deranged with serum triglycerides levels of 305 mg/dl, low density lipoprotein levels being 114.20 mg/dl, total serum cholesterol 236.1 mg/dl and raised very low density lipoprotein levels (63.80 mg/dl). Thyroid function tests, Anti-neurtrophilic antibody, Anti-acetylcholine receptor antibody and Rheumatoid arthritis factor were negative. Magnetic resonance imaging of the brain with orbit (Fig. 2A, 2B, 2C) and magnetic resonance angiography of the brain (Fig. 2D, 2E) were normal. Presuming a pre-diabetic state after an endocrinology consultation, she was advised a diabetic diet. Aspirin and rosuvastatin were started. Left eye patching was advised to alleviate disabling diplopia.After a follow-up at 2 weeks, diplopia recovered considerably with mild esophoria and the patient was able to fuse intermittently. She was asymptomatic after a further follow-up of 2 weeks. (Fig. 1J- 1R).
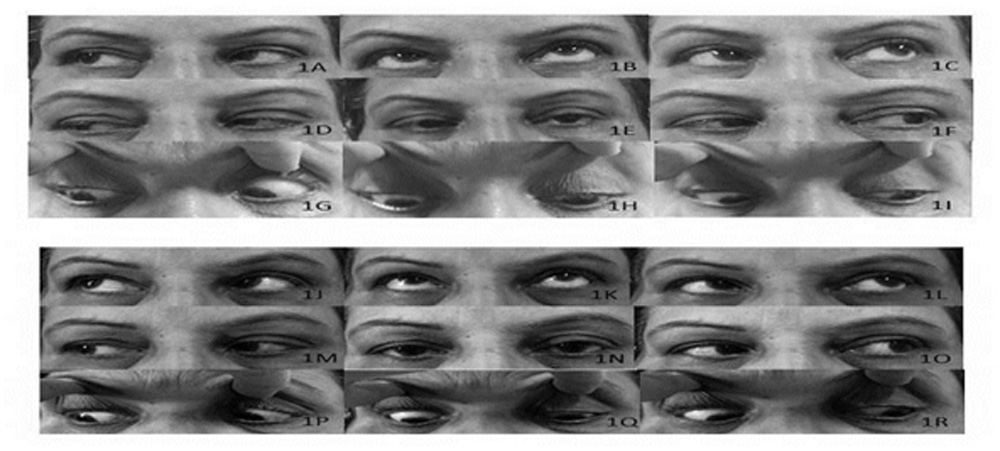
Figure 1A- 1R: Sequential patient photographs: On presentation, this 55 year old female had a right comitant esotropia of 30 prism diopters (Fig. 1E). The ocular movements were full and normal in all directions of gaze (Fig. 1A-1D,1F-1I). At 2 weeks, she had complete amelioration of diplopia and at 4 weeks from the onset of illness, she had adequate ocular alignment without any esotropia (Fig. 1J-1R).
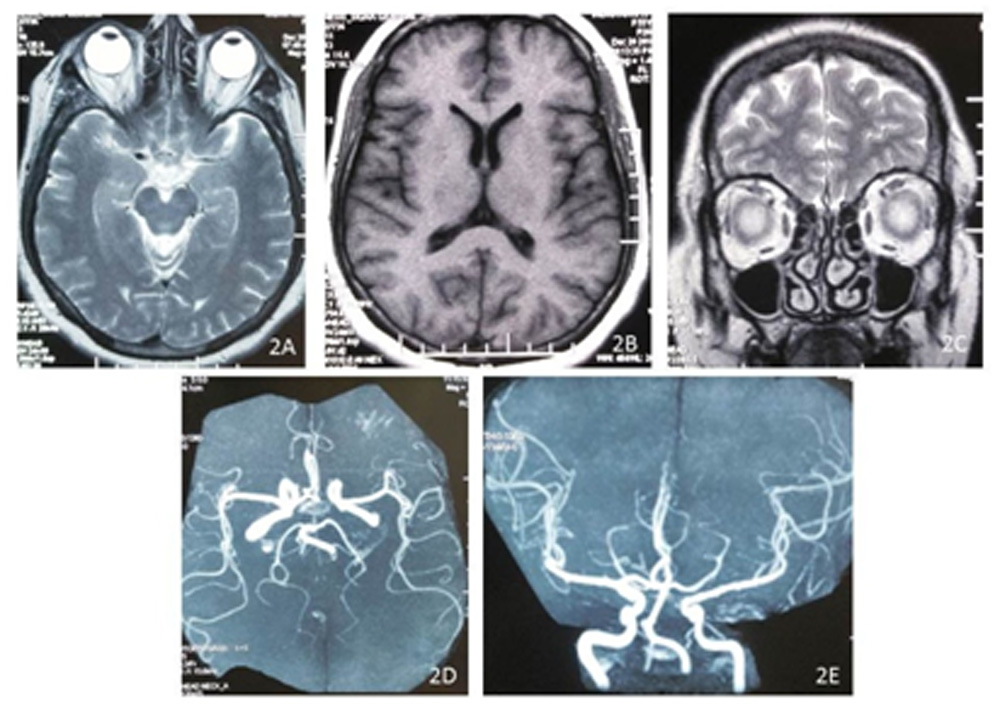
Figure 2A-2E: Neuroimaging Photographs: Magnetic resonance imaging of the brain (Fig. 2A, 2B) with orbit (Fig. 2A, 2C) and magnetic resonance angiography of the brain (Fig. 2D, 2E) were normal.
