

Dr. Lalgudi Ganesh Vaitheeswaran, V18501, Dr. Hema Malini M S, Dr. Mathew Kurian, Dr. Rohit Shetty
![]()
![]()
PURPOSE: To compare the ICL sizing obtained using WTW and ACD from Orbscan II, Lenstar, Nidek OPD scan III and Galilei and assess its impact on the predicted vault.
METHODS: The WTW and anterior chamber depth from Orbscan (Bausch & Lomb) were used to calculate the ICL size. The predicted vault was calculated from the UBM (Quantel Medical) machine and achieved vault measured by the AS OCT (Casia). In patients with normal predicted and achieved vaults, the ICL size was also calculated using the WTW from the Lenstar, Nidek OPD scan III and Galilei with the standard ACD from Orbscan and also their respective ACDs, except for Nidek OPD III scan. Predicted vaults in each situation was compared with the achieved vault.
RESULTS: 54 eyes (31 OD, 23 OS) of 54 patients underwent uneventful ICL implantation. The mean WTW from Orbscan was 11.56 +/- 0.35 mm, Lenstar was 12.16+/- 0.47 mm, Galilei was 12.02 +/- 0.35 mm and Nidek OPD scan III was 12.32+/- 0.44 mm. Mean ACD from Orbscan was 3.14+/- 0.18 mm, Lenstar was 3.66 +/- 0.19 mm, Galilei was 3.75 +/- 0.18 mm, UBM was 3.27+/- 0.19 mm. Using the ACD from Orbscan and WTW from the different devices, ICLs were oversized by 2 sizes compared to Orbscan in 5%, 11% and 18% of patients by Galilei, Lenstar and OPDIII scans respectively and the same was in 10% and 20% of patients by Galilei and Lenstar when their ACDs were also considered.
The mean preoperative predicted vault by Orbscan was 0.56+/- 0.11 mm, by Lenstar 0.70 +/-0.13 mm, by Nidek 0.71+/-0.12 mm, by Galilei 0.69+/-0.12 mm and the mean post-operative attained vault was 0.53 +/- 0.14mm.
CONCLUSIONS: ICL sizes by Lenstar, Nidek OPD scan III and Galilei were oversized significantly compared to the sizes calculated by the Orbscan and with higher predicted vaulting. In considerable patients, they were further oversized when the ACD from Lenstar and Galilei were used for calculation. These patients stand a significant risk of high vault and complications. A correction factor is needed to accurately calculate the appropriate ICL diameter.
Introduction:
The Implantable Collamer Lens (V4C) has been proven to be effective and approved by the FDA for the correction of moderate to high myopia (1). There are still reports on complications and requirement of exchange of ICLs owing to high or low vault and its associated problems as pupillary block, pigment dispersion or cataract formation. (2) Majority of these problems stem out of the inaccuracy in the sizing of the lens which is surrounded by the controversy of WTW or STS (sulcus to sulcus) as a guide to the sizing.
With several studies (3-8) comparing WTW or STS based methods for the ideal sizing and outcomes ruling in favour of neither of them as the single best method, meta-analysis has shown that comparison between WTW or STS based methods result in no clinically or statistically significant differences in the overall attained vault. (9)
While STS can be measured by UBM machine only, WTW and ACD are being measured by numerous machines available in market. The correlation between WTW and STS has been found to be weak by studies (4, 10). With STS still not approved by the FDA and widespread non-availability of UBM among refractive surgeons, the current search is towards instruments that can give the ideal WTW and ACD for estimating the ICL sizing with accuracy (11).
Among the instruments measuring WTW and ACD, studies have shown that the inter instrument variability is significant and they cannot be used interchangeably (12-14), but the amount of difference they generate in ICL sizing and its effect on the vault has not been studied to date. Some studies have shown the use of Orbscan II for WTW measurement to be safe and predictable for ICL size calculation and that other machines measure a higher WTW compared to Orbscan. But no method has been devised till date to calculate the WTW or ACD of a certain ideal device if the same parameters are known of another device. This could go a long way in helping refractive surgeons in low resource settings to be able to deliver safer outcomes in a larger number of patients (11).
Methodology:
Patients of high myopia with or without astigmatism willing for ICL/TICL implantation in the last 12 months were studied. All these patients underwent standard ICL sizing calculation using the WTW and ACD from Orbscan and keratometry, Pachymetry from Pentacam. Cycloplegic refraction and subjective acceptance was used to calculate the amount of refractive error to be corrected. UBM (Quantel Medical) was also done routinely to estimate the mean STS and predict the post-operative vault based on the ICL simulator software for the ICL size obtained (using STAAR ICL calculator). Post operatively, the attained vault was measured using the swept source based (Casia) ASOCT.
