
Dr. Rakesh Juneja (J15026)
Abstract:
Aim: To report outcome of Ozurdex implant in macular edema (ME) secondary to various posterior segment pathologies.
Settings and Design: Single-center, retrospective, interventional study
Methods and Material: Patients of ME were treated with one or more Ozurdex implants (0.7 mg). Data collection included demographic details, Best-corrected visual acuity (BCVA), central foveal thickness (CFT), duration of efficacy, and record of adverse events (if any) within 24 weeks.
Statistical analysis used: Paired sample t-test, Stata data analysis and statistical software, version 12.1, StataCorp, College Station, TX, USA
Results: 116 eyes of 104 patients were studied which had a diagnosis of diabetic macular edema (n=46), retinal vein occlusion (n=40), and uveitis (n=30). The average age of patients (mean± standard deviation) was 50.2±21.9 years. Baseline mean ± SD logMAR BCVA, CFT and intra-ocular pressure (IOP) were 0.636±0.4, 527.8±210.1 μm and 15.3±3.8 mmHg respectively. The reinjection interval was around 12-18 weeks. Ozurdex proved its efficacy in improving mean logMAR visual acuity and reduction of CFT from baseline till 12 weeks follow up period (0.414±0.5 and 301.5±278.5 respectively; p value < 0.05) and after 12 weeks follow-up it started worsening (0.530±0.9 and 444.8±375.2 respectively; p value >0.05). The most common reported adverse event was significant rise of intra-ocular pressure (>5 mmHg), with a total of 12 cases followed by cataract 9 cases.
Conclusion: Ozurdex implant lead to a significant improvement in BCVA and CFT values till 12 weeks, followed by a gradual decline for all the pathologies studied together. No new safety concerns were observed with the Ozurdex implant. The duration of efficacy was found to be less than 24 weeks.
Keywords: diabetic macular edema, uveitic macular edema, retinal vein occlusion, posterior segment pathologies, Ozurdex®
Key Messages:In real life scenario, Ozurdex implant is safe and effective and the mean duration of efficacy against macular edema secondary to various posterior segment pathologies is less than 24 weeks compared to 24 weeks duration as quoted by manufacturer
Introduction:
Posterior segment pathologies like diabetic retinopathy, retinal vein occlusion and uveitis can cause macular edema, culminating in significant deterioration of central vision.1,2Ozurdex (Allergan Inc., Irvine, CA, USA) delivers 0.7 mg dexamethasone, over six months. 3,4 It is approved by United States Food and Drug Administration (FDA) for the treatment of macular edema associated with retinal vein occlusion (RVO) and for non-infectious posterior uveitis.3,5
With the objectives, to evaluate anatomical and functional outcome, to assess efficacy and safety parameters, of Ozurdex in macular edema, a retrospective study was conducted, among Indian subset of population, in a tertiary care clinical setting.
Subjects and Methods:
Study design and patient enrolment:
This was a single-center, retrospective, open-label, interventional study with data collected from patients with ME secondary to various posterior segment pathologies, treated with one or more Ozurdex implant (0.7 mg) and provided informed consent to be enrolled in study. The synopsis was reviewed and ethical approval was provided by the Ethical Committee and institutional review board. Patients recruited through the retina clinic from February 2013 to July 2016, were enrolled in the study, and were assigned a registration number, and no patient-identifiable information was collected. The study adhered to the tenets of the Declaration of Helsinki.
Eligibility criteria and data collection
Data was collected under the following headings: demographic details, history of presenting illness, eye laterality, history and duration of diabetes, hypertension or any other associated systemic co-morbidities, diagnosis of retinal pathology responsible for macular edema, lens status, previous ocular intervention, duration between last intervention and first Ozurdex implant, clinical examination details including visual acuity at presentation and follow- up with imaging, treatment details, complications (if any) and treatment given for that complication. Inclusion criteria were: (1) Age >21 years (2) presence of ME in the study eye secondary to any posterior segment pathology; (3) best-corrected visual acuity (BCVA) <20/25; (4) central foveal thickness (CFT) >250 μm as measured by spectral domain optical coherence tomography (SD-OCT); (5) follow-up of at least 6 months after the first Ozurdex injection was administered; and (6) complete availability of documentation till the last follow-up. If any one of the above-mentioned inclusion criteria was not met, patients were excluded from the study.
Study Parameters:
Patients who met inclusion criteria were enrolled in the study and underwent a complete eye examination which included BCVA with the help of Snellen’s Chart, color fundus images (Topcon 50 Dx, Medical Systems Inc, Oakland, NJ, USA), fundus fluorescein angiography (FFA) (Spectralis, Heidelberg Engineering Inc, Heidelberg, Germany), and SD-OCT (Spectralis, Heidelberg Engineering Inc, Heidelberg, Germany). Previous treatments consisted of intravitreal injection of 1.25 mg per 0.05 ml of bevacizumab (Avastin; Genentech, South San Francisco, CA, USA) or 0.5 mg per 0.05 ml of ranibizumab (Lucentis; Genentech, South San Francisco, CA, USA) or pan-retinal photocoagulation or sectoral laser or intravitreal steroid injections (apart from ozurdex). Ozurdex (Allergan, Irvine, CA, USA) injection was given as per standard protocol. During the entire study period, none of the patient received any concomitant treatment.
