

Dr. Anand Vinekar, V10089, Dr. Shetty Bhujang K, Dr. Chaitra Jayadev
![]()
![]()
Abstract:
Aim: To demonstrate the utility and impact of a novel online model for ROP training – “WISE-ROP”(Wide-field Imaging for Screening and Education of ROP)
Method: An indigenous, low-cost, high-impact, ROP training program was digitized (www.wiserop.com). The secure portal allowed trainees access to online course material, interactive video assessments and live mentor evaluation of imaging skills leading to certification based on the national guidelines. Cost impact compared to conventional training was assessed
Results: Non-physician trainees from remote centers with no other access to ROP training successfully executed and completed the courses. There was 85% reduction in overall training costs and 10:1 ‘time to train’ benefit
Conclusion: WISEROP is a unique model that can ‘create’ several imaging specialists for ROP screening in a short duration and at a lower cost compared to the conventional method. The program can help fill the void of screeners and improve access for rural infants
In India over 35 lakh babies born are premature annually, leading all nations worldwide in the number who are born and survive. With this burden, the prevalence and risk of blindness from Retinopathy of Prematurity (ROP) has also increased. India is a facing the global ‘third epidemic’ of ROP. A high birth rate, declining infant mortality, improved survival of low birth-weight babies and lack of uniform neonatal care, increases the vulnerability of these babies to blindness.
Until recently, ROP in India was reported and believed to exist only in urban neonatal units with an incidence between37- 54%. Our group has reported that rural and semi-urban centers in Karnataka have an incidence of ROP comparable to level 3 neonatal intensive care units (NICUs) of urban centers in the country. With fewer than 120 ROP specialists recently reported by the Indian ROP society who are trained to perform screening and appropriate laser treatment, there are millions of infants who are at risk of preventable blindness.
To address this lack of ROP screening service especially in the rural and outreach communities, our group developed a tele-ROP platform in 2007-2008, which continues to serve in rural and inaccessible areas of the South Indian state of Karnataka.Under this program, namely the Karnataka Internet Assisted Diagnosis of Retinopathy of Prematurity (KIDROP), non-physician ‘technicians’ travel to different rural and semi-urban neonatal units on a fixed time-table to perform ROP screening using digital imaging and the tele-ROP platform. The examinations are performed on-site, using a portable, wide field, digital retinal camera (Retcam Shuttle, Clarity MSI, USA or the Neo, Forus Health, Bangalore, India). The retinal images are uploaded on a secure, indigenous tele-ROP platform that is accessed by experts on their smart phones to provide real-time diagnosis.
The imagers have been hitherto trained using a validated program to not only image on site, but also to perform the first triage of diagnosis onsite itself to allow the result to be communicated to the rural mother or family so that appropriate counseling could be performed to allow better follow-up. The imagers are training is based on a 20 point score called the STAT score that has been previously published. The score and the process followed in KIDROP was validated by the Australian Government University in Perth using the Center for Disease Control (CDC) template in 2015 and has become the backbone of training scores of technicians, nurses, ophthalmic imagers and health care workers since.
With the availability of low-cost, indigenous, infant ROP cameras an increasing number of ‘adopters’ have created a new demand for trained, accredited and certified infant retinal imagers. However, the training takes 30,60 or 90 working days of on-site training with travelling of over 1000 kms in a week respectively to successfully complete Level I, II and III certification. With an increasing number of non-physicians requiring training in a short period of time, scaling this process was a challenge.
In this study we describe a novel, online training platform that was created to obviate the need for health care workers to travel to the city headquarters and to the outreach. The reduction in the duration of the training program, the efficacy of imparting theoretical and practical skill based learning and the cost benefit of such a program was evaluated.
Methods:
An online portal named “WISE-ROP”(Wide-field Imaging for Screening and Education of ROP), was created using a secure, internet based configuration. The portal provided secure access to registered users. Prior to registration, assessment and quality control measures were developed. The candidates were selected based on the program criteria for ROP imaging screeners. Each candidate is assigned a mentor from the team. The mentors are currently part of the KIDROP team, and will expand to other region wise mentors in phase 2.
The enrolled candidates had access to four courses. Course 1: ROP basics. These were divided into several units, which detailed basic anatomy, disease specific anatomy, ROP classification, ROP screening and management. Course 2: Telemedicine for ROP in India, ROP screening guidelines for India, age terminology and metrics, logistics and documentation of ROP Course 3: Understanding imaging, Imaging on the RetCam shuttle, Imaging on the Forus Neo camera and Course 4: Assessment of Image quality, Uploading of images on the WISEROP portal, training validation and accreditation.