These patients, in addition to the routine work up, were subjected pre-operatively to WTW and ACD measurements using the Lenstar 900, Galilei G4 and Nidek OPD III scan systems. All these devices automatically calculate these variables and hence there is no subjective difference between two different operators.
Post operatively, for all those patients who had a normal predicted and attained vaults (range of 250-750 micron), the ICL size was calculated with the WTW obtained from each of the other devices (Lenstar 900, Galilei G4 and Nidek OPD III scan) using the online standard calculator. In the first step, the ACD from Orbscan was used with only variable being WTW and in the next step, ACD was also taken from the individual devices (except Nidek OPDIII scan) along with the WTW from the respective devices for ICL size calculation. The predicted vaults were also measured for the ICL sizes obtained using the ICL simulation method in the UBM done pre-operatively.
All the data including the refractive error corrected, age of patients, WTW and ACD from each of the devices studied, STS, ICL sizes obtained using each of the above-mentioned methods were entered and analysed using MedCalc. Software.
Results:
54 eyes (31 OD, 23 OS) of 54 patients were included in the study. The Average age of patients studied was 29.35+/- 5.21 years (Range: 23- 42 years). The mean spherical equivalent corrected was 13.18 +/- 4.3 DS with 49 requiring Toric ICLs and remaining non toric ICLs. The mean WTW from Orbscan was 11.54+/-0.34 mm and the mean STS measured was 11.54+/- 0.49 mm. The mean ACD used from Orbscan was 3.15+/-0.19 mm. The WTW measured from the four devices showed significant difference with highest being that of Nidek OPDIII scan followed by Lenstar, Galilei and Orbscan, in that order (Table 1).
Table 1: Comparison of WTW between the devices studied (Mean, SEM and 95% confidence intervals are mentioned)
| Factor | Mean | Std. Error | 95% CI |
| WTW Galilei | 12.0073 | 0.04672 | 11.9136 to 12.1009 |
| WTW Lenstar | 12.1253 | 0.05833 | 12.0083 to 12.2422 |
| WTW OPD scan III | 12.2944 | 0.05925 | 12.1756 to 12.4132 |
| WTW Orbscan | 11.5389 | 0.04557 | 11.4475 to 11.6303 |
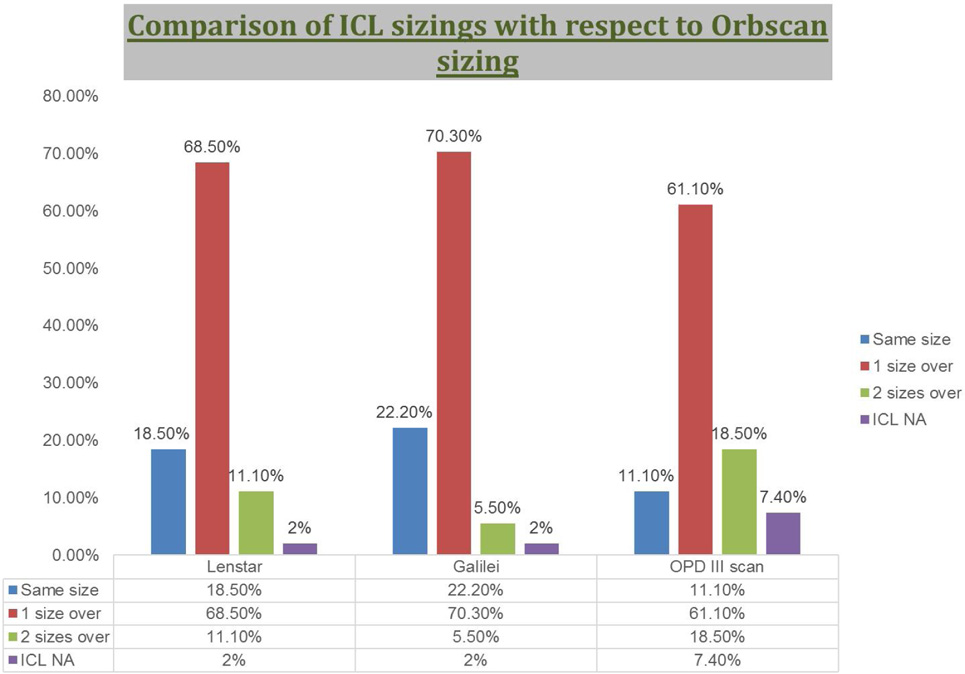
The impact of the above differences in WTW on ICL sizing with respect to sizing based on Orbscan WTW were studied. The sizes obtained by all the three devices were oversized in most of the eyes, with only around 20% of eyes having the same size as obtained by Orbscan WTW and ACD. The maximum number of eyes significantly over sized (by 2 sizes) was with Nidek OPD III scan followed by Lenstar and Galilei. ICLs were oversized by 2 sizes compared to Orbscan in 5%, 11% and 18% of patients by Galilei, Lenstar and OPDIII scans respectively (Figure 1).
