
Dr. Gitumoni Sharma (S12413 )
Purpose: Results of first 100 VR cases by a beginner surgeon in an advanced set up in a tertiary care centre.
Settings and Design:Tertiary referral eye care.Retrospective interventional study.
Methods and Material:Retrospective analysis of patients who underwentvitreoretinal surgery was done. Beginner surgeon is defined. The cases were divided into 8 groups based upon their etiology. The categories having the maximum number of cases were found out. Outcome of surgeries were found in terms of visual acuity at presentation, Ist day and 42nd postoperative day and anatomical integrity. The complications if any were noted.
Results:There were 99 eyes for analysis. Retinal detachment were 18, open globe injuries 15, endophthalmitis 16 , proliferative diabetic retinopathy and tractional retinal detachment 16, vitreous haemorrhage 12 ,nucleus drop 5, other minor procedures 17.Three eyes were one eyed.one (6%) patient of the retinal detachment surgery did not improve due to the development of macular hole at a later stage.three(13%) in the open globe group and three(19%) in endophthalmitis group each had phthisis bulbi.Only one (9%) case of proliferative diabetic retinopathy and tractional retinal detachment had redetachment and undergone silicone oil exchange. No patients had redetachment after silicon oil removal. The non-improvingvision in 15 cases was because of the severity at presentation. Anatomical success was 100% in the retinal detachment and nucleus drop group. Paired-t test was significant in retinal detachment (P=0.001), open globe (P= 0.001), endophthalmitis (P= 0.001), proliferative diabetic retinopathy and tractional retinal detachment(P = 0.001)and vitreous haemorrhage group (P=0.001).
Conclusions:Beginner performed vitreoretinal procedures in different groups with good outcome in terms of visual acuity and anatomical outcome with lesser complications related to the surgery.
Key-words:Vitreoretinal surgeries, endophthalmitis, phthisis bulbi, advanced vitreoretinal set up, beginner VR surgeon
Key Messages: The several factors of inertia at the level of a beginner vitreoretinal surgeon should not be there because the advanced vitreoretinal surgical techniques have improved the overall success rate of all the vitreoretinal procedures.
Vitreoretinal surgery undoubtedly has a steep learning curve—. Adjustment to surgical technique and prior experience with a technique seemed to flatten the learning curve2.Introduction:
There are numerous studies to demonstrate that operative volume often yields improved clinical outcome 3. The field of retina is constantly changing4. Thankfully, modern vitreoretinal surgical techniques have reduced overall complication rates5.
There are several factors of inertia at the end of the beginner vitreoretinal surgeon which determines the results of the first few surgeries. In this study, the outcome of such surgeries in terms of visual acuity and anatomical success and its associated complications and their cause wereanalysed.
Subjects and Methods:
Retrospective analysis was done, of the case sheets of 100 patients who had undergone vitreoretinal surgery and management by a single beginner surgeon independently in an advanced vitreoretinal set-up in a tertiary eye care. All the diagnosis and surgeries were done by a beginner surgeon. Expert opinion was sought if needed from a senior surgeon with more than 15 years experience in vitreo retina. Beginner surgeon is a 24 months vitreoretinal fellowship trained surgeon who is doing independently for 10 months. Visual outcome defined as good, poor and equivalent as compared to presenting visual acuity.
This study was IEC approved [Project No. IEC /MGMEI /I/105 /10, dated 21.09.2015] and adhered to the tenets of the Declaration of Helsinki.
The case sheets numbers were taken out from the OT register of those cases which were operated by the beginner surgeonafrom Nov. 2014- t Sep. 2015. The different surgeries done in each cases and the diagnosis was recorded. The visual acuity was noted at preoperative, first postoperative and final postoperative visits at 42nd day of the patient. All the surgeries were performed with either 23 gauge or 25 gauge Constellation vitrectomy system with (Volk minicord Excel) wide angle viewing system with SDI.
Further, datas were entered into MS- Excel sheets. Further, there were divisions into 7 more groups depending on their diagnosis and treatment undergone as Retinal Detachment undergone vitrectomy +/- belt buckle , Open globe injury repaired , Endophthalmitis undergoing vitrectomy, Vitrectomy for Proliferative Diabetic Retinopathy with Tractional Retinal Detachment and Vitreous Haemorrhage , Vitrectomy for vitreous haemorrhage due to other causes, Nucleus drop undergone vitrectomy. The categories having the maximum number of cases were found out. Outcome of surgeries were found out in terms of Visual acuity at presentation, Ist post- operative day and at final visit of 42nd day. The complications if any were noted.
