
Dr. Sumit Monga ( M10685 )
Abstract
Aim: To survey the management approach, regarding spectacle prescription in children,amongst members of Delhi Ophthalmological Society (DOS). Methods: A web-based, anonymous questionnaire (MCQs dealing with practical aspects of pediatric refraction), was send to available database. The survey responses (depicted in %) were compared using amount of pediatric clientele in one’s practice (group A: < 25 %, group B: 25% or more). The responses were also analysed in relation to the published concepts from literature. Results: 136 ophthalmologists (8.45 % response rate; 48% in group A), from the available database, responded to the survey. There were wide discrepancies in the responses (both, in and amongst, groups A and B; p > 0.05, chi square test), as to when and how much refractive error to prescribe in children, for a given situation. Conclusions: A wide gap exists between pediatric spectacle prescription patterns of ophthalmologists, as compared to the recommended paediatric ophthalmology protocols. The management approach, for certain situations concerning the paediatric refraction, was better amongst those with higher pediatric clientele.
Introduction: Pediatric refraction has its own unique challenges, viz. low cooperation of children, variable retinoscopy readings, amblyopia risk etc. One other factor, which complicates the issue, is the different interpretations of the same refractive errors, while prescribing in children, by the ophthalmologists. This article focusses on the latter issue.
Methods: Since spectacles, for children, are prescribed universally by allophthalmologists, we thought it was best to take their viewpoint, to understand theprevalent practice patterns. For the same, an online, anonymous survey questionnaire(https://www.surveymonkey.com/r/7NFQNV3) was sent to DOS members through email/social media. This survey included practical, commonly encountered situations,concerning pediatric refraction. All, ten questions of the survey had to be compulsorilyanswered by the respondent, before submission. Each question was multiple choicetype, with one of four responses, to be compulsorily, chosen. The survey assumes thatreliable refraction, using appropriate cycloplegics, has been done. The thrust was ondecision making approach: when and how do you prescribe for children, for a particular given refractive error? The responses (depicted in %) concerning the management of a particular refractive error, were noted. The appropriateness of the responses to case based situation (Question 3 to Question 9) were analysed, in relation to the recommended protocols, as per published literature. The responses were also segregated according to the amount of pediatric clientele in one’s practice (group A: < 25 %, group B: 25% or more), and compared, using Chi-square test.
Results and Discussion:
Till the last date of compilation of data, 136 ophthalmologists responded to the survey (8.45 % response rate, inspite of reminders). Of the respondents, 48 % were in group A (pediatric clientele <25%), possibly indicating general ophthalmology practice. The rest (group B) had varying pediatric patient clientele percentages (25-40% pediatric patients: 30% of respondents; 40-60% pediatric patients : 6% of respondents and >60% pediatric patients: 16% of respondents).
To the best of our knowledge, this is the first cross-sectional study highlighting descriptive data about the management approach of spectacle prescription in children, amongst Delhi ophthalmologists. This survey was a unique attempt to understand the prevalent practice patterns, regarding practical situations concerning paediatric refraction.
The results of the survey are being shared below, along with the discussion based on the concerned issue in the published literature.
Q1: What percentage of your practice are paediatric patients (overall)?
It was interesting to note that almost 79% of the responders were multi-specialty ophthalmologists (pediatric clientele less than 40%). “The proportion of pediatric patients seen” was taken as a criteria to understand the background of the responding ophthalmologists, as the label of “pediatric ophthalmology specialist” is vague in our country, due to lack of government recognized super-specialty fellowship programs
Q2: How are glasses, in children, prescribed at your set up?
In most cases (53%), the refraction was done by optometrists and prescribed by ophthalmologists. Interestingly, just over 1/3rd (34%) ophthalmologists, still did their own refractions and prescribe themselves. Only 7% of the responders would refer a refractive error case to their pediatric ophthalmologist colleague. The bottom-line is that ophthalmologist was the final decision maker in spectacle prescription in majority (94%) of cases.
