

Dr. Dipankar Das, D08987, Dr. Deepika Kapoor, Dr. Jayanta Kumar Das, Dr. Kasturi Bhattacharjee
![]()
![]()
Introduction: Non-specific orbital inflammation affects orbital tissue including fats, lacrimal glands, extraocular muscles etc focally or diffusely.1,2,3,4 Affection of Tenon’s capsule is the least frequent location.2,3,4 Incidence and prevalence findings of non-specific inflammatory disease of orbitbased on scientific literature was very difficult as it depended on inclusion or not of specific and non-specific inflammatory pathologies.3, 4, 5, 6, 7, 8
Aim: To present histopathological analysis of idiopathic inflammatory disease of orbit and ocular adnexa
Methods: Design-A retrospective laboratory based study.
The study was carried out in an ocular pathology laboratory in a tertiary institute of northeast India where analysis of 93 cases were done in 5 years between 2011 and 2016. Routine haematoxylin eosin and other special stains were done for the diagnoses. Immunohistochemistry (IHC) panel were also carried out. For infectious pathology,Grocott’smethenamine silver (GMS) stain for fungus, tissue Gram’s stain for bacteria’s and acid fast stains for tubercular bacilli were done. IHC panels were done for CD 20 (B-cells), CD-3 (T-cells), CD-45 (Leucocyte common antigen, LCA), BCL-2, CD-138 (Plasma cells), Kappa, Lambda, IgG4 in tissue, IgG 4 in serum etc. IHCs were done using kit methods (Standardized) and adequate controls were taken for each sample.
Results: 93 cases (6.64%) of non specific orbital inflammation were reported out of 1467 specimens (Figure 1). Orbital pseudotumors (IOID) were seen in 27 cases (sclerosing variety-6); benign lymphoid hyperplasias in two cases; reactive lymphoid hyperplasias in 10 cases; plasma lympho-proliferative reactive lesions in four cases ; IgG4 related disease in one case; non- specific inflammatory reactions (conjunctiva, sclera and lid) in 49 cases (Figure 2). In all the diagnoses, Infections and lymphomas were excluded.
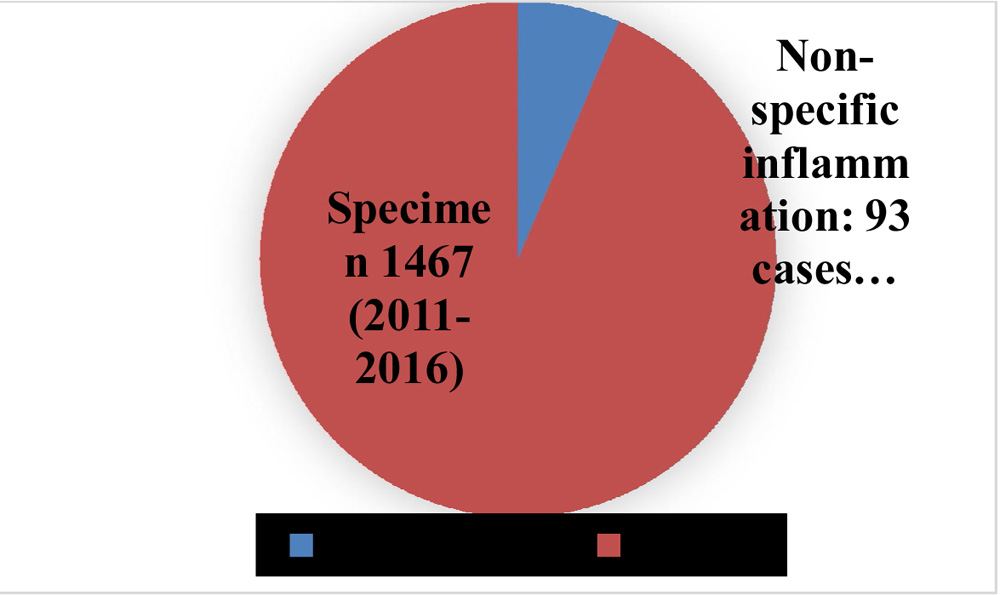
Figure 1. Graph showing non-specific orbital inflammatory cases in respect to total cases received in the ocular pathology laboratory during 2011-2016
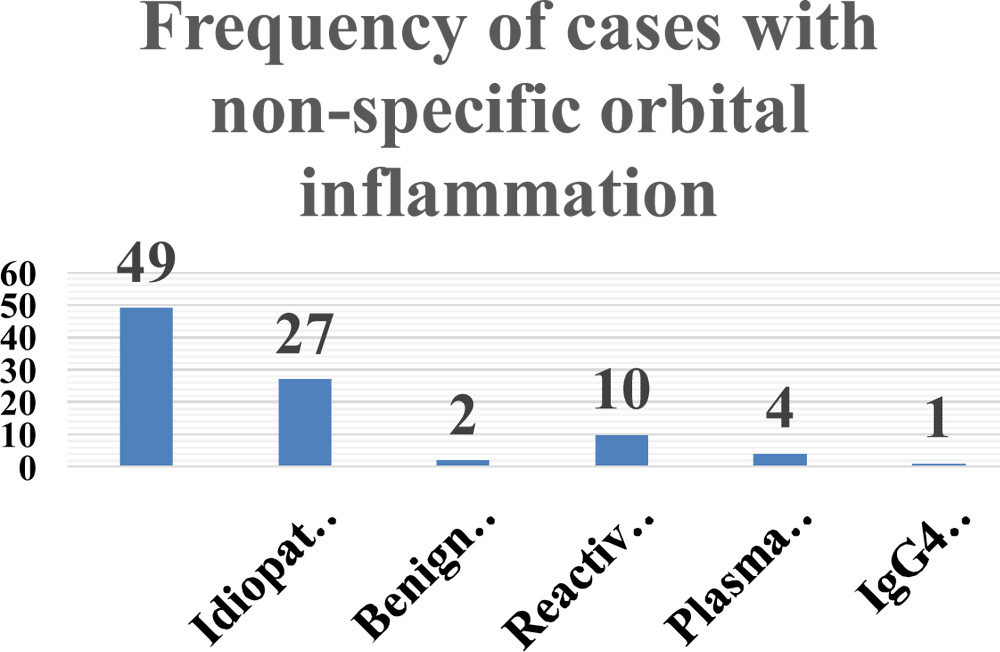
Figure 2: Distribution of Inflammatory disorders of orbit
Discussions: Pathology of typical non-specific orbital inflammation were characterized by cellular infiltrate, vascular congested tissues, altered lacrimal gland tissue and disturbances in other orbital structures.1,2,3,4 Grossly, the lesions displayed greyish white coloured tissues and microscopically, it revealed inflammation in the orbital structures and cellular infiltrates that were focal, multifocal or diffuse.3,4 Cellular infiltrations were of differentiated mature lymphocytes, intermixed with plasma cells, eosinophils, polymorphs and rarely with histiocytes and macrophages.1,2,3,4,5 The infiltrates were polyclonal and lymphoid follicles could be seen with germinal centres