

Dr. Deepti P, D14106, Dr. Krishna Prasad R
![]()
![]()
ABSTRACT
Purpose- Loop myopexy of superior rectus with lateral rectus is a well established surgical treatment of myopic strabismus fixus. We evaluated safety profile and surgical outcomes of a novel modification of loop myopexy with silicon tube sling (used for ptosis surgery).
Methods-It was a prospective interventional study. 19 eyes of ten patients with myopic strabismus fixus who presented to our OPD from January 2015 to June 2016 were surgically treated with silicone tube loop myopexy of superior rectus and lateral rectus. All eyes underwent additional medial rectus (MR) recession for varying grade. They were all followed up for 12 months post surgery. Pre and post operative horizontal deviation, vertical deviation and extraocular movements were recorded.Individual age, sex, duration of squint, visual acuity, refractive status, axial length, any previous squint operations, and associated complications were all noted. Myopic strabismus fixus due to causes other than myopia were excluded.
Results- At the last follow-up,mean esotropia improved to 11.6+/-7.1 prism dioptre (PD) from78.7=/-6.4 prism dioptre, p<0.001; deviation ≤20PD was achieved in to be filled in 73.68 % eyes. Mean hypotropia at presentation was 13.4=/-10.3 which improved to 1.3=/-2.3 prism diopter post-operative,p<0.001. There was a significant improvement in ocular motility, p<0.001.
Conclusion- Modified silicone tube loop myopexy with or without MR recession is a safe, easy and effective procedure in the management of myopic strabismus fixus and improves alignment significantly. Efficacy is comparable with other methods of loop myopexy. No significant complications noted.
Key words- Myopic strabismus fixus, esotropia- hypotropia, silicon tube loop myopexy
INTRODUCTION
Myopic strabismus fixus, or heavy eye syndrome, is an adult onset esotropia associated with high axial myopia, typically described as progressive esotropia and hypotropia associated with restricted elevation and abduction of variable degree and severity. According to studies,1,2there is superotemporal herniation of the posterior portion of theelongated globe from the muscle cone due to increased axial length. Therefore, the lateral rectus(LR) muscle is displaced inferiorly and superior rectus (SR) muscle is displaced nasally, resulting in limitation or failure to abduct and elevate.
Loop myopexy of superior and lateral rectus has become the standard procedure of choice for myopic strabismus fixus. Various techniques of loop myopexy including sutures3 and silicon bands4,5 have been advocated in past. The disadvantage of suture myopexy includes muscle strangulation, which may affect anterior ciliary circulation and may rarely cause cheese‑wiring of the muscle.
We performed a novel modification loop myopexy using silicon tube which has been used for performing ptosis surgery. Being thinner, circular and hence absence of indentation or pressure points, need for lesser tissue handling and smaller scleral tunnel for fixation gives the primary advantage of using a silicon tube over a silicon band.
MATERIALS AND METHODS
Objective- To evaluate safety profile and surgical outcomes of a novel modification of loop myopexy with silicon tube sling (used for ptosis surgery) for patients with myopic strabismus fixus.
Materials and methods-
This is a prospective interventional case series of nineteen eyes of ten patients who had underwent silicon tube loop myopexy of superior rectus and lateral rectus for myopic strabismus fixus at a tertiary eye care centre, South India from January 2015 to June 2016. All the surgeries had been performed by the same team of surgeons. This study was approved by ethic committee and the study was carried out in accordance with the approved guidelines. Informed consent was obtained from all subjects before surgery.
In our study, all patients were diagnosed to have myopic strabismus fixus preoperatively and was confirmed by computed tomography of orbit and brain, showing superotemporal herniation of the elongated eyeball from the muscle cone, inferior displacement of the LR, and nasal displacement of the SR. Other intracranial related pathologies are excluded . Patients with less than 6 months follow-up were excluded.
The degree of esotropia and hypotropia was assessed preoperatively and postoperatively for each patient by prism bar cover test (PBCT). In the situation that PBCT could not be performed due to extreme limitation of extraocularmuscle movement, the degree of ocular deviation was estimated by the Krimsky test6,7. The degree of restriction of extraocular movement was graded into 3 grades of impairment. Grade 0 is no restriction, grade 1 is mild restriction where eyes cross midline; Grade 2 is moderate restriction in which the eye could not cross midline; Grade 3 is extreme restriction with the eye fixed in adduction with minimal movement. The degrees of restriction are reported preoperatively and postoperatively.
Individual age, sex, duration of squint, visual acuity, refractive status, axial length, any previous squint operations, and associated complications are all reported.
Surgical Techniques: All patients had surgery under peribulbar anesthesia. Forced duction tests were performed to confirm the restriction. Silicon tube loop myopexy of SR and LR was performed for all patients as described below.
