
Dr. Shiva Prasad Gantyala, G16287, Dr. Sundaramoorthy Selva Kalianna, Dr. Sushma Poojary, Dr. Ananth D.
ABSTRACT
METHOD: 30 eyes of 23 patients with progressive keratoconus were considered in our study. Inclusion and exclusion criteria, study protocol, and follow up assessments were designated. Patients were followed up for 18 months after undergoing trans-epithelial corneal collagen cross-linking (TE-CXL). Baseline visual acuity (uncorrected and best corrected), refraction (spherical, cylindrical and spherical equivalent), corneal topographic measurements (simulated maximum, minimum, average keratometry, thinnest pachymetry and posterior elevation) using Orbscan IIz (Technolas Perfect Vision), ultrasound pachymetry (Tomey SP3000) and endothelial count using specular microscopy (Topcon SP 3000P) were recorded and repeated at each postoperative follow-up visit. Intra and postoperative complications were recorded. The solution used for TE- CXL comprised riboflavin 0.1% and dextran 20.0% (NanoSigma Biotech). Ultraviolet-A treatment was performed with Iroc UV-X System at 3mW/cm2.
MAIN OUTCOME MEASURES: Patients were tested for best-corrected visual acuity (BCVA), uncorrected visual acuity (UCVA), spherical equivalent (SE), maximum keratometry reading (max-K), average of minimum and maximum keratometry readings (mean-K), central corneal thickness (CCT), and posterior elevation at the apex at baseline, at 1, 3, 6, 12 and 18months after CXL. At 1 week follow-up, only vision, refraction and slit lamp examination was done and bandage contact lens was removed.
RESULT: Mean UCVA was 0.60 ± 0.31 logarithm of the minimum angle of resolution (logMAR) at baseline and 0.54 ± 0.31 logMAR at 18 months after the procedure. For mean BCVA, these values were 0.22 ± 0.11 and 0.18 ± 0.10 logMAR, respectively (P = <0.00). The mean SE changed from -2.43 ± 2.33 diopters (D) to -1.87 ± 2.76 D, and mean refractive cylinder error changed from -2.08 ± 1.72 to -1.58 ± 1.43D (P = 0.002). Mean max-K and mean-K decreased by 0.06 ± 3.86D and 0.20 ± 2.94 D, respectively, which means there was stabilization. Mean posterior elevation changed from 80.83 ± 29.13 to 73.77 ± 27.03 μm. Two eyes from two patients showed initial stabilization till 3 months and later showed progression from the 6 month visit. These two patients were on concurrent treatment for moderate to severe vernal keratoconjunctivitis and were constant eye rubbers. They were advised to undergo repeat CXL. There was no significant change in pachymetry and endothelial count. At 1 week corneal haze was present in 12 eyes (40%) which disappeared at 18 months. There were no complications (such as infiltrates, scarring, opacities, etc.) from the procedure.
CONCLUSION: Based on our 18 month results, treatment of progressive keratoconus with CXL can stop disease progression, without raising any concern for safety. Vernal keratoconjunctivitis and eye rubbing may be an important factor for aggressive disease. CXL is effective and safe in stabilizing progressive keratoconus in pediatric age group.
Key words: Corneal collagen cross-linking, keratoconus, pediatric age group.
INTRODUCTION
Keratoconus is a progressive, frequently bilateral and asymmetric, non-inflammatory corneal thinning disorder characterized by change in structure and organization of corneal collagen lamellae. This causes conical protrusion of the cornea owing to its biomechanical instability. Keratoconic eyes appear to be more elastic and less rigid than normal eyes [1]. This leads to irregular astigmatism and subsequent poor visual acuity [2, 3]. The disease classically manifests in second decade of life and age-specific incidence rates are greatest in the younger groups.