Statistical calculation was done using Microsoft Excel and Statistical Software SPSS 160.0. Visual acuity was notedinlogMAR.For visual acuity less than logMAR 1.00, were changed as per proper method mentioned by Holladay JT6. Paired student t-test was done to see the significance of variation between pre operative and 42 nd day post operative vision in the same group. P-value <0.05 was considered to test the 5% level of significance. Results:
There were a total of 100 eyes operated between Nov. 2014 – Sep. 2015 by a beginner surgeon One case was excluded from the analysis as was diagnosed as pediatric giant retinal tear on the table and was handed over to the experienced surgeon for further intervention.
The 99 cases which were analyzed in this study were again divided into 7 groups for ease of analysis (Table. 1). Retinal detachment undergoing vitrectomy with and without scleral buckle were 18 eyes, open globe injuries getting repaired were 15 eyes, endophthalmitis undergoing vitreous biopsy and vitrectomy were 16 eyes, Vitrectomy for Proliferative diabetic retinopathy with tractional retinal detachment were 16 eyes, Vitrectomy done for vitreous haemorrhage due to other causes were 12 eyes, nucleus drop undergoing vitrectomy were 5 eyes and other minor procedures like intravitreal injections with cataract surgery after +/- pan retinal photocoagulation were 17eyes.
3 patients were one eyed. One adult had cataract with total rhegmatogenous retinal detachment with PVR changes. He underwent BB+ Vit+ SOI and then Phaco IOL + SOR in second stage. His BCVA improved from PL in the preoperative period to 1.3 logMAR in the final check-up. The other two were of paediatric age groups. The first one was chorioretinalcolobomatous retinal detachment who underwent Belt Buckle+ Vitrectomy + Silicon Oil Infusion and then later Silicon Oil Removal + 14% C3F8 injection. BCVA in the final visit was 0.5 logMAR from HM+ve. The other was a macular on total rhegmatogenous retinal detachment who first underwent Belt Buckle+ Vitrectomy + Silicon Oil Infusion and then Silicon Oil Removal in second stage. BCVA in this case improved from CFCF to 0.6 logMAR.
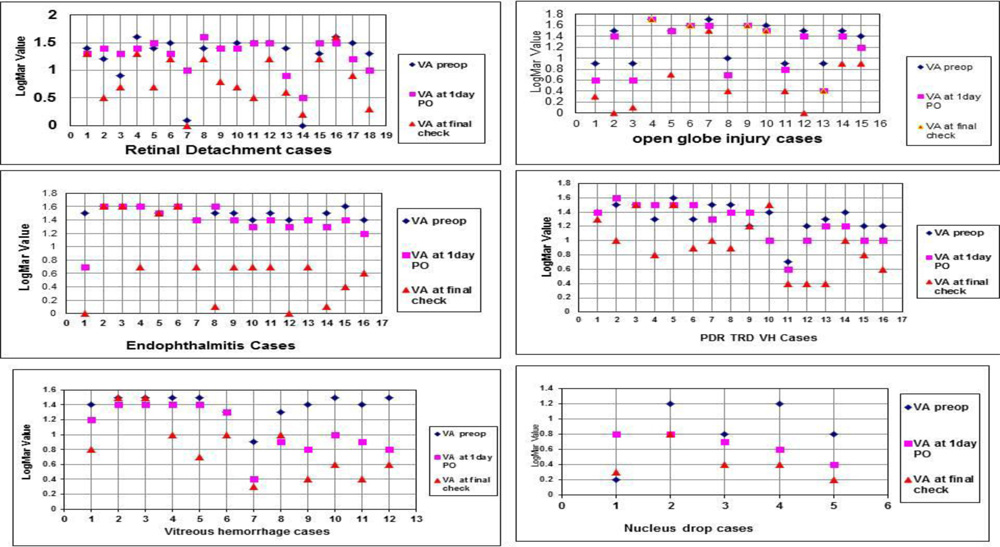
The X-Y Scatter in Fig.1,2 , 3, 4, 5 and 6, compares the logMAR visual acuity in preoperative, first postoperative day and 42nd postoperative day in each groups.1(6%) patient of the PVR with total RD surgery did not improve due to the macular hole developing later. Fig.1.
