
Dr. Alok Ranjan (R18966)
Intrastromal Keratopigmentation or Corneal Tattooing
Ranjan Alok 1, Mohan Shalini 2
1 Consultant , USD Hospital , Unnao (UP)
2 Associate Professor , GSVM Medical College , Kanpur (UP)
Introduction
Corneal opacity causes functional blindness as well as cosmetic difficulties. Functional treatments are undertaken for visual improvement and include procedures such as corneal transplantation. Because of advancement in microsurgery and new researches in medicine, incidence of Penetrating Keratoplasty had increased. But the patients with poor visual potential having a disfigured cornea can impair an individual’s self-confidence and can adversely affect one’s social and professional lives.
But in cases, where visual outcome is nil, one might consider cosmetic repair as one of the potential treatment options for corneal opacities in carefully selected cases to improve both the patient’s social relationships and personal sense of well-being.
Intrastromal Keratopigmentation (ISKP) or Corneal tattooing has been used for cosmetic treatment of corneal opacities for centuries. [1,2] It was first described by GALEN using copper sulphate and nutgall for unsightly leucomatous corneal opacity.[3,4,] Various chemical products such as Indian ink, metallic powders, organic colours, animal uveal pigment, Chinese ink, gold & platinum chloride, lamp black candle shoot, animal charcoal were also used. But the main problem affecting the outcome of previous ISKP studies was the fading of colours which made the results inconsistent over time. [5] This was also associated with recurrent corneal erosion syndrome and foreign body sensation.[6]
Intrastromal Keratopigmentation is done in patients who are intolerant to cosmetic lenses, had risk of phthisis, with orbital prosthesis, or had various complications of Penetrating Keratoplasty [7]. Thus to overcome these problems corneal tattooing is a very safe and cost effective method. Cosmetic lenses also have disadvantage of daily insertion, infection, giant allergic conjunctivitis etc .[8]
AIM OF STUDY
1: To improve cosmesis / visual disturbances in patients with corneal opacity using newer organic micronised pigment.
2: To compare the effectiveness of different techniques of corneal tattooing i.e Needle pucture , microkeratome assisted ISKP and combined.
MATERIAL AND METHOD
43 patients with Corneal opacity (CO) willing to undergo ISKP were included from Cornea Clinic of a GSVM Medical College, Kanpur. Written & informed consent as per Helsinki’s Declaration were taken. Two patients had lost to follow up, so finally 41 patients were included in our study. The maximum follow up was for 1 year. Patients were given set of 10 questionnaires at 3 months follow up to assess their satisfaction levels. The study was cleared from ethics committee of the institution.
Patients included in our study were
-
Blind eyes.
-
The eyes with no hope for visual recovery ( like with dense amblyopia, squint or posterior segment disease)
-
Eyes with eccentric scars
-
Eyes with corneo-iridic scars.
27 (66%) patients had superficial CO alone or deep CO associated with superficial CO, underwent needle puncture ISKP while Other 13 (32%) had deep CO were subjected to microkeratome assisted ISKP (Intra-stromal pocket).
1 (2%) patient had thick anterior capsular plaque with distorted pupil leading to visual disturbances; underwent both (needle puncture and microkeratome assisted) the procedures.
PROCEDURE
Procedure was performed under topical / peribulbar anaesthesia .
-
Needle puncture ISKP technique:
-
-
26 gauge needle was taken to make multiple stromal punctures without epithelial debridement
-
Pigment was spread on the cornea & inserted with the needle / fine iris repositor
-
-
Microkeratome assisted ISKP technique:
-
-
Horizontal incision with 15 no blade at the upper border of CO
-
Microkeratome (Crescent) taken to dissect a lamellar pocket beyond CO margins
-
Pigment inserted with the help of fine iris repositor
-
A 10–0 nylon suture put at the superior incision
-
All patients were followed up on day 1, 1st week, 1st month, 3rd month up to 1 year.
-
RESULT
Median age of the patients was 23.0 years (Range 16 – 41 years). Total 41 patients were included in our study. 13(32%) patients underwent microkeratome assisted ISKP and 27(66%) patients underwent needle assisted ISKP and followed up as shown in table (1&2).