Figure 1: Shows the comparison of ICL sizes obtained using other machines WTW alone with that of Orbscan.
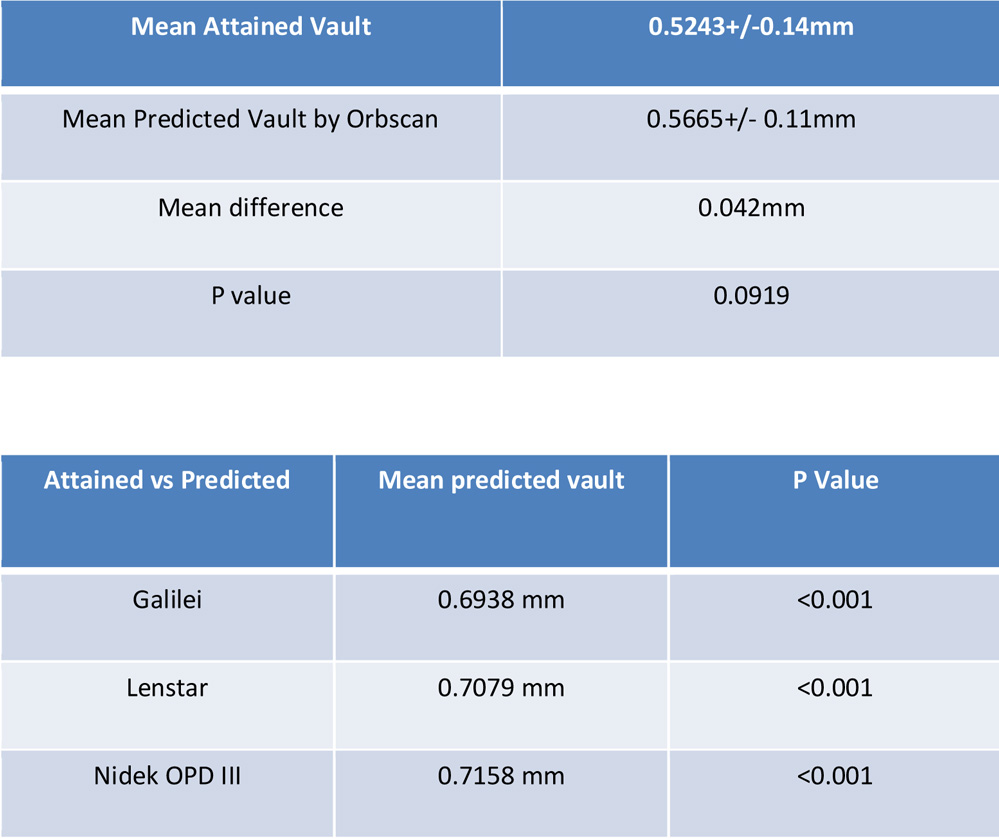
The means of predicted vault (based on UBM) by each of the devices were compared with the attained vault (measured by Casia ASOCT) and the distribution of the predicted vaults were also studied. The attained vault differed significantly (p<0.05) with the predicted vaults of all the devices except that of Orbscan (p=0.09). (Table 2a, 2b)
Table 2a, 2b: Comparison of means of attained vault with the means of predicted vault based on Orbscan WTW and with other devices WTW
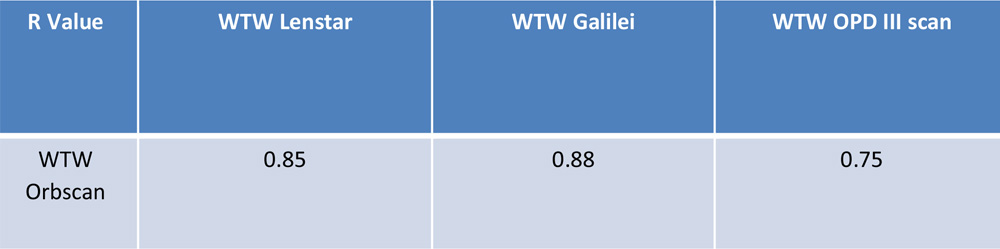
The WTW between devices were correlated to that of Orbscan WTW using parametric tests of correlation (Pearson) and the correlation was found to be significant (Table 3).