3(13%) patients in the open globe group had phthisis bulbi. Inspite of the globe repair being done successfully and though the globe was salvaged, these patients had irreparable retinal detachment seen on the B-Scan in the first post-operative day Fig.2. 2(20%) patients in the open globe group did not improve after the successful repair. One patient had persistent PL vision due to traumatic optic nerve injury. Another patient had prexisting total corneal opacity due to which he had persistent HM vision. Fig. 2.
3(19%) in the endophthalmitis group each had phthisis bulbi. One patient was of corneal tear repaired with endophthalmitis due to Aspergillus fungus, the other patient was post-operative (cataract surgery) endophthalmitis with Fusarium and yet another had delayed bleb related endophthalmitis with Gram Positive Cocci with choroidal detachment. Fig.3. 1(6%) patient had subsilicon retinal detachment who was in paediatric age group and had gram negative and gram positive endophthalmitis following injury by pencil.
Only 1 (9%) case of proliferative diabetic retinopathy with tractional retinal detachment had redetachment and undergone silicon oil exchange. Another 2(18%) patients were operated on advanced stage of proliferative diabetic retinopathy and vision did not improve significantly after surgery.Fig.4.
2(17%) case in Vitreous haemorrhage did not improve due to optic atrophy in one and recurring vitreous haemorrhage (8.3%) in the other. Fig.5.
All the 5(100%) cases of nucleus drop were managed successfully with good visual outcome.
Others category included patients who were treated for either macular oedema or with or without cataract. Visual improvement is shown in these groups also and no any related complication is shown. Any systemic factors for macular edema is also addressed, if any, found during the study by referring to physician.
The non-improving vision in all these 15 (15.15%) cases was because of the severity at presentation and no surgery related complications were noted in any of the case. No patients had redetachment after silicon oil removal.
Although, the X-Y scatter plotted shows final visual acuity to be better in the cases individually, but Paired sampling t-test was significant in final visual acuity at the post-operative period in retinal detachment (P = 0.001), open globe injury(P= 0.001), endophthalmitis(P= 0.001) and PDR TRD groups (P = 0.001) and vitreous haemorrhage (P = 0.001). This shows that individually, the case did better in most of the cases after the surgery. Paired sampling t-test in the nucleus drop group was (P = .049) and in the others group was (P= 0.536). Variation was not significant in these groups probably because of fairly good presenting visual acuity or not an excellent postoperative visual acuity post-operatively and also for a relatively less number of cases. Table 2.
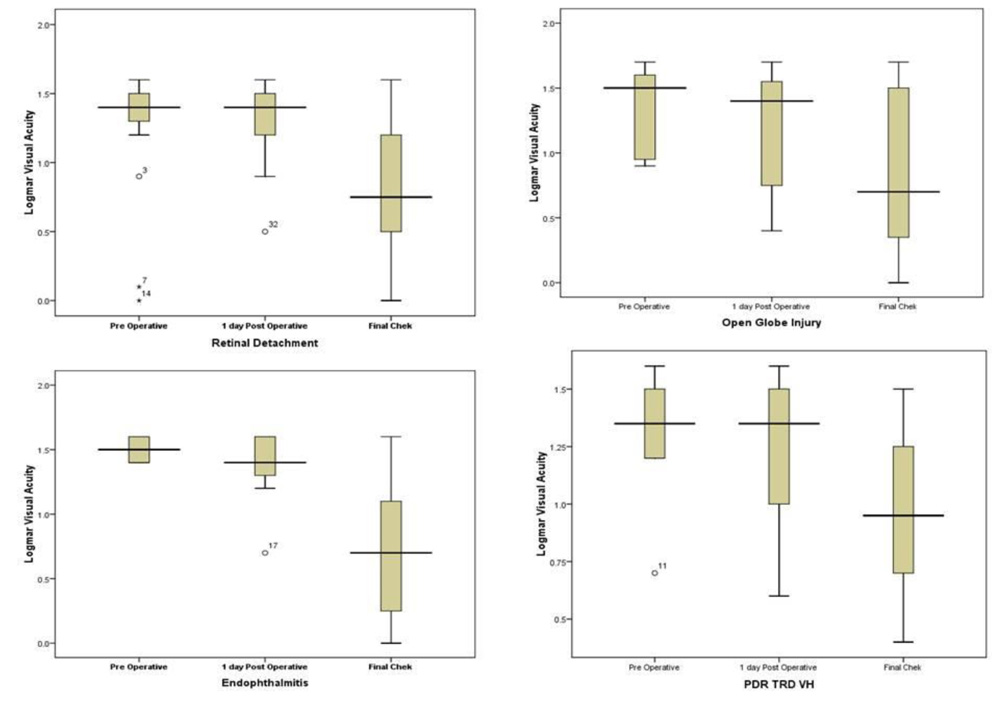
Box plot analysis (Figure.7 ) in each group represents that the data of final check is more normal than the pre-operative and one day operative data except the other cases group where the preoperative and first postoperative data are also near normal as similar with the paired sampling t-test. This signifies a favourable result in the final post-operative check-up of the patients.