In each case follow up data was collected on week, four, twelve and twenty four. Any further follow up data (if mentioned in records) was also noted. BCVA, Color fundus images and CFT values from SD-OCT noted during each visit was analysed. The criteria for defining treatment failure that required retreatment were as follows: loss of best-corrected visual acuity (BCVA) of more than five letters (ETDRS) and/or an increase in retinal thickness in OCT of >100 μm.6Adverse events like cataract, significant rise of IOP >5 mmHg, injection related adverse events were defined prospectively. Significant elevation of intra-ocular pressure (IOP) was defined as an increase of more than and or equal to 5 mmHg compared to the baseline level. The decision to institute anti-glaucoma therapy was made along conventional lines based on the degree of IOP elevation. None of the phakic cases for all pathologies included in the study had pre-existing cataract. LCOS III grading was used to grade the lens opacities during follow-up. The decision to perform cataract surgery with lens implantation was made in discussion with the patient, taking into account the level of vision in both the affected and fellow eye. All adverse event terms recorded in patient medical charts.
Data analysis and statistical methods
Being an open-label study, most analyses were descriptive. For statistical analysis Snellen’s visual acuity values were converted into logMAR at baseline and the last follow-up. Descriptive statistics included sample size, mean, standard error (SD), median, minimum, and maximum. Variables were summarized in frequency and percentage tables. Paired sample t-test was used to measure mean differences between pre- and post-implant values of all the parameters evaluated and obtained at first and the last follow-up visits. Statistical analyses were performed using commercial software (Stata data analysis and statistical software, version 12.1, StataCorp, College Station, TX, USA). P- value lay below 0.05 or 0.01, attained statistical significance (*) or high significance (**) respectively. The 95% confidence interval and statistical significance were analyzed using a generalized estimating equations model with a correlation structure. Various adverse events that occurred during the course of study were tabulated and computed using descriptive statistics.
Results:
Baseline Demographics:
One hundred fifty three eyes of 140 patients who received Ozurdex implant due to various segment pathologies were studied. Out of which, 116 eyes of 104 patients who met our inclusion criteria were included in the study and rest were excluded (Table 1). The average age of patients (mean± standard deviation) for all the pathologies in our study group was 50.2±21.9 years. Sixty patients were males and 44 patients were females. Twelve patients had bilateral retinal pathologies. Diabetes was the major co-morbid condition affecting 52 patients (50%) followed by hypertension affecting 39 patients (37.5%).
The most common retinal pathology encountered in our study group was DME comprising 46 cases (39.65%), followed by RVO 40 cases (34.48%) and uveitis 30 cases (25.86%). For all posterior segment pathologi
es mean ± SD logMAR BCVA, CFT and IOP at baseline were 0.636±0.4, 527.8±210.1 μm and 15.3±3.8 mmHg respectively. Overall 21 cases (18.10%) had pseudophakia at presentation of which DME, RVO & uveitis comprised 10 (8.62%), 4 (3.44%) and 7 (6.03%) cases respectively (Table 2).
Previous interventions:
DME and RVO, were reported to be treated with Intravitreal Ranibizumab in 2.58% and 1.72% cases respectively and with Intravitreal Bevacizumab in 3.44% and 5.17% cases respectively. Cases with uveitis were treated with posterior sub-tenon kenacort injections in 2.58% cases. Lasers (focal/grid or panretinal photocoagulation) were done overall in 19 eyes (16.37%), of which DME comprised a majority of 11 cases, followed by RVO 8 cases. The minimum duration between previous intervention and first Ozurdex implant was at least six months.
Ozurdex Implant Treatment:
The overall mean (± SD) number of injections for study eyes was 1.0±0.2 and individually with DME, RVO, and uveitis was 1.0±0.1, 1.1±0.1, and 1.0±0.2, respectively. The overall mean duration of Ozurdex implant after primary intervention for macular edema was 7.5 months and individually for DME, RVO and uveitis was 7.3, 3.2, 13.5 months respectively (Table 3).
Efficacy of Ozurdex in DME, RVO and uveitis:
Overall, Ozurdex proved its efficacy in improving mean logMAR best corrected visual acuity from baseline (0.636±0.45) till 12 weeks follow up period (0.414±0.5) (p value < 0.05) and after 12 weeks follow-up it started worsening (0.530±0.9) (p value >0.05) (Figure 1). For DME, RVO and uveitis the mean logMAR BCVA improved from baseline till 12 weeks (p value ≤ 0.05) and the amount of improvement was maximum in RVO followed by uveitis and DME (Figure 2). After 12 weeks follow-up, worsening or an increase in mean logMAR BCVA was seen which was observed more for DME, followed by uveitis and least for RVO.
In terms of reduction of CFT and improvement in macular edema, as compared to baseline value (527.8±210.1 μm) Ozurdex led to an overall improvement for all the posterior segment pathologies till 12 weeks (301.5±278.5;p value < 0.05) but after 12 weeks there was a resurge in macular edema leading to rise in overall mean CFT values (444.8±375.2; p value > 0.05) (Figure 3). Individually for DME, RVO and uveitis the mean CFT value improved from baseline till 12 weeks which was maximum for RVO followed by uveitis and least for DME but after 12 weeks follow-up there was an increase in CFT values in all the 3 pathologies signifying worsening of macular edema which gained a peak value for RVO followed by DME and uveitis respectively (Figure 4 and 7).