Table 3: Shows the strength of correlation between the WTW of devices studied with that of Orbscan WTW
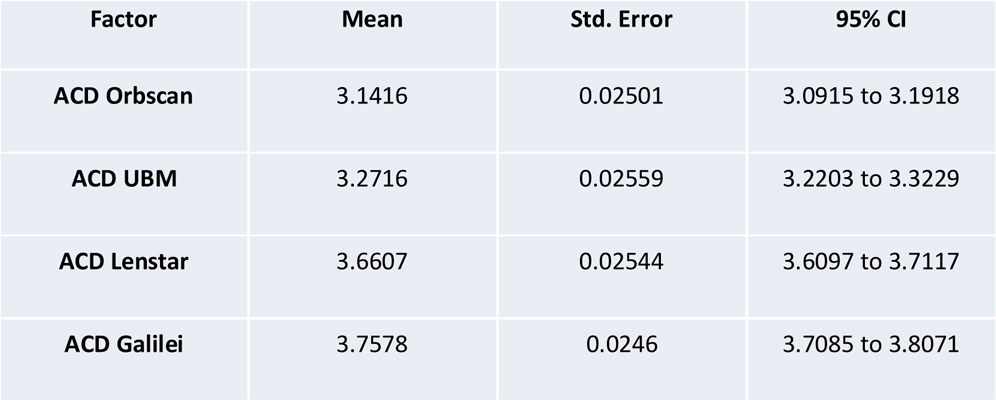
The ACD obtained using the devices used in the study were analysed (Table 4) and the impact of using the ACD from Lenstar, Galilei and Orbscan along with the WTW from the same machines on ICL sizing was studied.
Table 4: Comparison of ACD between the devices studied (Mean, SEM and 95% confidence intervals are mentioned)
When the ACDs of Lenstar and Galilei were used along with their respective WTWs, 20% and 10% of eyes respectively were two sizes oversized compared to Orbscan sizing for the same eyes. These values are double of the percentages of two sizes oversizing when the ACD from Orbscan was used
Discussion:
WTW and ACD are two important variables in the ICL size calculation and there are several machines which provide automated measurements of the same. Manual measurements are not as repeatable as automated measurements(15).
The measurements of WTW and ACD have been compared between devices in a few studies. A comparative study between Pentacam and IOL master revealed that Pentacam measured significantly higher ACD and lesser WTW compared to IOL Master(14).
A study by Salouti et al (12) showed that Orbscan WTW was significantly lesser in comparison to that of Pentacam and they should not be used interchangeably. Another study (13) by the same group has compared Orbscan with that of EyeSys and Galilei systems and concluded that Orbscan WTW was significantly lesser than that of the other two and WTW of Galilei was closer to Orbscan WTW. Kiraly et al (16) among other devices compared Orbscan II WTW with that of IOL master and showed that Orbscan WTW was significantly lesser than IOL Master WTW.
The results of our study have been similar in that Orbscan WTW has been the least followed by Galilei, Lenstar and Nidek OPD III scan in the same order. There is no study till date which has suggested which among the devices is better for WTW measurement and how much these differences lead to a change in the ICL sizing.
In our study, the comparison of mean pre-operative predicted vaults with that of post-operative attained vaults revealed that among all the devices studied, Orbscan mean predicted vault was closest to the ideal vault suggesting the use of Orbscan WTW for better outcomes. A study by Cao et al using Orbscan had similarly good outcomes with vault in most of their patients(17). When the sizing of ICL obtained with WTW from other devices were compared with the size that gave the patients a normal vault (calculated based on Orbscan WTW), we noticed that up to 20% patients would have been oversized by 2 sizes and another 50-60% by one size. This means that a significant number of patients would have had high vaults and possibility of complications had WTW been used from the other devices studied. This hypothetical ICL size calculation, when done also considering the ACD derived from these devices instead of Orbscan ACD showed more oversizing than just considering their WTW along with Orbscan ACD.
This is the first study to show the rate of “significant oversizing of ICL size” with the differences in the WTW and ACD between the devices, which were known to occur even before.
In the current scenario where there is no clear protocol of using either the STS or WTW for ICL sizing and meta-analysis showing equivalent outcomes with the use of either of them, it becomes more important to understand the technical differences between the various machines derived WTW and ACD and how much of change they can lead to in the sizing of the ICL and in turn the vaulting.