Discussion:
Learning how to avoid complications and knowing what steps to take if they do occur takes years of practice. As we are learning the different surgical approaches of our attending’s, it is important to follow up on these patients to know their long-term outcomes. With cautious surgical technique, the complications can be avoided7. During training the beginners learn different surgical approaches of their masters and it is applied when they perform independently, it is important to follow-up on these patients to know their long-term outcomes. At times, expertise remain helpful in complex situations for a better outcome as was in this study in a case of paediatric giant retinal tears. With cautious surgical decisions and techniques, the complications can be avoided as is shown from this study where there is no major surgery related complications.
In the past 10 years, there has been an exponential increase in the number of practice-changing prospective, randomized trials published in the field of retina. Advancements in pharmacotherapy and laser technology are similarly occurring at an ever-increasing pace.
O’ Grady GE8had found the techniques required for successful surgery are noteasily mastered, and ‘ it is the author’s practice to have a trainee assist on about 50 operations before assuming major responsibility for a difficult microdissection’. The beginner surgeon in this study fulfils the criterion before beginning independently.
Pharmakakis et al9had found that having applied standard exam. and treatment protocols, the efficacy of the management of diabetic patients was consistent with international standardseven though patients were treated mostly by doctors in training. Recently, Mazinani et al10had concluded that although the intraindividual learning defect being higher in beginners the primary anatomical success were not related to the number of vitreoretinal procedures. In this study, seven different types of vitreoretinal pathologies were intervened by beginner surgeon. The outcome in terms of visual and anatomical in the 6th week postoperative period was good individually in most of the cases. The non- improvement of vision in 15(15.15%) cases were because of the severity at presentation.
Fenk k et al11in their study of prognostic indicators for no light perception after open globe injury had found closed funnel retinal detachment or retinal prolapse to be a statistically significant(P = .005) prognostic indicators for pthisis after open-globe injury. In this study, there were 3(13%) pthisis bulbi in the open globe repaired due to irrepairable retinal detachment diagnosed in the immediate post operative period on B-Scan after primary repair of the open globe.
Christiane et al12had shown redetachment after silicon oil removal occurred in 20 eyes (17.4%) in first 6 months. In this study, no patients had redetachment after silicon oil removal upto 6th weeks of post-operative follow-ups.
MS Dikopf et al13 in surgical outcome of 25-guage pars plana vitrectomy for diabetic tractional retinal detachment recently, had found redetachment rate of 10% for diabetic tractional retinal detachment.This study found, recurring retinal detachment in diabetic tractional retinal detachment to be 9%.
Others category, included patients who were treated for either macular oedema and/or cataract and there were 17 eyes.Visual improvement is shown in these groups also and no any related complications is shown.. Any systemic factors for macular edema is also addressed, if any, found during the study by referring to physician.
There are, however, fewer limitations in this study. They are: 1) retrospective study. 2) The analysis is based on operative results and the resources (time, materials and human resources) to achieve these results cannot be studied retrospectively. 3) There may be author bias in writing the analysis. 4) Follow up period was short. But, the strength of the study lies in the fact that this study is first of its kind in vitreoretinal diseases comprising of many groups of interventions done by the beginner surgeon.