A genetic basis for keratoconus has been suspected and several candidate genes, including those coding for different types of collagen and proteinase inhibitors as well as antioxidant genes, have been investigated. The most compelling evidence for a genetic origin in some forms of keratoconus is the degree of concordance between monozygotic twins. There are reports of at least 18 sets of monozygotic twins that identify one or both siblings in the pair with evidence of keratoconus [5]. Most families with keratoconus show autosomal dominant inheritance with variable penetration [6]. Family history is classically found in up to 6-10% of patients [4, 7-9].
The treatment algorithm has mainly consisted of visual rehabilitation with spectacles, contact lenses (soft or rigid) and keratoplasty (lamellar or penetrating) depending on the stage of the disease. When left untreated, spontaneous stabilization may occur during the third to fourth decade due to natural history of the disease, and stiffening of the corneal stroma by an increase in the number of cross-links between collagen fibrils may occur [10, 11]. Unfortunately, the progression of keratoconus for years before final stabilization may result in severe corneal scarring, and keratoplasty is the only treatment option left in up to 20% of patients [12, 13].
A new treatment modality, first introduced in the late 90s by Sporl et al [14], corneal collagen crosslinking (CXL) with irradiated riboflavin, has been utilized for over 10 years in adult population. Based on the evidence of its efficacy and safety, variations in the treatment protocol [transepithelial (TE) CXL, accelerated (ACC) CXL] [15] and its application in pediatric keratoconic patients have been under evaluation [16-18].
Keratoconus in patients less than 18 years old tends to be more aggressive and as previously outlined, rapid and severe deterioration is not exceptional. At diagnosis, 27.8% children with keratoconus were in stage 4 vs 7.8% of adults [19]. Therefore, rapid decision making is mandatory. In addition, the biomechanical rigidity of the cornea is inversely related to age and children with keratoconus are frequent eye rubbers, especially the subgroup of children with coexisting vernal keratoconjunctivitis (VKC). Therefore keratoconus progression in children may not halt on its own [20-22]. Therefore, treating patients with mild keratoconus at an earlier age could be of greater benefit than waiting until patients are older and have more advanced disease requiring corneal transplantation. As corneal transplantation in children carries a poorer prognosis than in adults [23], CXL offers immense benefits in long run.
This study aims to evaluate the efficacy of CXL in treating progressive keratoconus affecting pediatric subjects.
AIMS AND OBJECTIVES
The primary aim of this study is to evaluate the effectiveness and safety of transepithelial corneal collagen cross-linking in children with anterior keratoconus.
- To assess the progression of keratoconus after CXL.
- To analyze anterior surface keratometric changes before and after CXL.
- To assess changes in visual acuity.
- To study the effect of riboflavin on corneal endothelium.
MATERIALS AND METHODS
This study is prospective study done at Lotus Eye Care Hospital, Coimbatore, India.
STUDY DESIGN :
Prospective Non-Randomized Open Label Study
STUDY SETTING :
Patients below 18 years of age, having progressive keratoconus of mild to moderate grade attending Lotus Eye Care Hospital, Coimbatore.
STUDY PERIOD :
From July 2014 to December 2015.
SAMPLING METHOD AND SAMPLE SIZE:
Convenient sampling method was adopted for the study. Total 30 eyes of 23 patients with progressive keratoconus were included after meeting inclusion criteria.
INCLUSION CRITERIA:
- Age less than 18 years
- Slit-lamp/ clinical findings of keratoconus
- Keratoconus diagnosed on orbscan
Clinical criteria for diagnosing keratoconus:
- One or more corneal signs of keratoconus on Slit Lamp (eg, enhanced appearance of corneal nerves, Vogt striae, Fleischer ring, corneal scarring)
- Scissoring reflex on retinoscopy
- Oil droplet reflex on direct ophthalmoscopy
- Munson sign
Orbscan criteria for diagnosing keratoconus:
- Keratometry (K) value >49
- Inferior steepening
- Inferior-versus-superior corneal asymmetry; a value of 1.4 D or greater
EXCLUSION CRITERIA:
- Age more than 18 years
- Corneal thickness less than 400 um
- Presence of corneal opacity
- Concurrent corneal infection
- Herpetic clinical history
- Presence of autoimmune diseases
- Severe dry eye
- Previous ocular surgery
METHOD OF DATA COLLECTION:
After obtaining the informed consent from the patients’ parents, the data was collected using a semi structured questionnaire and both ocular and systemic examination was done as per the evaluation protocol. The patients were subjected to necessary investigations to confirm the examination findings.