Q3: 3 year old child cycloplegic refraction +1.5 Dsph/-0.5 Dcyl/180 degrees OU. The child had aligned eyes, normal anterior and posterior segments. What would you decide to do?
20 % of the responders would prescribe according to PMT, while 80% decided to manage the refractive error conservatively, at present. The latter seems justified on the basis of well, established principle of emmetropization, the process where the change in dimensions of the eye in the early years of life, effect in spontaneous regression of refractive errors. The American academy of pediatric ophthalmology and strabismus
(AAPOS) has devised evidence based spectacle prescription protocols for young children1 (Table 1). The bottom-line is that refractive error needs to be prescribed in children, only if amblyogenic enough.
Q4: 5 yr. old; unaided vision of 6/18p in RE and 6/12p in LE. The child had aligned eyes (on torch light), movements are full, normal anterior and posterior segments. Cycloplegic refraction reveals +4.5/-1.0/180 degrees OU. PMT:
+2.0/-0.5/180 OU (BCVA 6/12p OD, 6/9p OS).What would you do?
Majority (85%) would prescribe according to PMT response, and 1/3rd (30%) would start additional occlusion therapy for amblyopia, based on the documented asymmetric visual responses. On a careful review of the situation, we would realize that we are making lot of assumptions here. This child actually requires a careful cover test evaluation to rule subtle esophoria/esotropia, analysis to rule out any fixation preference and assessment of binocularity. If the child had an latent or manifest esodeviation, with one eye fixation preference (could be objectively assessed with vertical prism fixation test or a resistance to occlusion of the good eye, in case of dense amblyopia) with decreased binocular response (as judged by worth 4 dot test or titmus fly stereovision test), then the child would full cycloplegic correction, irrespective of child’s responses. If the child is indeed orthophoric for distance and near, on cover tests, with no fixation preference and good stereo acuity, the child would require spectacles after fogging on PMT (undercorrect hyperopia ny 1.5- 2.0 D). The child may also require initial cycloplegics for initial adaptation to glasses. As a corollary, high hyperopes (6D) also require full correction, due to their amblyopia potential. The learning pearl is that for significant hyperopic refractive errors, in addition to the visual responses, also appropriately evaluate accommodation, alignment status, fixation preference and binocularity, and then prescribe accordingly2. In case the same are not assessable in your setup, the help of a trained pediatric ophthalmologist should be taken (though only 13% had indicated in the survey that they would do so, for such a situation).
Q5: 8 yr. old comes with blurred vision OU since one week. Unaided vision 6/36 in
RE, 6/18p in LE. Dry acceptance: RE -5.5 Dsph (6/18p); LE -3.5 Dsph (6/12p).
Anterior and posterior segments are unremarkable; Aligned eyes (torch light);
Cycloplegic refraction show +0.25 Dsph OU. What would you do next?
About a fifth (21%) indicated their preference to prescribe the myopia, while almost half (48%) indicated their preference to re-refact the child under Atropine 1%. Just less than 1/3rd (31%) opined for using cycloplegics and transient bifocals in such a case.
To understand this situation, we should recollect the physiological process of accommodation. In the latter, when the ciliary muscles contract, the lens becomes more convex, thus shortening its focal length and we are able to focus on near objects. In the event of a persistent ciliary spasm, the increasing convexity of lens would remain and there would be induced myopia. This accommodative spasm would lead to pseudo-myopia, leading to blurring of vision for distance. Always consider this entity in a case of recent onset blurriness of vision with documented myopia with significant disparity in dry and wet refractions3. Careful evaluation may also reveal subtle esodeviation and miosis, in some cases. These cases indeed benefit with cycloplegic therapy (often require Atropine 1% for few weeks) along with bifocal spectacles for temporary use. With the increasing use of screen based devices for long hours, this entity is surely showing an increasingly trend.
Question 6: 6 yr. old girl; Unaided vision 6/36 OU; Aligned eyes, unremarkable
anterior and posterior segments. Cycloplegic refraction: +5.0 Dsph/-4.5 D cyl/180 degrees OU. PMT : +2.0 Dsph/-2.5 D cyl/180 degrees OU (BCVA 6/18p OU). Which of the following prescriptions would you agree with?