A fornicealconjunctival incision is created in the superotemporal quadrant approximately 8mm posterior to the limbus. LR and SR muscles are then identified and isolated. About 14 mm from limbus scleral tunnel was made. Silicon tube was passed below LR, through the scleral tunnel and then below SR. While insertion of tube below the muscle, the needle was folded over the tube and the base of needle was passed below the muscle, taking care not toinjure muscle with needle. The tube was then passed through the sleeve and secured (Figure 1). In cases where scleral thinning prevented us from making a scleral tunnel, the tube was secured 14 mm beyond the limbus to the sclera by using 5-0 ethibond suture. All eyes underwent medial rectus recession in same sitting.
RESULTS
19 eyes of 10 patients were recruited in the study. Majority of subjects were males (73.7%) and 26.3% were females. Age ranged from 17 to 74 yearold, mean age of subjects in the study was 54.9 ± 15.8 years. All patients were followed up for a period of 1 year.
Characteristics of operated eyes- Best SnellenCorrected Visual Acuity of the operated eyes ranged from hand movement to 0.25, mean BCVA was 0.1 ± 0.1. Axial length of the operated eyes ranged from 27mm to 35.98mm, with a mean of 31.4 ± 2.7mm .The spherical equivalent of the refractive error of the operated eyes ranged from −10.00D to −24.50Dmean being 17.4 ± 3.4 dioptres.Only one patient had previous history of surgery- medial rectus recession and lateral rectus resection performed.
Loop myopexy surgery– In this series, 9 patients underwent bilateral loop myopexy whereas 1 patient underwent unilateral loop myopexy. Totally, 19 eyes underwent additional MR muscle recession. Mean pre-operative horizontal deviation at baseline was 78.7 ± 6.4 prism dioptres and at post surgery 3 months was 11.6 ± 7.1 prism dioptre. There was significant decrease in mean horizontal deviation at all the post-operative period compared to pre-operative horizontal deviation, p<0.001. A significant decrease in mean vertical deviation from 13.4 ± 10.3 prism diopter preoperative to 1.3 ± 2.3 post-operative 3 months was noted, p<0.001. From preoperative to post operative 3 months, there was a significant improvement in grade of extraocular movements compared to baseline Grade, p<0.001.
DISCUSSION
Silicon tube loop myopexy of superior rectus and lateral rectus is an effective treatment for patients with myopic strabismus fixus as it can reduce the degree of esotropia and increase in range of extraocular movement by a significant amount. As proposed by Kekunayyaet al5, the surgery helps to normalize the vectors of muscle force of the superior rectus and lateral rectus, allowing the globe to move more freely within the muscle cone by eliminating the mechanical disturbance of eye movement.
In our study we performed silicon tube loop myopexy of 19 eyes. In addition, we did do a variable amount of recession of medial rectus in all our patients as just a loop myopexy did produce residual esotropia in few of our patients. In patients with noted fibrosis of medial rectus, a hang back recession of medial rectus was performed. There was a significant decrease in horizontal and vertical deviation post operatively. The improvement in the grade of extraocular movements was also significant (Figure 2). No significant complications were noted post operatively. One patient did complain of chronic foreign body sensation, but that could be explained by anterior placement of loop. As the complaint was nonspecific, no further intervention was performed.
As compared to suture myopexy3,8, the chances of cheese wiring of muscles and anterior segment ischemia was eliminated. Moreover silicon tube loop myopexy is reversible.
Silicon tube (which is commonly used in ptosis surgery) in comparison to silicon bands which have been used previously for loop myopexy4,5, is thinner and circular (Figure 3). Hence, there is an absence of indentation or pressure points on sclera. It also warrants a need for lesser tissue handling and a smaller scleral tunnel for scleral fixation.
The major drawback of the study is smaller sample size. As myopic strabismus fixus is a rare ocular condition, the sample size is justified.
CONCLUSION
Modified silicone tube loop myopexy with or without MR recession is a safe, easy and effective procedure in the management of myopic strabismus fixus and improves alignment significantly. Efficacy is comparable with other methods of loop myopexy. No significant complications noted.
REFERENCES
-
- Yokoyama T, Tabuchi H, Ataka S, Shiraki K, Miki T, Mochizuki K. The mechanism of development in progressive esotropia with high myopia. In: de Faber JT, editor. Transactions of the 6th Meeting European Strabismological Association Barcelona, Spain, September 2000. Lisse, Netherland: Swets and Zeitlinger Publishers; 2000. p. 218‑21.
- Krzizok TH, Schroeder BU. Measurement of recti eye muscle paths by magnetic resonance imaging in highly myopic and normal subjects. Invest Ophthalmol Vis Sci 1999;40:2554‑60.
- Yamaguchi M, Yokoyama T, Shiraki K. Surgical procedure for correcting globe dislocation in highly myopic strabismus. Am J Ophthalmol 2010;149:341‑6.e2.
- Wong I, Leo SW, Khoo BK. Loop myopexy for treatment of myopic strabismus fixus. J AAPOS 2005;9:589‑91.
- Shenoy BH, Sachdeva V, Kekunnaya R. Silicone band loop myopexy in the treatment of myopic strabismus fixus: Surgical outcome of a novel modification. Br J Ophthalmol 2015;99:36‑40.