Each course is divided into lessons. Each lesson has a self-assessment quiz and a mentor-assessed quiz after each course is completed. Candidates may progress to the next course only after successfully completing the exit exam of each course respectively.
Live Video based assessments are integrated on a “Google Hangout’ template that is securely embedded into the WISEROP platform. Mentors and candidates are engaged in a unique one-on-one scheduled video classroom. During these session, practical demonstration of skills, modification of imaging techniques, soft-skills imparting, remote hand-holding methods and rote-recall methods were developed.
In this pilot project, selected candidates underwent a 7-day onsite (at headquarters) orientation program. During this period, they underwent hand-holdingsessions on the retinal camera on mannequins and infants as per previously published protocols.
Post capture image processing, saving, reporting, uploading and archiving were also covered in the curriculum.
The time average duration for successful completion of the course were tabulated for the candidates and compared with profile matched candidates from the historical cohort who did not have online access. Direct and indirect costs incurred were tabulated for the course, travel and logistics and compared with historical data of the program when the entire training was performed on-site. International candidates using the portal were assessed using international monetary denominations consistent with their institute and job profiles.
The study was approved by the IRB of the institute and conforms to the Declaration of Helsinki. All patient information was anonymized. Only parents who consented for ROP screening using wide-field imaging were enrolled in this study.
Results:
Enrolled candidates were chosen from the voluntary Government centers under the KIDROP program and the non-governmental hospitals that have been beneficiaries of the program. These were ophthalmic assistants (3), optometrists (3), or ophthalmic imagers (3). In addition, sevenfemale staff nurses form government neonatal units were chosen after an orientation program where 55 nurses attended.Four international candidates were also enrolled in the pilot phase of the program.
The average duration of completing the course was 88 days (+/- 3.2 days) for Level III in the traditional method and 9.8 days (+/- 7.4 days) (p < 0.001) in those using WISEROP. The mean cost to company (CTC) was amortized to account for the currency, time period (when historical data was used) and the shared costs of the infrastructure, content creation, copyright costs, online data management costs, internet charges, travel allowances, dearness allowances (as per Government regulations), accommodation, consumables, resource person surveillance visits and faculty mentorship. There was 84.6% reduction in the cost of the training program using WISEROP compared to the historical conventional method.
Conclusion:
The key aspects of the WISEROP program are summarized:
- WISEROP is a novel, online, live training platform that addresses the scarcity of trained imaging specialists for Retinopathy of Prematurity management especially in underserved and rural centers
- The new gold standard of ROP screening is wide-field imaging. This has replaced the more traditional method of indirect ophthalmoscopy after the medico legal negligence judgment of the Hon, Supreme Court of India, in 2015.
- However, there is a gross deficiency of trained ROP specialists as well as trained and accredited imaging specialists or technicians.
- The KIDROP program has shown how non physicians may be trained to image for ROP in rural centers. The training is validated by the CDC guidelines and has been used in over 100,000 infant imaging sessions
- To train a ROP naïve non-physician to become a level 3 (highest status) imager, over 90 working days in the headquarters were necessary
- With WISEROP this is reduced to over 1/10th of the duration of the conventional method
- Besides, WISEROP allows training of candidates in their local milieu causing minimal disruption of the routines of these imagers
- WISEROP is over 85% less expensive than the conventional regime
- These advantages allow a greater number of non-physicians to be trained in a shorter duration of time.
- The impact of this would be felt as a ten fold increase in the number of trained imagers would lead to a compounding effect across the nation
- The program has also been piloted on international candidates and could be a source of health tourism and e-medicine commerce.
- WISEROP is the first online training program for ROP in the world and exploits the decade long program’s curriculum which provides theoretical and practical, skill based learning on a novel e-learning platform.
References:
- Howson CP, Kinney MV, Lawn JE. March of Dimes, PMNCH, Savethe Children, WHO. Born Too Soon: The Global Action Report onPreterm Birth. Geneva: World Health Organization; 2012.
- Gilbert C, Rahi J, Eckstein M, O’Sullivan J, Foster A. Retinopathyof prematurity in middle‑income countries. Lancet 1997;350:12‑4.
- Gilbert C, Fielder A, Gordillo L, Quinn G, Semiglia R, Visintin P, et al. Characteristics of infants with severe retinopathy ofprematurity in countries with low, moderate, and high levels ofdevelopment: Implications for screening programs. Pediatrics2005;115:e518‑25.