Safety of Ozurdex implant:
A total of 28 treatment-related adverse events were reported with Ozurdex implant in patients with a diagnosis of DME (19.56%; 9/46), RVO (17.5%; 7/40), and uveitis (40%; 12/30). The most commonly reported adverse event was increased IOP, with a total of 12 events, for DME (8.69%; 4/46), RVO (5%; 2/40), and uveitis (20%; 6/30 patients) (Table 4) (Figure 5). Overall, cataract was noted in 9 cases of which DME comprised 2 cases (22.22%), RVO 2 cases (22.22%) and uveitis 5 cases (55.55%). In each and every case, IOP was controlled with anti-glaucoma medications. None of the cases, having raised IOP required anti-glaucoma surgery. All cases diagnosed as having cataract were managed surgically with cataract extraction and IOL implantation (Figure 6)
Discussion:
This study highlights the role of Ozurdex in macular edema secondary to various posterior segment pathologies in an Indian clinical scenario, a real life situation. Several other studies describing various parameters like morphological and functional outcome, efficacy & safety profile of Ozurdex in macular edema have been conducted including various posterior segment pathologies individually but less as a whole. In Germany, a prospective study was conducted by Mayer et al; in 64 eyes of RVO patients. Out of which in Group 1, 38 eyes (22 central retinal vein occlusion and 16 branch retinal vein occlusion) received ozurdex alone. The mean injection numbers were 2.4 among CRVO patients and 1.8 among BRVO patients over the 12 months of study period. They reported that BCVA improved by 6.6 (±1.7) letters in CRVO and 7.8 (±2.9) in BRVO patients.6
A large multi-centric (167 clinical sites in 24 countries throughout the world) prospective study (Ozurdex Geneva trial that led to FDA approval of DEX implant in RVO) was conducted in patients (at least 18 years of age) with BRVO (Branch retinal vein occlusion) and CRVO (Central retinal vein occlusion) related ME (n=1267) who received, a single treatment with DEX implant 0.7 mg (n=427), DEX implant 0.35 mg (n=414), or sham (n=426) reported that percentage of patients who experienced improvement in BCVA ≥15 letters (3 Snellen lines) was higher in DEX implant group and also the duration to achieve this gain was lower as compared to sham group.3,7,8The study was also able to show that early treatment of macular edema was more beneficial than delayed treatment in restoring VA.3
Chhablani J et al & Totan Y et al in their studies have proven the role of Ozurdex implant in cases of Diabetic macular edema (DME) and DME resistant to intravitreal Bevacizumab treatment, in which DEX implant caused reduction in CFT & significant improvement in BCVA.9,10 The CHAMPLAIN study, a prospective, multicenter trial carried out in cases diagnosed as DME in a vitrectomised eye, have shown significant improvement in visual acuity (21.4% of diabetic eyes gained at least ten letters and 42.9% of eyes had improved at least five letters of visual acuity) and decrease in central macular thickness (27% at week 13 and 9.6% at week 26) after the dexamethasone intravitreal implant.3
The Ozurdex HURON Study group evaluated the safety and efficacy of two doses of dexamethasone intra-vitreal implant (DEX implant) for treatment of non-infectious intermediate or posterior uveitis, and concluded that a single DEX implant significantly improved intraocular inflammation and visual acuity persisting for six months.11 Another retrospective study by Tomkins-Netzer O et al included noninfectious uveitis (27 patients, 38 study eyes) found that repeat DEX implant injections resulted in improved ocular function and retinal thickness and resolved inflammation.12 Yuskel Totan et al also reported that Ozurdex results in significant improvement in baseline BCVA and reduction in CFT in cases of chronic DME.10
Ozurdex has been approved worldwide for the treatment of RVO in 2011, treatment of noninfectious uveitis affecting the posterior segment of the eye in 2012 and is recently approved for the treatment of adult pseudophakic DME since 2015.5,7,13 Our study included eyes with macular edema that were treatment naïve and also which had been previously treated with some or the form of therapy. Based on the pharmaco bio-kinetic profile of the drug, the re-injection interval quoted for treating re-current or non-resolving macular edema secondary to various posterior segment pathologies is six months.5 While our study found that for all posterior segment pathologies taken into account, there occurs a decline in mean CFT values and improvement in mean BCVA from baseline (527.8±210.1 μm & 0.636±0.4 respectively) till 12 weeks (301.5±340 μm & 0.414±0.2 respectively). At 24 weeks, a resurge in mean CFT values which was complimented with a decline in mean BCVA values (444.8±210.1 μm & 0.530±0.1) was observed which signifies that in a real world scenario the duration of efficacy or the pharmaco bio-kinetic profile of the drug is less than six months requiring a re-injection of Ozurdex in cases of recurrent and/or non-resolving macular edema before six months (Figure 1 and 3).
The most common adverse event was increased IOP (>5 mmHg) reported in 12 eyes post Ozurdex implant, for DME (8.69%; 4/46), RVO (15%; 6/40), and uveitis (6.66%; 2/30) patients. Lowder et al reported that in their study on any given follow-up visit, substantial increase in IOP (≥25 mmHg) occurred in less than 10% of treated eyes. 14,15 These 12 study eyes were managed with one or two anti-glaucoma medications and none of the eyes required more than two anti-glaucoma medications or anti-glaucoma surgery. Cataract was the second most common adverse event in our study comprising 9 eyes of which DME comprised 2 cases (22.22%), RVO 2 cases (22.22%) and uveitis 5 cases (55.55%). All these eyes underwent cataract surgery.
When these posterior segment pathologies were studied individually, it was observed that, mean CFT reduction from baseline at 12 weeks was maximum for RVO followed by DME and UME respectively (p value <0.05). This gradual reduction in CFT continued till 24 weeks as compared to baseline for RVO, DME & UME. But when CFT values were compared amongst 12 weeks and 24 weeks, it was observed that, there was a gain in CFT values at 24 weeks as compared to values at 12 weeks which was highest for RVO, followed by UME and DME respectively (p value >0.05). This data suggests that Ozurdex implant works much better in RVO cases followed by DME and UME cases in terms of reduction in macular edema or anatomical improvement. The amount of gain in mean CFT values is also much more in RVO cases at 24 weeks compared to 12 weeks which was followed by UME and DME cases respectively which signifies that the anatomical improvement attains its peak around 12 week period after which there is again a rise in CFT value indication re-worsening of anatomical improvement (Figure 1 and 2).