Post operatively all patients had mild redness, lacrimation and ocular discomfort on 1st post op day which corresponds to surgically induced corneal defect. Most of complaints – resolved within 1 month with corneal re-epithelisation. On slit lamp examination patients with needle tract ISKP did not find uniform pigmentation but on diffuse light examination showed uniform pigmentation as shown in figure (1). Same patient was examined after 2 week as shown in figure (2). Corneal surface was smooth and uniform. With lamellar pocket ISKP had uniform homogenous distribution of pigment. After 3 month of follow up 39 (96%) patients were satisfied with result of procedure as shown in table (4).
DISCUSSION
Corneal tattooing or Intrastromal Keratopigmentation has been used for cosmetic treatment of corneal opacities for centuries[1,2]. It was first described by Galen using copper sulfate and nutgall[3,4,] and after that various chemical substances were used. Patients with poor visual acuity because of corneal disease, optical keratoplasty being the most acceptable treatment till date.
But in patients with poor visual outcome and good visual potential with eccentric corneal opacity, one might consider cosmetic repair as one of potential treatment option for disfiguring scars. ISKP was done in patients who are intolerant to cosmetic lenses, risk of phthisis with orbital prosthesis, and various complication of keratoplasty and would not result in functional outcome.
Now a days new organic micronised pigments are available for ISKP which has better cosmetic appearance and high patients satisfaction.[9] With the help of newer keratome assisted micronized pigment insertion technique has lesser long term complication, and fading of pigmentation has been reduced. Tattooing may persist for longer duration . ISKP is a safe surgical procedure, easy to learn and to perform, that does not require expensive materials and it avoids more extensive and invasive reconstructive ocular procedures. Cosmetic contact lenses, enucleation or evisceration with orbital prosthesis are the most frequently used methods to improve aesthetic appearance in cosmetically unacceptable, disabled eyes[10,11,12]. However, disabled eyes frequently have contact lens intolerance[13], and prostheses often cause inflammation and infection.[14] Penetrating keratoplasty (PK) has risks of infection and graft rejection and its use for cosmetic purposes is ethically unacceptable in many parts of the world due to the worldwide shortage of corneal donors.
Theoretically two Intrastromal Keratopigmentation technique is available:
-
Needle puncture ISKP technique (Superficial / Superficial with deep opacities):
-
Microkeratome assisted ISKP technique (Deep opacities).
Total 41 patients were included in our study. In which 26 patients were female and 15 patients were male with mean age 23 year (range 16-41 year) as in table (1 &2)
-
The 27 (66%) patients with superficial CO alone or deep CO associated with superficial CO, underwent needle puncture ISKP.
-
Others 13 (32%) with deep CO were subjected to microkeratome assisted ISKP (Intrastromal pocket).
-
One patient (2%) was subjected to combined (needle and intrastromal ) technique.
As we can see in table-3, complications like redness, lacrimation, pain and discomfort as foreign body sensation, were very less with intrastromal pocket technique and if present, most of them resolved in one week with the help of topical use of preservative free lubricant and low potency steroid. In needle puncture multiple puncture were made in cornea so multiple epithelial defect was present. As defect healed lacrimation and foreign body sensation reduced with time.
We compared the patient’s satisfaction based on questionnaire in table-4,
11 patients with microkeratome assisted ISKP were highly satisfied while 2 patient was satisfied. The 19 patients in needle puncture ISKP did not have satisfactory results on first follow up. Second sitting in 15 patients & third in 2 lead to satisfactory results. Sometimes one or two sittings of re-tattooing may be required to achieve patient’s satisfaction. As we can see that one patient was not satisfied with the result of needle puncture technique. Patients with high expectation, sometimes were not satisfied with results, so proper counselling of patient about procedure, result and complication should be properly explained.