occasionally. The lesions were highly vascular due to capillary proliferations and were accompanied with perivascular and lympho-plasmacyticinfiltrations and eosinophils were sometimes seen tracing near capillary adventitia.1,2 Endothelial cells showed hyperplasia and sometimes there were reactive increase in the number of cells. In some long standing cases, sclerosing patterns were noticed andperiductalfibrosis in lacrimal tissue with atrophied acini were seen.1, 2, 3, 4, 5
We had seen 93 cases (6.64%) of non specific inflammation were reported out of 1467 specimens. IOID were seen in 27 cases (sclerosing variety-6 cases), Benign lymphoid hyperplasias in two cases Reactive lymphoid hyperplasias in 10 cases, Plasma lympho-proliferative reactive lesions in four cases, IgG4 related disease in one case, non specific inflammatory reactions (conjunctiva, sclera and lid) in 49 cases (Figure 2). In all the diagnoses, Infections and lymphoma were excluded from the cohort.
Moreiras and Prada et al. studied 189 cases of non-infectious inflammatory disorders (specific and non-specific) and found an incidence of 12.8 % among orbital lesions excluding thyroid orbitopathy.1, 7Pseudotumours or non-specific inflammations were frequently diffuse variety in 30 cases, anterior in 20 cases, dacryoadenitis in 26 cases and myositis in 24 cases.1,4,6,7,9 Our histopathological cases in the study were 6.64% which was almost half the above mentioned study.7
Conclusion: Biopsy supported study on non specific orbital inflammation was important to know the pattern. Further, larger multicentre studies will give better insight on the clinico-pathological aspect of this inflammatory orbital disease.
Acknowledgements:
Dr. Panna Deka, Co-Pathologist, Sri Sankaradeva Nethralaya (SSN), Guwahati, India
Mr. ApurbaDeka, Technician, Ocular Pathology Lab, SSN, Guwahati, India
References:
- Blodi FC. Orbital inflammation. Orbit 1982, 44: 1-19
- Garner A. Pathology of pseudotumour of the orbit: a review. J ClinPathol. 1973; 26: 639-648
- Chavis RM, Garner A, Wright JE. Inflammatory orbital pseudotumour. A clinicopathologic study. Arch Ophthalmol 1978; 96: 1817-1822
- Hara Y, Ohnishi Y. Orbital inflammatory pseudotumour: clinicopathologic study of 22 cases. Jpn J Ophthalmol 1983;27: 80-89
- Nguyen QD, Arbour J, et al. Sclerosing inflammatory pseudotumour of the eye. Arch Ophthalmol 2001; 119: 279-290
- Kennerdell JS, Dresner SC. Non-specific orbital inflammatory syndromes. Surv Ophthalmol 1984;29:93-103
- JVP Moreiras, MC Prada Text book of Orbit, Vol 1, High lights of Ophthalmology, ISBN: 9962-613-22-1
- Plaza JA, Garrity JA, Dogan A, Ananthamurthy A, Witzig TE, Salomao DR. Orbital inflammation with IgG4- positive plasma cells: manifestations of IgG4 systemic disease. Arch Ophthalmol 2011; 129(4): 421-428.
- Sato Y, Ohshima K, Ichimura K, Sato M, Yamdori I, Tanaka T et al. Ocular adnexal IgG4-related disease has uniform clinicopathology. Pathol Int.2008; 58(8):465-470
Leave a Comment