- Charan R, Dogra MR, Gupta A, Narang A. The incidence ofretinopathy of prematurity in a neonatal care unit. Indian JOphthalmol 1995;43:123‑6.
- Vinekar A, Dogra MR, Sangtam T, Narang A, Gupta A. Retinopathyof prematurity in Asian Indian babies weighing greater than1250 grams at birth: Ten year data from a tertiary care center in adeveloping country. Indian J Ophthalmol 2007;55:331‑6.
- Hungi B, Vinekar A, Datti N, Kariyappa P, Braganza S, Chinnaiah S,et al. Retinopathy of prematurity in a rural Neonatal IntensiveCare Unit in South India – A prospective study. Indian J Pediatr2012;79:911‑5.
- Vinekar A. IT‑enabled innovation to prevent infant blindness inrural India: The KIDROP experience. J Indian Bus Res 2011;3:98‑102.
- Vinekar A, Jayadev C, Mangalesh S, Shetty B, Vidyasagar D. Roleof tele‑medicine in retinopathy of prematurity screening in ruraloutreach centers in India – A report of 20,214 imaging sessions inthe KIDROP program. Semin Fetal Neonatal Med 2015;20:335‑45.
- Suryanarayana MH, Agrawal A, Prabhu KS. Inequality‑adjustedHuman Development Index for India’s States. India: UNDP; 2011.
- Vinekar A, Gilbert C, Dogra M, Kurian M, Shainesh G, Shetty B,et al. The KIDROP model of combining strategies for providing retinopathy of prematurity screening in underserved areas in Indiausing wide‑field imaging, tele‑medicine, non‑physician gradersand smart phone reporting. Indian J Ophthalmol 2014;62:41‑9.
- Dutta S, Raghuveer T, Vinekar A, Dogra MR. Can we stop thecurrent epidemic of blindness from retinopathy of prematurity?Indian Pediatr 2016;53 Suppl 2:S80‑4.
- Vinekar A, Avadhani K, Dogra M, Sharma P, Gilbert C, Braganza S,et al. A novel, low‑cost method of enrolling infants at risk forretinopathy of prematurity in centers with no screening program:The REDROP study. Ophthalmic Epidemiol 2012;19:317‑21.
- Vinekar A, Jayadev C, Bauer N. Need for telemedicine inretinopathy of prematurity in middle‑income countries: E‑ROPvs. KIDROP. JAMA Ophthalmol 2015;133:360‑1.
- Vinekar A, Avadhani K, Braganza S, Shetty B, Dogra M, Gilbert C.Outcomes of a protocol‑based management for zone 1 retinopathyof prematurity: The Indian twin cities ROP screening programreport number 2. Am J Ophthalmol 2011;152:712.
- Vinekar A, Jayadev C, Dogra M, Shetty B. Improving follow‑up ofinfants during retinopathy of prematurity screening in rural areas.Indian Pediatr 2016;53 Suppl 2:S151‑4.
- Vinekar A, Jayadev C, Mangalesh S, Kurian M, Dogra M, Bauer N,et al. Initiating retinopathy of prematurity screening beforedischarge from the neonatal care unit: Effect on enrolment in RuralIndia. Indian Pediatr 2016;53 Suppl 2:S107‑11.
- Supreme Court Judgement. Available from: https://www.supremecourtofindia.nic.in/FileServer/2015‑07‑02_1435823185.pdf[Last accessed on 2017 Mar 09].
- CDC. Developing an Effective Evaluation Report; 2013. Available from: https://www.cdc.gov/eval/materials/Developing-An‑Effective‑Evaluation‑Report_TAG508.pdf [Last ccessed on2017 Mar 09
- UNICEF. State of the World’s Children 2015 Country StatisticalInformation. UNICEF; 2015.
- Pejaver RK, Vinekar A, Bilagi A. National eonatology Foundation’sEvidence Based Clinical Practice Guidelines. Retinopathy ofPrematurity (NNF, India, Guidelines); 2010. p. 253‑62.
- World Health Organization. The Global Initiative for Eliminationof Avoidable Blindness. (WHO/PBL/97.61 Rev 1). Geneva: WorldHealth Organization; 1997.
- Government of India. Advance Estimates of National Income. PressInformation Bureau, Government of India; 2012‑2013.
- Blencowe H, Lawn JE, Vazquez T, Fielder A, Gilbert C.Preterm‑associated visual impairment and estimates of retinopathyof prematurity at regional and global levels for 2010. Pediatr Res2013;74 Suppl 1:35‑49.