CONCLUSION:
Keratopigmentation, in patients with corneal opacity with poor visual outcome or eccentric CO, is a very beneficial option available. As number of cosmetic lenses are available but there are many problems associated with it like daily insertion and removal, infections, allergic reaction, papillary conjunctivitis etc. Other thing that these lenses are very costly. So in these patients ISKP is a relatively permanent and cost effective. ISKP or corneal tattooing, using micronized mineral pigments may be considered as an alternative for patients in whom evisceration or prosthesis implants would otherwise be used to improve their cosmetic appearance. Corneal tattooing can be a procedure for long term or permanent correction of cosmetic eye deformities in patients who have cosmetically disabling corneal scars
| Table 1:- Demographic profile of patients |
| S.No | Diagnosis | No of patients | No of male | No of female |
| 1 | Blind eye with diffuse corneal opacity | 29 | 14 | 15 |
| 2 | Blind eyes with eccentric corneal opacity | 05 | 00 | 05 |
| 3 | Corneo-iridic scar | 03 | 00 | 03 |
| 4 | Eccentric corneal opacity with useful vision | 03 | 01 | 02 |
| 5 | Pseudophakic bullous keratopathy | 01 | 00 | 01 |
| Total | 41 | 15 | 26 |
| Table 2 |
| Type of surgery | Total no of patient | |
| Microkeratome assisted ISKP (Deep CO) | 13 | |
| Needle puncture ISKP (Superficial and deep CO) | 27 | |
| Combined | 01 | |
| Table 3 :- Post – Operative Result |
Microkeratome assisted ISKP (n=13)
| Follow up period | 1st day | 1st week | 1st month | 3rd month | 1 year |
| Redness | 13 | 01 | 00 | 00 | 00 |
| Lacrimation | 04 | 01 | 00 | 00 | 00 |
| Pain | 00 | 00 | 00 | 00 | 00 |
| Ocular discomfort | 04 | 00 | 00 | 00 | 00 |
Needle puncture ISKP (n=27)
| Follow up period | 1st day | 1st week | 1st month | 3rd month | 1 year |
| Redness | 27 | 16 | 02 | 00 | 00 |
| Lacrimation | 20 | 16 | 00 | 00 | 00 |
| Pain | 07 | 1 | 00 | 00 | 00 |
| Ocular discomfort | 27 | 17 | 02 | 02 | 01 |
| Table 4:- Patient Satisfaction Score |
| Poor | Average | Good | Excellent | |||||
| Needle puncture ISKP (n=27) | 01 (5.8%) | 01 (5.8%) | 06 (17.6%) | 19(n=70.5%) | ||||
| Microkeratome assisted ISKP (n=13) | 00 | 00 | 02 (14.2%) | 11 (85.7%) | ||||
| Combined (n=01) | 00 | 00 | 01 (100%) | 00 | ||||
FIGURE – 1