In terms of individual analysis of mean logMAR BCVA for various posterior segment pathologies, an improvement till 12 weeks was observed which was highest in RVO cases followed by UME and DME cases. But at 24 weeks this gain in mean logMAR BCVA was seen only for RVO and UME cases as compared to baseline values and deteriorated in cases of DME which was even more worse than the baseline value. This can be attributed to occurance of macular ischemia and poor metabolic control of diabetes during study period in certain cases of DME. This data suggests that there is a improvement in mean logMAR BCVA or functional improvement till 12 weeks for all three pathologies which was maintained till 24 weeks only for RVO & UME cases and DME cases had significant worsening around 24 weeks indicating that Ozurdex implant works best in RVO, followed by UME and least in DME cases. The functional gain reaches its peak around 12 weeks for all the three pathologies and then starts declining which is more for DME followed by UME and least in RVO cases.
In conclusion, the results of our study provide new insight on the real-world scenario and effect of Ozurdex implant across various posterior segment pathologies (individually as well as when studied together). Ozurdex implant provided one-line to three-line gain in visual acuity from baseline, along with significant improvement in CFT values for all the pathologies. No new safety concerns were observed with the ozurdex implant, and increase in IOP, was easily managed with topical IOP-lowering medications. Apart from providing data on functional and anatomical improvement achieved, safety and efficacy of Ozurdex implant, this study also focuses on duration of efficacy of Ozurdex implant which was found to be less than 24 weeks as compared to manufacturer’s quoted pharmaco-kinetic bio-profile (24 weeks). Although various forms of Anti-VEGF therapies still remain the primary modality of treatment in macular edema secondary to various posterior segment pathologies but in cases which, do not respond optimally or have recurrence, requiring repeat anti-VEGF injections, Ozurdex is a potent and viable option and can also be considered as primary line of management.
The major limitations of our study are its retrospective nature, less number of cohorts and open-label design. The adverse events were limited to those reported on the medical charts. The cases of retinal venous occlusion were not studied sub-dividedly into branch and central vein occlusion and thereafter ischemic and non-ischemic vein occlusion, which can provide further insight into cases of vein occlusion. Also, follow-up data collection interval was fixed, therefore, evaluation was not possible to be done at specific time points. So we recommend a longitudinal study encompassing all these posterior segment pathologies with larger number of cohorts in all sub-groups to further validate our findings. The major strength of the study is that it provides data on Indian subset of population, and all three major posterior segment pathologies responsible for causing macular edema were taken together into account.
Abbreviations:
BCVA best-corrected visual acuity
BRVO branch retinal vein occlusion
CFT central foveal thickness
DEX intravitreal dexamethasone
DME diabetic macular edema
ME macular edema
OCT optical coherence tomography
UME uveitic macular edema
References:
- Wolfensberger TJ, Gregor ZJ. Macular edema – rationale for therapy. Dev Ophthalmol. 2010; 47: 49–58.
- Kuppermann BD, Blumenkranz MS, Haller JA, Williams GA, Weinberg DV, Chou C et al. Randomized controlled study of an intravitreous dexamethasone drug delivery system in patients with persistent macular edema. Arch Ophthalmol. 2007; 125: 309–317.
- SaraoV, VerittiD, BosciaF, LanzettaP. Intravitreal steroids for the treatment of retinal diseases. Scientific World Journal, 2014 Jan 8; 2014: 989501.
- Hadayer A, Schaal S. Delivery of steroids into the eye for the treatment of macular edema.Expert Opin Drug Deliv. 2016 Aug; 13: 1083-91.
- Ozurdex (dexamethasone intravitreal implant 0.7 mg). [Product mono- graph]. Markham, ON, Canada; Allergan Inc.; 2015.
- WJ Mayer, A Wolf, M Kernt, Kook D, Kampik A, Ulbig M et al. Twelve month experience with Ozurdex for the treatment of macular edema associated with retinal vein occlusion. Eye 2013; 27: 816–822
- Lam WC, Albiani DA, Yoganathan P, Chen JC, Kherani A, Maberley DA et al. Real-world assessment of intravitreal dexamethasone implant (0.7 mg) in patients with macular edema: the CHROME study. Clin Ophthalmol. 2015 Jul 10; 9: 1255-68.
- Gillies MC, Lim LL, Campain A,Quin GJ, Salem W, Li J et al. A randomizedclinicaltrial of intravitrealbevacizumabversusintravitrealdexamethasone for diabeticmacularedema: the BEVORDEX study. Ophthalmology. 2014 Dec; 121: 2473-81.
- Chhablani J, Bansal P, Veritti D, Sambhana S, Sarao V, Pichi F et al. Dexamethasoneimplant in diabeticmacularedema in real-lifesituations. Eye (Lond). 2016 Mar; 30 : 426-30.
- Totan Y, Güler E, Gürağaç FB.Dexamethasone Intravitreal Implant for Chronic Diabetic Macular Edema Resistant to Intravitreal Bevacizumab Treatment.Curr Eye Res. 2016; 41: 107-13.
- Lowder C1, Belfort R Jr, Lightman S, Foster CS, Robinson MR, Schiffman RM et al. Ozurdex HURON Study Group.Dexamethasone intravitreal implant for noninfectious intermediate or posterior uveitis. Arch Ophthalmol. 2011 May; 129: 545-53. 12. Tomkins-Netzer O, Taylor SR, Bar A, Lula A, Yaganti S, Talat Let al. Treatment with repeat dexamethasone implants results in long-term disease control in eyes with noninfectious uveitis. Ophthalmology. 2014; 121: 1649–1654.