- Krimsky. The binocular examination of the young child. American Journal of Ophthalmology, vol. 26, article 624, 1943.
- Y. Choi and B. J. Kushner. The accuracy of experienced strabismologists using the Hirschberg and Krimsky tests. Ophthalmology, vol. 105, no. 7, pp. 1301–1306, 1998.
- Carol P. S. Lam, Jason C. S. Yam, Flora H. S. Lau, Dorothy S. P. Fan, C. Y. Wong, Christopher B. O. Yu,1 and WinnieW. Y. Lau. SR and LR Union Suture for the Treatment of Myopic Strabismus Fixus: Is Scleral Fixation Necessary? Hindawi Publishing Corporation BioMed Research International, vol. 2015, Article ID 470473.
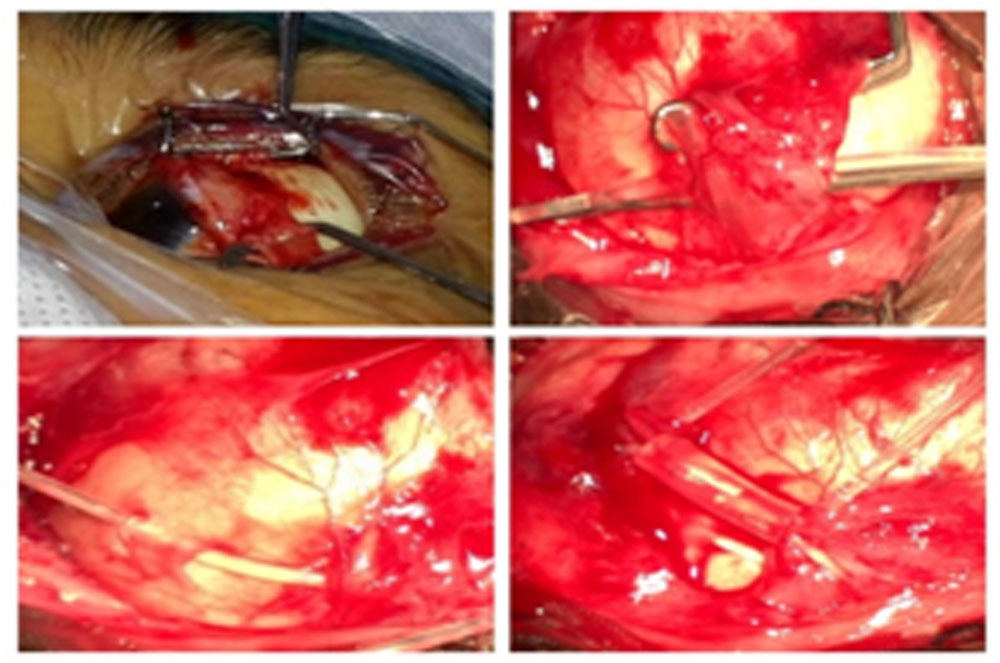
Figure 1- surgery for loop myopexy. From left to right- A- demonstration of displaced muscles. B- insertion of tube beneath muscle. C- scleral fixation of the tube. D- loopmyopexy of SR and LR with tube secured with sleeve.

Figure 2- Pre operative and post operative pictures of patient post silicon tube loop myopexy.
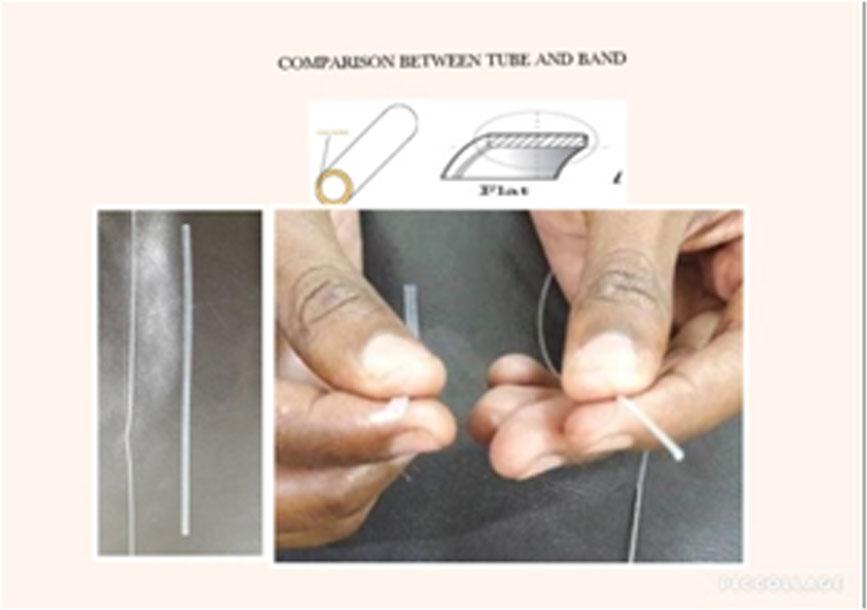
Figure 3- Comparison between silicon tube and band.
Leave a Comment