Conclusion:
This study conclusively proves that the WTW and ACD derived from the machines Orbscan, Galilei, Lenstar and Nidek OPD III scan are not at all interchangeable. The use of Orbscan WTW and ACD provided ideal mean predicted vaults and attained vaults in our patients and the hypothetical use of other machines can lead to a significant oversizing of the phakic intra ocular lenses and risk of complications. Correction factors are necessary to overcome this factor in order to attain vaults close to ideal vaults in our patients when using different devices for WTW/ACD measurements.
References:
- Packer M. Meta-analysis and review: effectiveness, safety, and central port design of the intraocular collamer lens. Clinical Ophthalmology (Auckland, NZ). 2016;10:1059-77.
- Khalifa YM, Goldsmith J, Moshirfar M. Bilateral explantation of Visian Implantable Collamer Lenses secondary to bilateral acute angle closure resulting from a non-pupillary block mechanism. J Refract Surg. 2010;26(12):991-4.
- Choi KH, Chung SE, Chung TY, Chung ES. Ultrasound biomicroscopy for determining visian implantable contact lens length in phakic IOL implantation. J Refract Surg. 2007;23(4):362-7.
- Gao J, Liao RF. [Correlation between white-to-white diameter and ciliary sulcus diameter of high myopia eyes]. [Zhonghua yan ke za zhi] Chinese journal of ophthalmology. 2013;49(7):627-32.
- Reinstein DZ, Lovisolo CF, Archer TJ, Gobbe M. Comparison of postoperative vault height predictability using white-to-white or sulcus diameter-based sizing for the visian implantable collamer lens. J Refract Surg. 2013;29(1):30-5.
- Biermann J, Bredow L, Boehringer D, Reinhard T. Evaluation of ciliary sulcus diameter using ultrasound biomicroscopy in emmetropic eyes and myopic eyes. J Cataract Refract Surg. 2011;37(9):1686-93.
- Guber I, Bergin C, Perritaz S, Majo F. Correcting Interdevice Bias of Horizontal White-to-White and Sulcus-to-Sulcus Measures Used for Implantable Collamer Lens Sizing. Am J Ophthalmol. 2016;161:116-25.e1.
- Kojima T, Yokoyama S, Ito M, Horai R, Hara S, Nakamura T, et al. Optimization of an implantable collamer lens sizing method using high-frequency ultrasound biomicroscopy. Am J Ophthalmol. 2012;153(4):632-7, 7.e1.
- Packer M. Meta-analysis and review: effectiveness, safety, and central port design of the intraocular collamer lens. Clin Ophthalmol. 2016;10:1059-77.
- Reinstein DZ, Archer TJ, Silverman RH, Rondeau MJ, Coleman DJ. Correlation of Anterior Chamber Angle and Ciliary Sulcus Diameters With White-to-White Corneal Diameter in High Myopes Using Artemis VHF Digital Ultrasound. J Refract Surg. 2009;25(2):185-94.
- Domínguez-Vicent A, Pérez-Vives C, Ferrer-Blasco T, García-Lázaro S, Montés-Micó R. Device interchangeability on anterior chamber depth and white-to-white measurements: a thorough literature review. International Journal of Ophthalmology. 2016;9(7):1057-65.
- Salouti R, Nowroozzadeh MH, Zamani M, Ghoreyshi M, Khodaman AR. Comparison of Horizontal corneal diameter measurements using the Orbscan IIz and Pentacam HR systems. Cornea. 2013;32(11):1460-4.
- Salouti R, Nowroozzadeh MH, Zamani M, Ghoreyshi M, Salouti R. Comparison of horizontal corneal diameter measurements using Galilei, EyeSys and Orbscan II systems. Clin Exp Optom. 2009;92(5):429-33.
- Sayed KM, Alsamman AH. Interchangeability between Pentacam and IOLMaster in phakic intraocular lens calculation. European journal of ophthalmology. 2015;25(3):202-7.
- Baumeister M, Terzi E, Ekici Y, Kohnen T. Comparison of manual and automated methods to determine horizontal corneal diameter. J Cataract Refract Surg. 2004;30(2):374-80.
- Kiraly L, Duncker G. [Biometry of the anterior eye segment for implantation of phakic anterior chamber lenses. A comparison of current measurement devices]. Ophthalmologe. 2012;109(3):242-9.
- Cao XF, Wang Y, Shen Y, Tong JP, Xia JH, Zhou TA, et al. [Selection of the posterior chamber phakic intraocular lens length]. [Zhonghua yan ke za zhi] Chinese journal of ophthalmology. 2013;49(3):235-41.
Leave a Comment