- Haller JA, Bandello F, Belfort R Jr, Blumenkranz MS, Gillies M, Heier J et al. Randomized, sham-controlled trial of dexamethasone intravitreal implant in patients with macular edema due to retinal vein occlusion. Ophthalmology. 2010; 117: 1134–1146.
- Lowder C, Belfort R Jr, Lightman S, Foster CS, Robinson MR, Schiffman RM et al. Dexamethasone intravitreal implant for noninfectious intermediate or posterior uveitis. Arch Ophthalmol. 2011; 129: 545–553. 15. Haller JA, Dugel P, Weinberg DV, Chou C, Whitcup SM et al. Evaluation of the safety and performance of an applicator for a novel intravitreal dexamethasone drug delivery system for the treatment of macular edema. Retina. 2009; 29: 46–51.
Figures:
Figure 1:Mean logMAR BCVA values for all posterior segment pathologies including DME, RVO, UME at baseline, 4 weeks, 12 weeks, 24 weeks
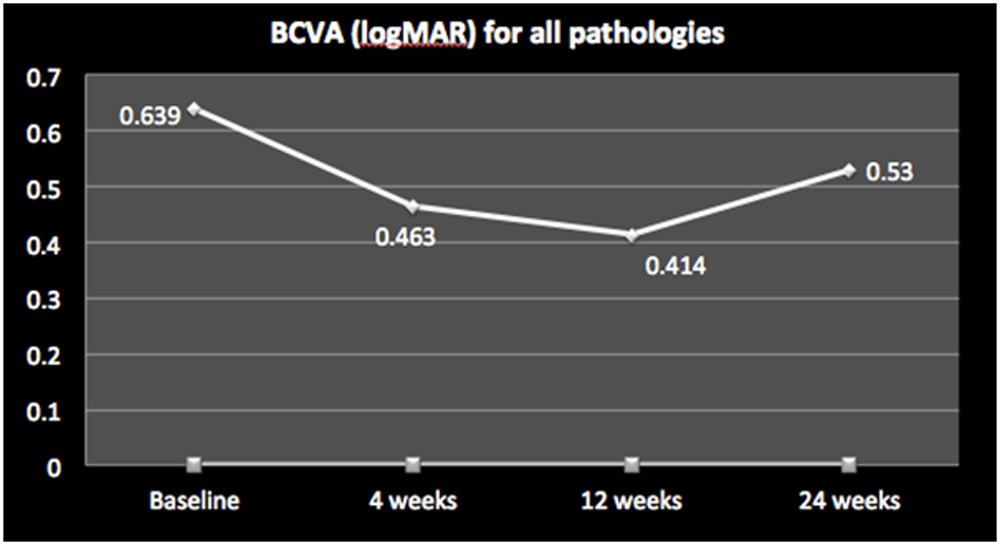
Figure 2:Mean logMAR BCVA values studied individually for DME, RVO, UME at baseline, 4 weeks, 12 weeks, 24 weeks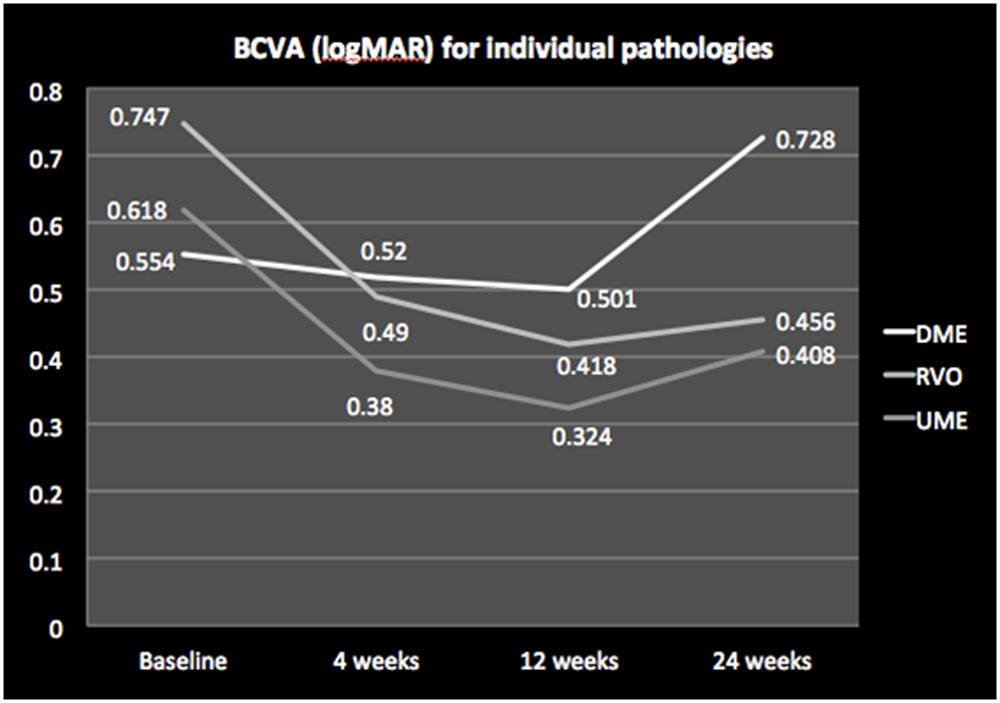
Figure 3:Mean CFT values for all posterior segment pathologies including DME, RVO, UME at baseline, 4 weeks, 12 weeks, 24 weeks
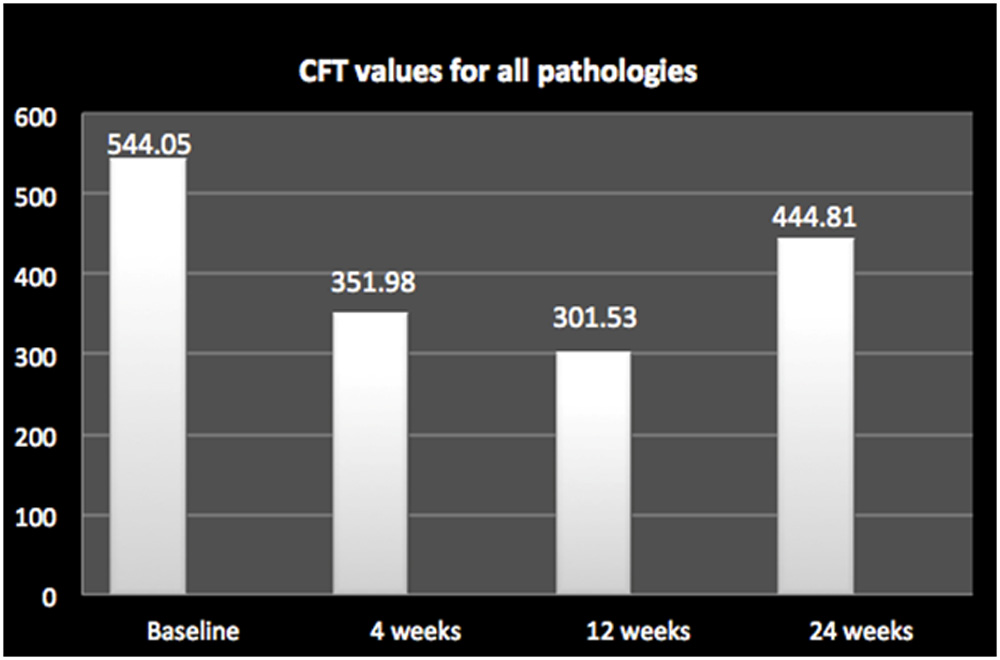