Conclusion:From this study it appears that with improved technological advances in vitreoretinal surgeries, beginners also can have a reasonably good outcome of the cases managed and the learning curve can be flattened to some extent. The chances of complications are also minimized.
References:
1.Nagy ZZ, Takacs AI, Filkorn T, Kránitz K, Gyenes A, Juhász É, Sándor GL, Kovacs I, JuhászT, SladeSComplications of femtosecond laser-assisted cataract surgeryJ Cataract Refract Surg. 2014 Jan;40(1):20-8.
2.Bali SJ, Hodge C, Lawless M, Roberts TV, Sutton GEarly experience with the femtosecond laser for cataract surgery Ophthalmology. 2012 May;119(5):891-9.
3. Halm EA; Lee C; Chassin MR Is volume related to outcome in health care? A systematic review and methodologic critique of the literature, Ann Intern Med 2002; 137: 511-520.
4. Alok S Bansal, Nikolas London, AndreWitkinSurgical Pearls for the Beginning Vitreoretinal Fellow, Retina today. 2011 Sep:26-30.
5. Adam Gerstenblinth, Francis Char DeCroos, Rajiv Shah Making most of Your vitreoretinal fellowship:Part 1 Retina Today. 2011November/December:29-30
6. Holladay JT Proper method for calculating average visual acuity.J Refract Surg. 1997 Jul-Aug;13(4):388-91.
7. Adam Gerstenblinth, Francis Char DeCroos,Rajiv Shah Making most of your vitreoretinal fellowship:Part 2 Retina Today. 2013January/February:26-28
8. O’Grady GEVitreous surgery and retinal detachment. Int Ophthalmol Clin.1976Spring;16(1):169-93
9. PharmakakisNM,Petropoulos IK, Peristeropoulos PA, Vantzou CV, Koliopoulos JX Evaluating the management of diabetic retinopathy in a teaching center. Eur J Ophthalmol 2002 Nov-Dec ; 12(6): 488 – 494
10. Mazinani BA, Rajendram A, Walter P, Roessler GF Does surgical experience have an effect on the success of retinal detachment surgery? Retina2012 Jan; 32(1):32-7.n2012;Vol32:32-37
11. Fenk K, Hu YT, Ma J Prognostic indicators for no light perception after open-globe injury Eye injury vitrectomy study,Am J of ophthalmol 2011 Oct;152(4):654 652.
12. Christiane IF, Susanne B, Andreas K Outcome after silicon oil removal Br J ophthalmol 2001 Nov;85(11): 1324-1327..
13. Dikopf MS, Patel KH, Setlur VJ, Lim JI Surgical outcome of 25-guage pars plana vitrectomy for diabetic tractional retinal detachment Eye 29 2015 Sept; 1213-1219.
Acknowledgement: Dr. Pradeep Kumar Chaurasia for all the statistical calculations.
Tables and Figures:
| 1. | RD undergone vitrectomy +/- belt buckle | 18 |
| 2. | Open globe injury repaired | 15 |
| 3. | Endophthalmitis undergoing vitrectomy | 16 |
| 4. | Vitrectomy for PDR TRD VH | 16 |
| 5. | Vitrectomy for vitreous haemorrahgedue to other causes | 12 |
| 6. | Nucleus drop undergone vitrectomy | 05 |
| 7. | Other minor interventions like inj, prp +/- Phaco | 17 |
| Total | 99 |
| Group | Pre-operative VA | 42nd day Final postoperative visual acuity | P value |
| RD | 1.25 | 0.83 | 0.002 |
| Open Globe | 1.40 | 0.94 | 0.014 |
| Endoph | 1.52 | 0.9 | 0.001 |
| PDR TRD | 1.35 | 1.09 | 0.084 |
| Vit. Haem | 1.37 | 0.97 | 0.012 |
| Nucleus drop | 0.73 | 0.50 | 0.580 |
| Others | 0.80 | 0.73 | 0.860 |
Legends
Table.1. 7 groups of patients operated
Fig.1 : Graphs showing the logMar Visual acuity in preop, 1day po, and final PO in each group.
Table.2. t-test showing the significance of variation ( P<0.05) in the preoperative and final post-operative visual acuity.
Fig.2.Box plot analysis in each group represents that the data of final check is more normal than the pre- operative and one day operative data except the other cases group where the preoperative and first postoperative data are also near normal.
Leave a Comment