Detailed history was taken to find out progression of keratoconus, wearing of contact lenses, any complications and contraindications.
PRE-OPERATIVE ASSESMENT:
- History:
Detailed history regarding onset, duration and progression of symptoms were recorded. History of use of glasses and RGP lenses were noted. Previous records of glass prescription and visual acuity were evaluated. Herpetic clinical history and autoimmune disease history was ruled out.
- Pre-operative visual acuity assessment:
- Baseline visual acuity with (BCVA) and without correction (UCVA) was recorded in all individuals with Snellen’s distance visual acuity chart. Visual acuity was converted to LogMAR equivalent for statistical analysis.
- Refraction:
Objective and subjective refraction was done. Objective refraction was done with retinoscopy or autorefractor.
- Slit lamp examination of anterior and posterior segment:
Detailed examination of anterior and posterior segment was done with Haag-Streit type slit lamp. Presence of Fleischer’s ring and Vogt’s striae was noted. Any signs of advanced keratoconus were ruled out. Any eye infection and corneal opacity was ruled out.
- Corneal topography:
Corneal topography was done using Orbscan IIz (Technolas Perfect vision). Parameters noted are-
- Sim K’s maximum (D)
- Sim K’s minimum (D)
- Sim K’s average (D)
- Corneal thickness (µm)
- Posterior elevation (µm)
- Ultrasound (USG) pachymetry:
Ultrasound pachymetry (Tomey SP 3000 pachymeter) was done to measure central corneal thickness (µm).
- Endothelial count:
Endothelial count was measured using specular microscope (Topcon SP 3000P)
CONSENT:
A written informed consent was taken from all patients’ parents before taking them up for CXL procedure.
ANAESTHESIA:
Topical anaesthesia proparacaine 0.5% [Paracain]
PAINTING AND DRAPING:
Solution of 10% povidone iodine was used to clean the skin surrounding the eye. Lid margin was cleaned with bud soaked in povidone iodine. Draping was done.
PROCEDURE:
- Patient was placed under operating microscope and eye lid speculum was inserted.
- Multiple criss-cross epithelial abrasions were made with 24 gauge needle in central 9 mm diameter area. This was done to achieve adequate penetration of riboflavin in corneal stroma.
- As a photosensitizer 0.1% riboflavin solution in 20% dextran (NanoSigma Biotech. Co., Ltd) was applied to the cornea every 2 minutes for 30 minutes to allow sufficient saturation of the stroma.
- 9 mm diameter of central cornea was irradiated with UV-A light using Iroc UV-XTM device from distance of 50 mm (5cm). Wavelength used was 365 nm and irradiance was 3mW/cm2. UV-X™ device was calibrated using the UV light meter prior to each treatment.
- During 30 minutes of irradiation, drops of riboflavin 0.1% solution were applied to cornea every 2 minutes to sustain necessary concentration of the riboflavin.
- Treated eyes were dressed with bandage contact lens (BCL) for 1 week.
POST-OPERATIVE MANAGEMENT AND EVALUATION :
Post-operative drug regimen used was –
- Antibiotics (moxifloxacin 0.5%) eye drops 4 times/day for 2 weeks
- Tear substitute (carboxymethyl cellulose sodium 0.5%) eye drops 4times/day for 4 to 8 weeks.
- Steroids (fluorometholone acetate 0.1%) eye drops 4times/day for first week and tapered over next 3 weeks.
- Post-operative visits were scheduled at day 1, 1 week, 1 month, 3 months, 6 months, 12 months and 18 months.
- Post-operative Evaluation –
- Uncorrected visual acuity (UCVA).