Figure 4:Mean CFT values studied individually for DME, RVO, UME at baseline, 4 weeks, 12 weeks, 24 weeks
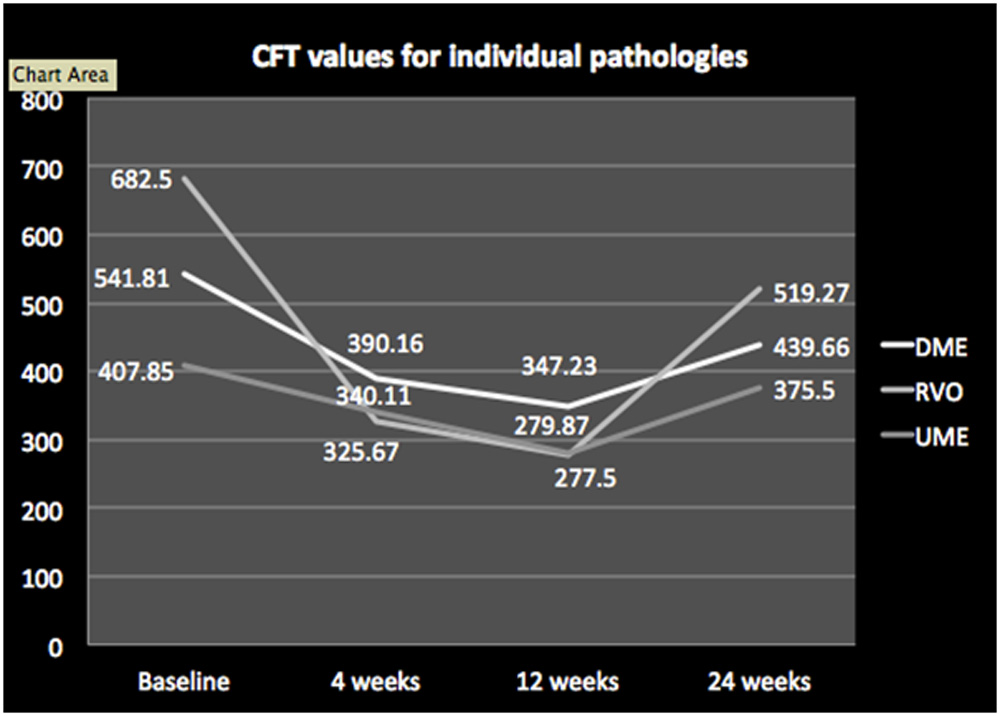
Figure 5: Distribution of patients on the basis of significant rise of IOP (>5mmHg) with cases studied together and individually at 4 weeks, 12 weeks and 24 weeks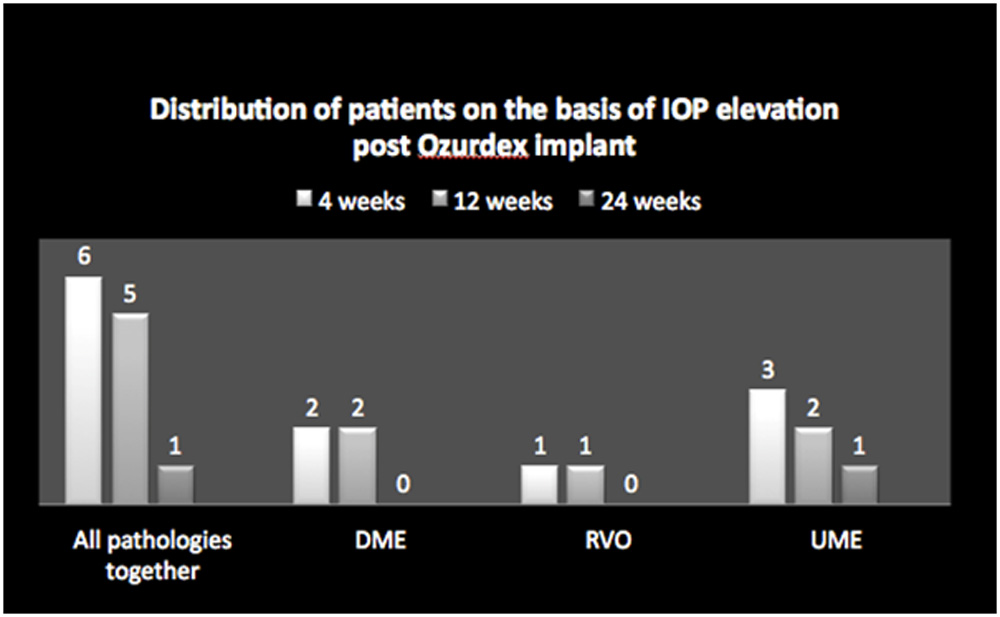
Figure 6:Distribution of Cataract in patients with cases studied together and individually at 4 weeks, 12 weeks and 24 weeks
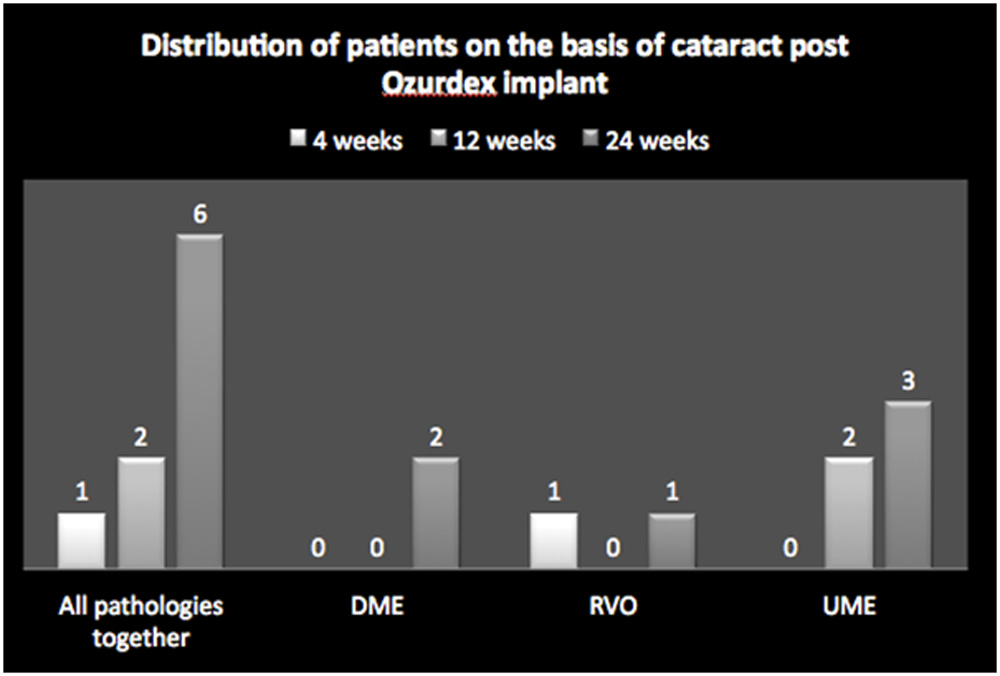
Figure 7:OCT retinal images from representative DME, BRVO, and uveitis study eyes at baseline and after treatment with Ozurdex at 12 weeks and at 24 weeks follow-up. BCVA and CFT values are mentioned.
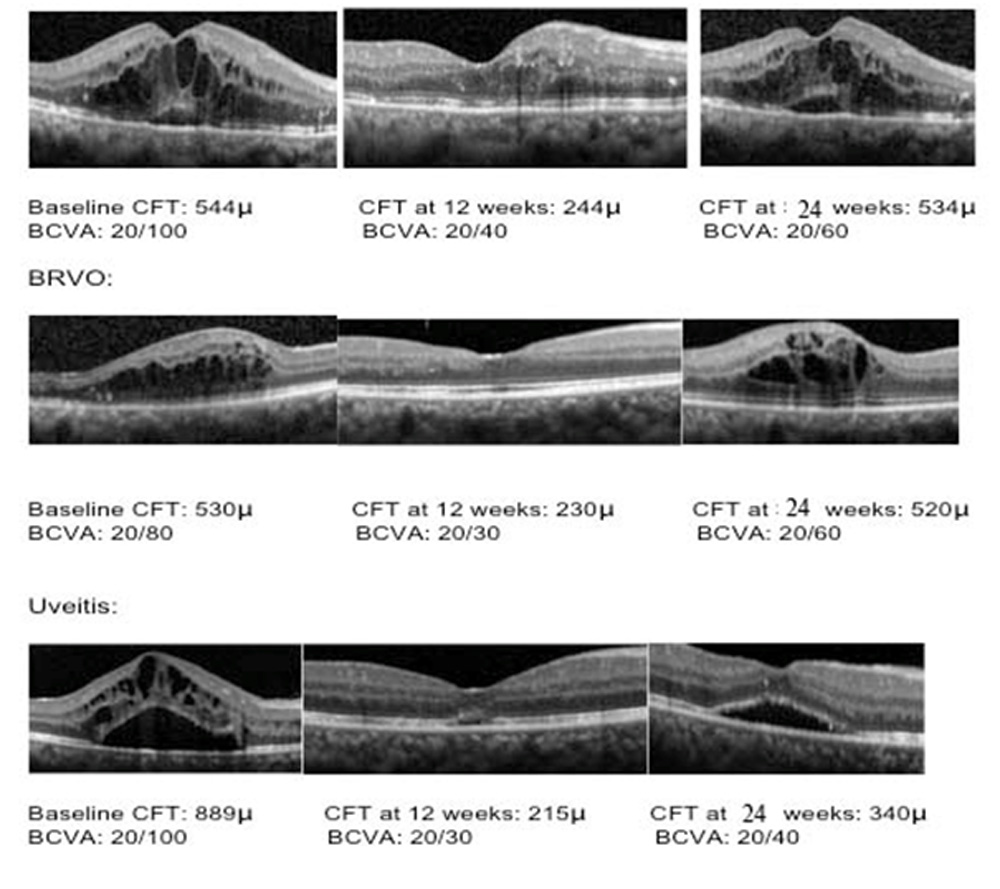
Table 1 Baseline demographics of patients treated with intravitreal dexamethasone implant injection
| Demographics | Study eyes
(N=116) |
| Age (in years)
Mean±SD Range |
50.2±21.9 21-83 |
|
Sex [N] (%)
Female Male |
Patients (N=104) 44 (42.3%) 60 (57.6%) |
|
Co-morbidities, [N] (%) Diabetes Hypertension |
Patients (N=104) 52 (50%) 39 (37.7%)
|
| Characteristics | Study eyes
(N=116) |
DME
(N=46) |
RVO
(N=40) |
UME
(N=30) |
|
Mean BCVA (logMAR) Mean±SD
|
0.636±0.4 |