Discussion
Acute onset of a moderate to large size esodeviation which is similar in all gaze positions resulting in diplopia with a full ocular motility and absent lateral incomitance without accompanying visual deterioration aptly describes AACE. These patients demonstrate good fusion with corrective prisms or n a synoptophore.2There is no change in the degree of esotropia with the use of corrective spectacles. The causes for AACE are multifactorial ranging from idiopathic, occlusion therapy for anisometropic amblyopia (in children) to the presence of an underlying ocular or intracranial pathology. Presence of abducting nystagmus, non- achievement of binocularity after ocular realignment, evidence of a V-pattern and a near-distance disparity in deviation are all the possible clinical signs that prompt evaluation of an underlying CNS tumour in patients with AACE.3, 4, 5, 6Tumors of the cerebellum, pons, hypothalamus, corpus callosum, Arnold-Chiari malformation and idiopathic intracranial hypertension have been known to cause ACE, but the exact underlying mechanism for a comitant deviation remains uncertain.3, 4, 5, 6Acute esotropia in adults can be observed following a sixth nerve palsy, divergence paralysis, age relateddistance esotropia, restrictive or a sensory squint, accommodative esotropia, consecutive esotropia , decompensated monofixation syndrome, ocular myasthenia gravis, and an underlying neurological disorder.
Three distinct categories have been described for acute onset comitant esotropia. Characteristic features include a large angle of deviation, good binocularity and no underlying neurological pathology. Type I (‘Swan type’) follows disruption of binocularity by monocular occlusion, type II (‘Franceschetti type’) has no obvious underlying cause other than possible ‘physical or psychic shock’ and type III (‘Bielschowsky type’) is associated with myopia of −5.00 diopters or more.7A type of strabismus associated with high myopes is described as “heavy eye” syndrome (myopic strabismus fixus) in which there is inferiordisplacement of the lateral rectus (LR) resulting in esotropia and hypotropia with limited supraduction and abduction.8 Comitant esotropia is a benign clinical entity and does not warrant comprehensive neurological evaluation for an underlying pathology as proposed by few research scholars.1iology
The cerebral microangiopathy of diabetes involves signal pathways such as metabolic abnormalities of polyol, saccharification hyperactivity, abnormal transport of amyloid-β across blood-brain barrier, oxidative stress and activation of protein kinase.9Alterations in the blood-nerve barrier are observed as a result of loss of tight junctions and microvascular pericytes, hypertrophy of the microvascular basement membrane eventually producing oedema, and hypoxia in the endoneurial space. Statins chiefly rosuvastatin, improve epithelial cell function, reduce oxidative stress, alleviate arteriosclerosis and inflammation and normalizes metabolic malfunctions significantly.10 Additionally these drugs decrease fasting glucose levels, improve glucose tolerance, and decrease fat tissue weight and adipocyte size. Cytotoxic T cell activity is enhanced and serum tumor necrosis factor-a and interleukin 6 levels are decreased by these agents. All these factors help in early normalization of microangiopathic changes induced by diabetes or uncontrolled blood sugar levels and may augment recovery of a neurological deficit.
Neuroimaging is a must in elderly patients to rule out an underlying neurological disorder. Management is chiefly conservative and non-surgical. Nonsurgical treatment options include ocular occlusion, prism therapy, and botulinum toxin type-A injection.7 Prisms usually help in subjects with a small-angle strabismus (less than 15 prismdiopters). Non- resolving large angle squints may require strabismus surgery after a close follow-up.
AACE patients without any underlying neurological disease warrant a comprehensive evaluation for an undiagnosed metabolic disorder like diabetes. Prompt intervention can achieve good motor and sensory outcomes.
References
- Hoyt S.andGoodW. V., “Acute onset concomitant esotropia: when is it a sign of serious neurological disease?” British Journal of Ophthalmology, vol. 79, no. 5, pp.498–501, 1995.
- Rutstein RP, DaumKM. Anomalies of Binocular Vision: Diagnosis and Management. St. Louis: Mosby, 1998; p.80–243
- Williams AS, Hoyt CS. Acute comitant esotropia in children with brain tumors. Arch Ophthalmol 1989;107:376-8.
4. Fledelius HC.Acute acquired comitant esotropia: a prospective study.Eye (Lond). 2000 Aug;14 ( Pt 4):686.
5. Jampolsky AJ. Problems in strabismus management.Transactions of the New Orleans Academy ofOphthalmology. New York: Raven Press, 1986:456.
- Scott W. Problems in strabismus management. Transactionsof the New Orleans Academy of Ophthalmology. New York:Raven Press, 1986:456.
- Turan Kadriye Erkan and KansuTulay. “Acute Acquired Comitant Esotropia in Adults: Is It Neurologic or Not?” Journal of Ophthalmology, vol. 2016, Article ID 2856128, 9 pages, 2016. doi:10.1155/2016/2856128
- Chaudhuri Z. and DemerJ. L. “Sagging eye syndrome: connective tissue involution as a cause of horizontal and vertical strabismus in older patients,” JAMA Ophthalmology, vol. 131, no. 5, pp. 619–625, 2013.
- Li Y, Zeng KW, Wang XM.Cerebral microangiopathy of diabetes.ZhongguoZhong Yao Za Zhi.2017 x Jun;42(12):2247-2253. doi: 10.19540/j.cnki.cjcmm.2017.0104.
- LiaoJ.K., LaufsU..Pleiotropic effects of statins, Annu. Rev. Pharmacol. Toxicol.45 (2005) 89.
Legends to figures
Leave a Comment