- Slit lamp examination of anterior segment was done to see any signs of infection, infiltrates and to confirm presence of BCL.
- Post-operative Evaluation – 1 week –
- Uncorrected visual acuity (UCVA).
- Best corrected visual acuity (BCVA).
- Refraction – both objective and subjective.
- Slit lamp examination of anterior segment – to see for epithelial healing, any signs of infection and infiltrates and corneal haze formation.
- Post-operative Evaluation – 1, 3, 6, 12 and 18 months –
- Uncorrected visual acuity (UCVA).
- Best corrected visual acuity (BCVA).
- Refraction – both objective and subjective.
- Slit lamp examination of anterior segment – to see for signs of infection, infiltrates, corneal haze formation, opacity.
- Orbscan IIz – Sim K’s maximum, Sim K’s minimum, Sim K’s average, corneal thickness, posterior elevation.
- USG pachymetry – for central corneal thickness.
- Specular microscopy – for endothelial count.
ETHICAL CONSIDERATION –
This study was approved by the Ethical Committee of the Institute.
STATISTICAL ANALYSIS
- The database was entered into a microsoft excel sheet.
- Statistical tools applied in this thesis have been evaluated using (Statistical Package for the Social Sciences) SPSS (version 17) software.
- There are two statistical measures used in this study known as Descriptive analysis and Paired t-test analysis. The descriptive analysis is a basic analysis to measure the data using percentage analysis or mean and standard deviation.
- The paired t-test analysis is used to compare two populations, in which one population contains preoperative data and another population contains postoperative data. The effectiveness of paired t-test is observed using the p-value.
- A Pearson’s co-efficient “p” value of 0.05% or less was considered statistically significant.
RESULTS AND OBSERVATION
Total 30 eyes of 23 patients were included in this study.
Table 3: Age distribution of the study sample.
| Age | Patients (eyes) | Percent |
| <10 | 2 (3) | 10.00 |
| 10-15 | 11 (14) | 46.67 |
| >15 | 10 (13) | 43.33 |
| Total | 23 (30) | 100.00 |
Chart 1: Age distribution of the study sample.
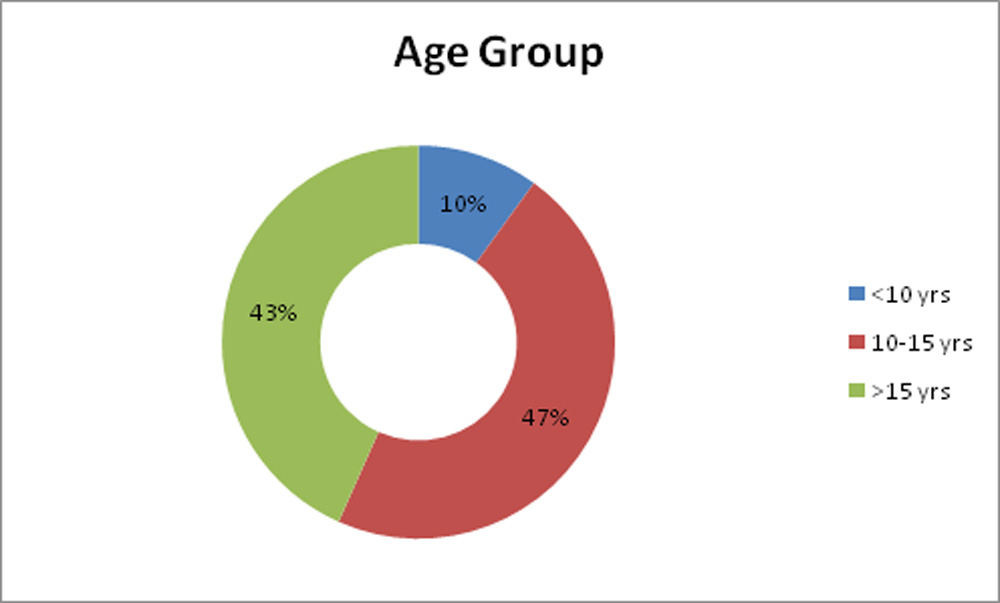
Study population had a mean age of 14.13 + 2.83years. Age of patients was ranging from 8 to 17 years. 2 patients (3 eyes; 10%) were aged 10 years or less. 11 patients (14 eyes; 47.67%) were between 10-15 years and 10 patients (13eyes; 43.33%) were above 15 years.