.554±0.6 |
.744±0.7 |
.418±0.2 |
|
CFT (in microns)
|
527.8±210.1μm |
541.8±216.4μm |
682.5±240.2μm |
407.8±189.7μm |
|
IOP (in mmHg) |
15.3±3.8 |
14.21±3.10 |
13.3±2.8 |
18.2±4.1 |
| Lens Status:
Pseudophakic % (N) Phakic % (N) |
21(18.10%)
95 (81.89%) |
10 (8.62%)
36 (31.03%) |
4 (3.44%)
36 (31.03%) |
7 (6.03%)
23 (19.82%) |
Table 2 Baseline study eye characteristics
DME-diabetic macular edema; RVO-retinal vein occlusion; SD-standard deviation;
UME-uveitic macular edema; CFT-central foveal thickness; IOP-intraocular pressure;
BCVA-best corrected visual acuity
Table 3 Prior Intervention & treatment with Ozurdex implant
|
Parameters |
Study eyes
(N=116) |
DME
(N=46) |
RVO
(N=40) |
UME
(N=30) |
| Previous Interventions
Intravitreal Ranibizumab [N](%) Intravitreal bevacizumab [N](%) Posterior sub-tenon kenacort [N](%)
Lasers Focal [N](%) Grid [N](%) Pan retinal [N](%) |
6(5.17%)
11(9.48%)
3(2.58%)
1(0.862%) 4(3.448%) 14(12.06%) |
3(2.58%)
4 (3.44%)
–
0 0 11(9.48%) |
2(1.72%)
6(5.17%)
–
1(0.86%) 4(3.44%) 3(2.58%) |
1(0.86%)
1(0.86%)
3(2.58%)
0 0 0 |
|
No. of Injections Mean±SD
|
1.0±0.2 |
1.0±0.1 |
1.1±0.1 |
1.0±0.2 |
| Mean Duration of Ozurdex implant post primary intervevntion | 7.5 months | 7.3 months | 3.2 months | 13.5 months |