Results: PMT + Alternate eye patching (34%); +4.0 D sph/-4.5 Dcyl/180 (6/18 OU)
(35%); +3.5 Dsh/-3.5 Dcyl/180 (6/18 pOU) (12%); +2.0 Dsh/-3.5 Dcyl/180 (6/18 ppOU)
(19%)
Essentially, the debate here is between undercorrected astigmatism (65%) vs. full corrected astigmatic prescription (35%). It is imperative to understand that astigmatism (>2 D) is a potent stimulus for amblyopia, as unlike spherical errors, it is not neutralized
enough, by accommodation. Hence, unless we fully correct both meridians in astigmatism, we won’t be able to achieve the amelioration of amblyopia4. Interestingly, children are easily receptive to high astigmatic errors (upto 4.5 to 5.0 D), compared to adults, probably because children with such refractive errors are already amblyopic to begin with. If the child has symmetrical meridonial amblyopia (no preferential fixation), they tend catch up over time with just appropriate spectacles (alternate patching may not be required). Needless to say, that the cases with high astigmatic errors, also need to be evaluated to rule out corneal ectasia.
Question 7: 2 year old boy with pseudo strabismus. Cycloplegic refraction (Atropine 1 %) :OD +4.5 Dsph; OS +1.5 D sph. Anterior and posterior segments were unremarkable. What would you do?
About 1/3rd (35%) opted for conservative management (Would wait either for child up with a reliable visual response, or would prescribe only if squint develops or would just watch for stability of refraction over next year). While the others would go ahead and prescribe, evaluate for possible amblyopia and start occlusion.
It needs to be understood that anisometropia (especially anisohypermetropia) is another potent stimulus for amblyopia. In case of anisometropia, even the cutoff for spectacle prescription (as per the AAPOS guidelines)are lower than for symmetrical, isometropic refractive errors1. Also, there are objective methods to evaluate amblyopia (like the vertical prism fixation test, using 14 PD base down loose prism) in preverbal children. One need not necessarily wait for child’s visual responses alone; otherwise the unwarranted delay would lead to dense amblyopia, which would be tough to tackle at a higher age.
Q8: How do you monitor a child with refractive errors?
It was gratifying to see that overwhelming 99.9% monitor cases of refractive error, at follow up visits, with visual acuity, alignment evaluation and by checking their stereovision. If its’ indeed the case, it is an ideal situation and would help defeat the scourge of amblyopia.
Q 9: Who decides about the material and design of spectacles, in a child?
It was heartening to learn that almost 2/3rd of the responders (64%), participated in the spectacle making process, by indicating the nature of lenses and frame, to be made. In fact, all prescribing ophthalmologists should have a working knowledge about the same. Glass lenses are avoided in children, due to their obvious traumatic potential. CR39 lenses are the universally preferred. In case of one eye status of a child or a specific requirement for eye protection (e.g. contact sports), polycarbonate lenses are preferred (although they are costlier). Large aperture frames are preferable to avoid looking “over or under the frame”. Appropriate fitting and optical centration is extremely important in children, especially for astigmatism. Adjustable nose pads and elastic self-retainers (head bands) may be used. Rimless frames need to be avoided in children (again especially for astigmatism). Special situations require modifications, e.g. Use of high index lenses for high refractive errors, use of bifocal lenses in a case of high AC/A ratio, use of tinted lenses in cone dystrophies, etc4.
Q10: When should the first screening of refractive errors be done, in an asymptomatic child?
60% of the respondents, favour an age based refractive error screening (23 % would prefer at 6 months, while 37 % would screen at 3 yrs of age). A significant group (40%) would screen for refractive errors only when child is able to give a verbal response or if strabismus develops.The benefits of vision screening at an early age, has been well recognized5. However, many debate that a vision screening module tends to pick up children with only moderate or high refractive errors. To add to it, the lack of standard vision screening protocols and the lack of a consensus on a “safe” vision cut off, make the process vulnerable. Therefore, many researchers have raised the pitch for a combined refractive error screening at a young age. An integrated approach is obviously better5. However, it is easier said than done, as it needs trained personnel and resources, for an effective mass screening, which is lacking, at least, at present. Probably a start can be made in a limited, urban metropolitan setting like Delhi, if the government can make a refractive error screening certificate mandatory (by a qualified certified ophthalmologist) , for a child of 3 yr. old child, who is just joining school.