Out of a total of 23 patients, 10 patients had bilateral disease.
Table 4: Laterality of eye involvement of the study sample.
| Laterality | No. of Patients | Percent |
| Bilateral | 10 | 43.5% |
| Unilateral | 13 | 56.5% |
| Total | 23 | 100.0% |
Chart 2: Laterality of eye involvement of the study sample.
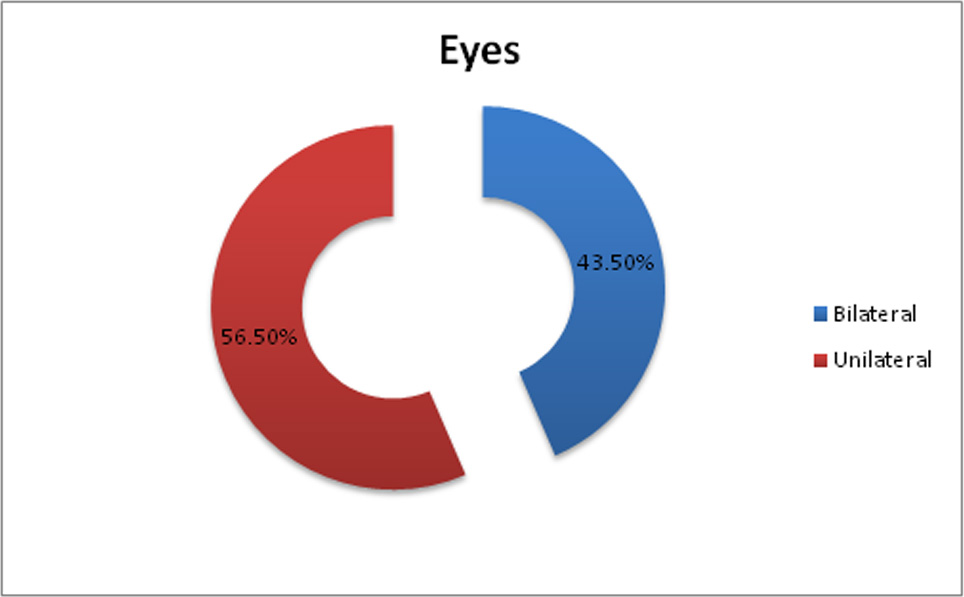
BILATERAL:
Both eyes of 7 patients (14 eyes) were included in this study. Only one eye of remaining 3 bilateral cases (3 eyes) was included in this study. Other eye of these patients was not included in the study as thinnest pachymetry was less than 400µm.
UNILATERAL:
These 3 eyes were treated with CXL using hypotonic riboflavin solution. 13 patients (13 eyes) had unilateral disease.