Table 4 Efficacy & Safety of Ozurdex implant in various posterior segment pathologies
| Parameters | Study eyes
(N=116) 4W 12W (p<0.05) 24W (p>0.05)
|
DME
(N=37) 4W 12W (p<0.05) 24W (p>0.05)
|
RVO
(N=34) 4W 12W (p<0.05) 24W (p>0.05)
|
UME
(N=28) 4W 12W (p<0.05) 24W (p>0.05)
|
|
Mean BCVA (logMAR) Mean±SD
|
.463±0.2 .414±0.5 .530±0.9 |
.520±0.1 .501±0.8 .728±0.3 |
.490±0.2 .418±0.4 .456±0.5 |
.380±0.1 .324±0.2 .408±0.7 |
|
CFT (in μm)
|
351.9±310.9
301.5±278.5 444.8±375.2 |
390.1±313.3
347.2±286.3 439.6±388.2 |
325.6±286.3
277.5±223.1 519.2±467.9 |
340.1±281.4
279.8±231.4 375.5±303.6 |
|
Cataract (N) |
1
2 6 |
0
0 2 |
1
0 1 |
0
2 3 |
|
Rise of IOP (N) (>5mmHg) |
6
5 1 |
2
2 0 |
1
1 0 |
3
2 1 |
|
Others (N) |
2
2 3 |
0
1 2 |
2
1 0 |
0
0 1 |
Abbreviations: p: p value; Others: Epi-retinal membrane (n=3), Vitreous Heamorrhage (n=2), Retinal Detachment (n=2)
Table Legends:
Table 1 Baseline demographics of patients treated with intravitreal dexamethasone implant injection
Table 2 Baseline study eye characteristics
Table 3 Prior Intervention & treatment with Ozurdex implant
Table 4 Efficacy & Safety of Ozurdex implant in various posterior segment pathologies
Leave a Comment