Needless to say, in the interim, that the whole ophthalmic community and medical professionals should keep on striving to keep on spreading awareness about early screening of refractive error in young children.
The amount of pediatric patients in one’s practice was used as a criteria to segregate responses, as the label of “pediatric ophthalmologist” is still vague in India, due to lack of recognised/standardised specialty fellowship/training programs and the mixed nature of ophthalmic practice, often tilting in favour of general ophthalmology. As is apparent from the survey, pediatric refraction was handled by ophthalmologists, with varying degrees of paediatric clientele. In fact, almost half (48%) were presumably general ophthalmologists (group A, <25% practice) and only a minority (16%) had major pediatric clientele (>60 % practice). Understandably, the responses of group B was better than group A, on some issues of pediatric refraction (management of pseudo myopia, high astigmatism and first screening of refractive error; Table 2). But, in both the groups, there were wide variations in the responses (Table 2). The latter suggests that there is a dire need to spread awareness on issues concerning paediatric refraction, amongst all group of ophthalmologists, irrespective of the amount of paediatric clientele in their practice.
The limitations of an online survey are well known6. The poor participation and small
sample size, which is what we saw in our series, limits the understanding of practice patterns of the community. In multiple choice format, the self reported response may vary from true practice patterns of the respondents. However, there were many positives,too, that this amateur exercise (survey) elicited. To the best of our knowledge, this is the first attempt, in India, to gather information on the important subject of pediatric refraction. Secondly, the model of the survey, using practical examples of paediatric refraction, helped us in gaining insights on practice patterns of Indian ophthalmologists and the same approach can, perhaps, be used as a teaching module to spread awareness on the subject.
Conclusion: The take home message is that for before prescribing any refractive error in a child, in addition to the visual response (subjective) , the objective parameters like
eye alignment, fixation preference, accommodative response, stereo acuity and overall visual need of the patient (asthenopia relief, alignment restoration, amblyopia potential of the refractive error), should also be checked. And above all, do not forget passion and patience. In case any treating ophthalmologist feels that they do not have the time, energy, skill or patience for examining all the details in a child, please feel free to refer the child to a trained pediatric ophthalmologist. After all, it is our moral obligation to ensure that future generation of tomorrow is amblyopia free.
Suggested reading
- Miller JM, Harvey EM. Spectacle prescribing recommendations of AAPOS members. J Pediatr Ophthalmol Strabismus 1998; 35:51-2.
- Associations between Hyperopia and other Vision and Refractive Error Characteristics. Optom Vis Sci. 2014 April; 91(4): 383–389.
- Goldstein J H etal. Spasm of the Near Reflex: A Spectrum of Anomalies. Sure Ophthalmol 40:269-278, 1996.
- Sainani A. Special considerations for prescription of glasses in children. J Clin Ophthalmol Res 2013; 1: 169-73.
- Sharma A, Congdon N, Patel M, Gilbert C (2012) School-based approaches to the correction of refractive error in children. Surv Ophthalmol 57: 272–283.
- Vaske Jerry J. Advantages and Disadvantages of Internet Surveys: Introduction to the special issue. Human Dimensions of Wildlife. 2011; 16(3): 149-53.