- Early Treatment for Retinopathy of Prematurity CooperativeGroup. Revised indications for the treatment of retinopathy ofprematurity: Results of the early treatment for retinopathy ofprematurity randomized trial. Arch Ophthalmol 2003;121:1684‑94.
- Zin A, Gole GA. Retinopathy of prematurity‑incidence today. ClinPerinatol 2013;40:185‑200.
- Zepeda‑Romero LC, Gilbert C. Limitations in ROP programs in 32 Neonatal Intensive Care Units in five states in Mexico. BiomedRes Int 2015;2015:712624.
Figure 2: Screen shot of the WISEROP module of the lesson on Retinopathy of Prematurity (Basic). The dashboard on the right shows the completed and pending lessons in each course
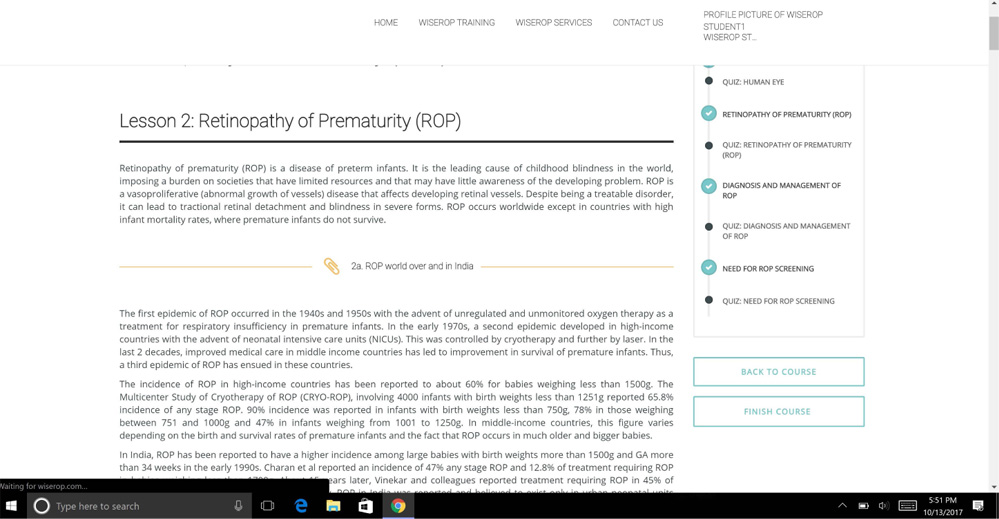
Figure 3: Dashboard of the WISEROP website. The candidate can schedule live video or mentoring sessions with the remote mentor. The event reflects on the calendar of the mentoring team.
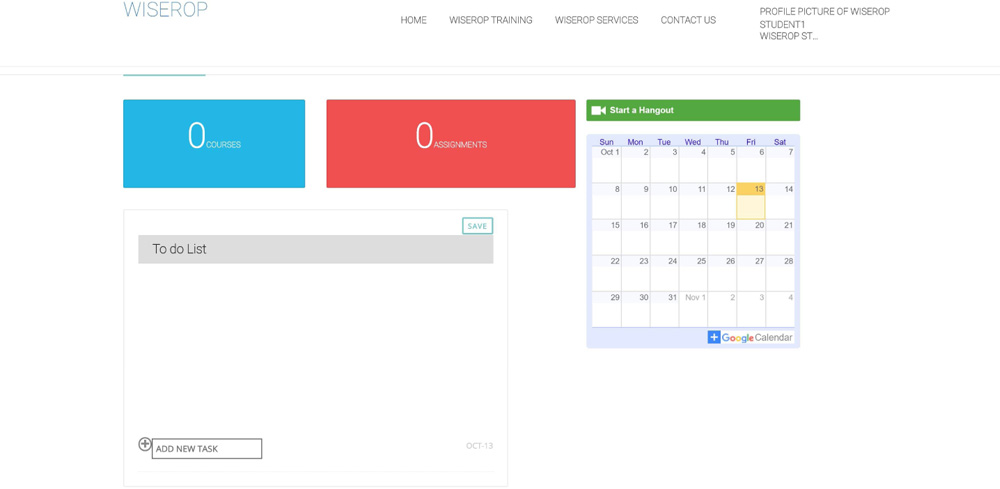
Figure 4: A screen capture of a live video based mentoring session. Candidates are remotely taught the technique of effective infant retinal imaging (for ROP) with special emphasis on image assessment and reporting.
Leave a Comment