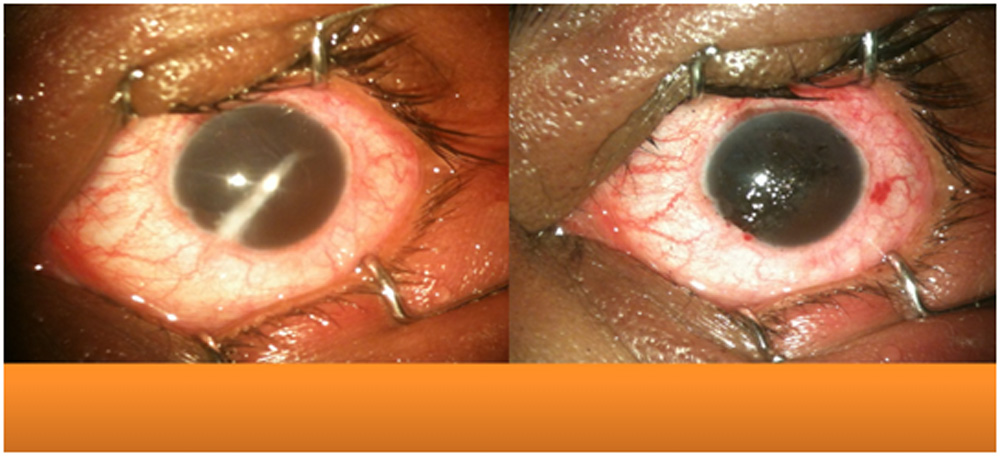
Needle puncture technique: Result immediately after surgery
FIGURE -2
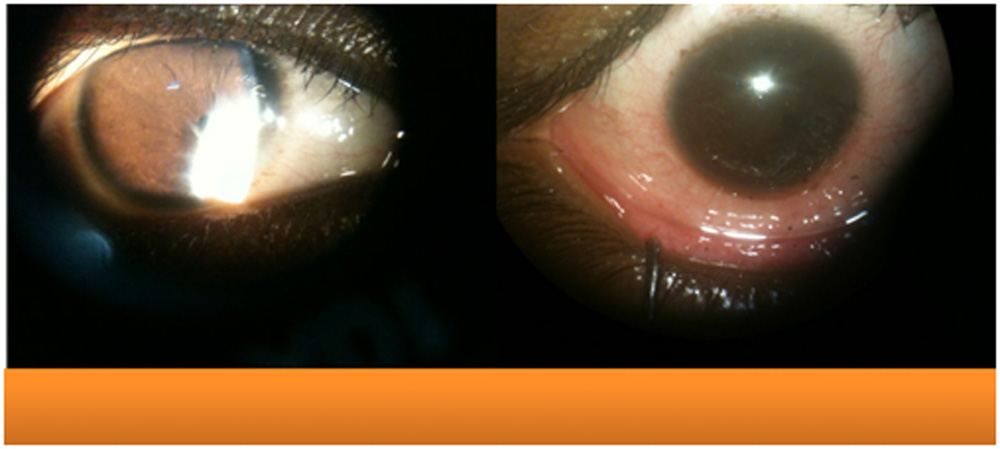
Needle puncture technique in eccentric corneo-iridic scar after 2 week
References:
1.Mannis MJ, Eghbali K, Schwab IR, Keratopigmentation: a review of corneal tattooing. Cornea 1999;18:633-7.
2. Leigh AG. Tattooing of the cornea. In: Duke-Elder S. System of ophthalmology. Vol VIII, Part 2, London: Henry Kimpton, 1965: 645-8.
3. Holth S. Revival of Galen´s corneal staining with coppersulfate and tannine should be abandoned. Am J Ophthalmol 1931; 14: 378-379.
4. Van der Velden-Samdeerubun EM, Kok Jh. Dermatography as a modern treatment for colouring leukoma corneae. Cornea 1994; 13: 349-353.
5. Jorge L Alio, Belucha Sirerol, Anna Walewska – Szafran Corneal Tattooing (keratopigmentation) to restore cosmetic appearance in severely impaired eyes with new mineral micronized pigments, British Journal of Ophthalmology bjo.bmj.com Br J Ophthalmol doi:10.1136/bjo.2008.149435.
6. Kim C, Kim KH, Han YK, Wee WR, Lee JH, Kwon JW.) Five-year results of corneal tattooing for cosmetic repair in disfigured eyes. Cornea. 2011 Oct;30(10):1135-9. doi: 10.1097/ICO.0b013e3181f2391a.
7. Garrido-Hermosilla AM, Angeles-Figueroa RA, Gessa-Sorroche M Surgical intrastromal keratopigmentation using tattoo ink Arch Soc Esp Oftalmol. 2013 Aug 2. pii: S0365-6691(13)00168-8. doi: 10.1016/j.oftal.2013.04.011.
8. Contact Lens Association of Ophthalmologists, Inc. Eye & Contact Lens 29(4): 196–200, 2003.
9. Alio JL, Sirerol B, Walewska-Szafran A, Miranda M.) Corneal tattooing (keratopigmentation) with new mineral micronised pigments to restore cosmetic appearance in severely impaired eyes Br J Ophthalmol. 2010 Feb;94(2):245-9. doi:1136/bjo.2008.149435. Epub 2009 Aug 12.
10. Ziegler SL. Multicolor Tattooing of the Cornea.Trans Am Ophthalmol Soc.1922;20:71-87
11. Hallock GG. Cosmetic trauma surgery. Plast Reconstr Surg. 1995; 95: 380-381
12. Kuzan WM. Jr. Plastic Surgery. J. Am Coll Surg. 1999; 188: 171-177
13. Hoeyberhs JL, Fortnightly review: Cosmetic surgery. BMJ. 1999; 318: 512-516.
14.Custer PL, Kennedy RH, Woog JJ, et al. Orbital implants in enucleation surgery. A report by the American Academy of Ophthalmology. Ophthalmol. 2003; 110: 2054-2061
Leave a Comment