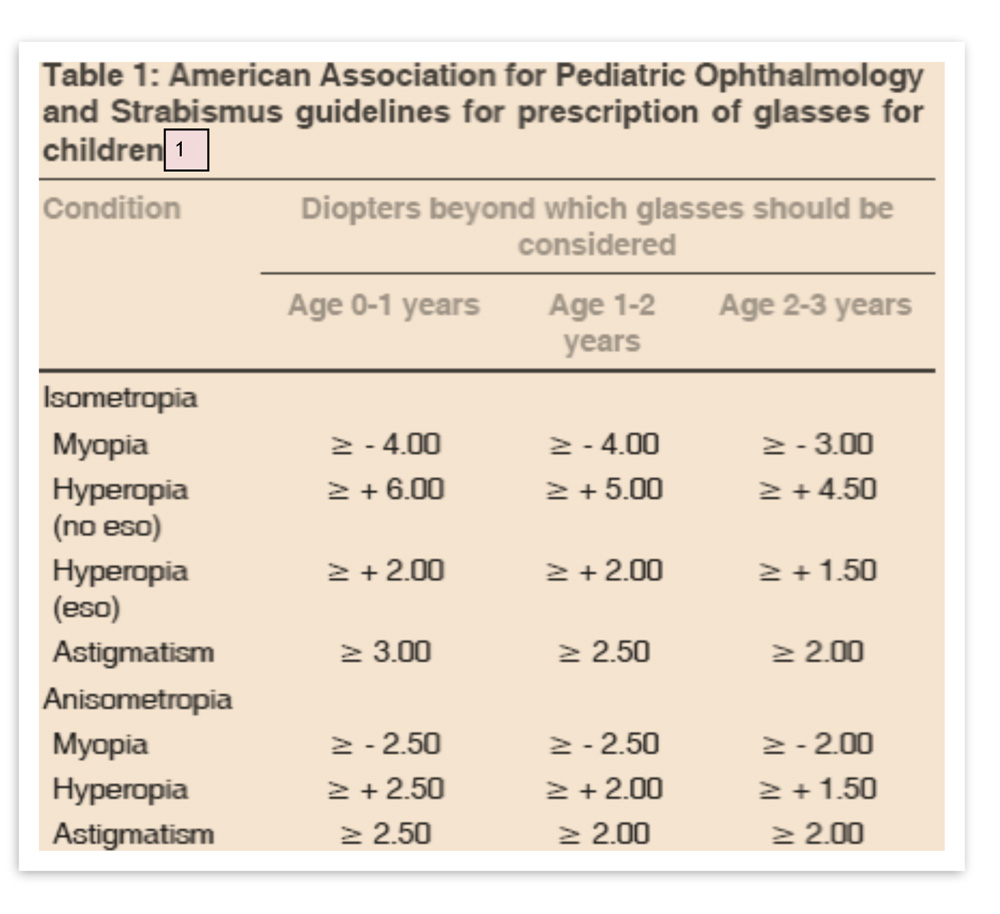
Table 2: Congruity of survey responses with desirable response and comparison of responses according to amount of paediatric clientele in practice
| Survey | Issue/Concept | Desired | Congruity | Group | Group B | p value |
| Q.No. | response, as | of survey | A | (Chi | ||
| per literature | responses | square | ||||
| with | test) | |||||
| desirable | ||||||
| response | ||||||
| 3 | Refractive error | Observe | 61% | 55/101 | 67/109 | 0.303 |
| within Normal range | ||||||
| 4 | Moderate | Pediatric | 12% | 15/101 | 5/109 | 0.011 |
| hyperopia Mgt | Ophthal R/v | |||||
| 5 | Pseudo myopia | Cycloplegia | 28% | 16/101 | 36/109 | 0.004 |
| and bifocals | ||||||
| 6 | High | Full | 35% | 27/101 | 45/109 | 0.026 |
| Cylindrical | Cylindrical | |||||
| errors | correction | |||||
| 7 | Anisometropia | Prescribe | 65% | 62/101 | 73/109 | 0.399 |
| and patch | ||||||
| 8 | Refractive | VA, | 99% | 98/101 | 104/109 | 0.541 |
| error monitoring | alignement, | |||||
| binocularity | ||||||
| 9 | First refractive | School joining | 48% | 28/101 | 52/109 | 0.004 |
| error screening in | Age (3-5 yrs) | |||||
| an | ||||||
| asymptomatic child |
Leave a Comment