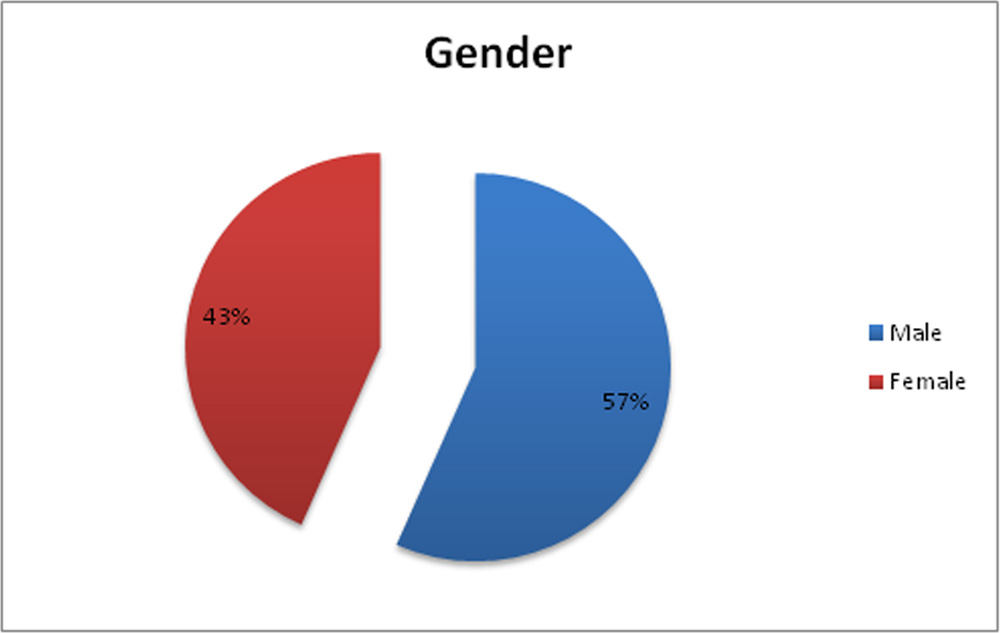
Study included 17 male (56.67%) and 13 (43.33%) female eyes.
Table 5: Sex distribution of the study sample.
| Gender | No. of eyes | Percent |
| Male | 17 | 56.67 |
| Female | 13 | 43.33 |
| Total | 30 | 100.00 |
Chart 3: Sex distribution of the study sample.
VISUAL ACUITY –
Table 6: Mean UCVA of the study sample.
| UCVA | Mean | SD | P-value |
| Pre-OP | 0.60 | 0.31 | 0.057 |
| 1wk | 0.60 | 0.30 | |
| Pre-OP | 0.60 | 0.31 | 0.020 |
| 1mth | 0.57 | 0.32 | |
| Pre-OP | 0.60 | 0.31 | 0.014 |
| 3mths | 0.55 | 0.32 | |
| Pre-OP | 0.60 | 0.31 | 0.001 |
| 6mths | 0.55 | 0.31 | |
| Pre-OP | 0.60 | 0.31 | 0.000 |
| 12mths | 0.55 | 0.31 | |
| Pre-OP | 0.60 | 0.31 | 0.001 |
| 18mths | 0.54 | 0.31 |
Chart 4: Changes in mean UCVA of the study sample
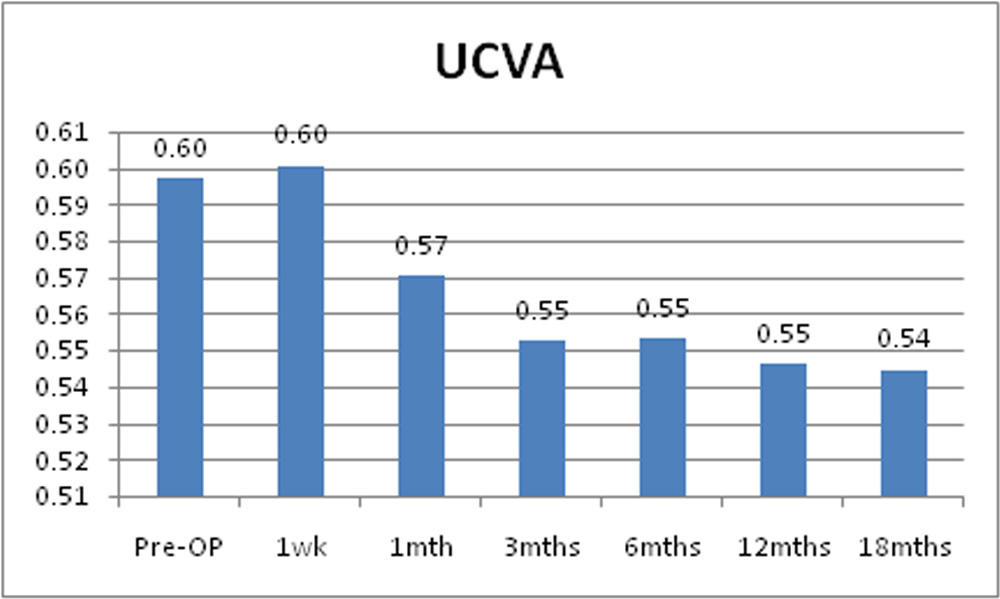
Mean pre-operative LogMAR UCVA was 0.60 + 0.31. Post operatively it was 0.60 + 0.30 at 1 week, 0.57 + 0.32 at 1 month, 0.55 + 0.32 at 3 months, 0.55 + 0.31 at 6 months, 0.55 + 0.31 at 12 months and 0.54 + 0.31 at 18 months. Difference between mean LogMAR UCVA pre and post operatively was significant from 1 month up to 18 months.
Table 7:Mean BCVA of the study sample.
| BVCA | Mean | SD | P-value |
| Pre-OP | 0.22 | 0.11 | 0.001 |
| 1wk | 0.23 | 0.11 | |
| Pre-OP | 0.22 | 0.11 | 0.017 |
| 1mth | 0.21 | 0.11 | |
| Pre-OP | 0.22 | 0.11 | 0.002 |
| 3mths | 0.21 | 0.11 | |
| Pre-OP | 0.22 | 0.11 | 0.000 |
| 6mths | 0.19 | 0.11 | |
| Pre-OP | 0.22 | 0.11 | 0.000 |
| 12mths | 0.18 | 0.10 | |
| Pre-OP | 0.22 | 0.11 | 0.000 |
| 18mths | 0.18 | 0.10 |
Chart 5: Changes in mean BCVA of the study sample.
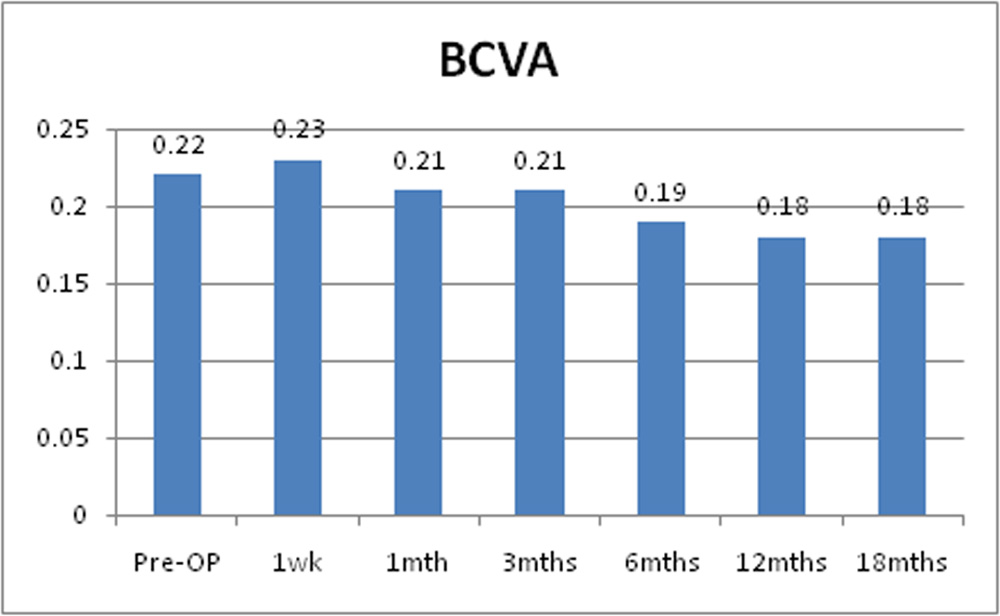
Mean pre-operative LogMAR BCVA was 0.22 + 0.11. Post operatively it was 0.23 + 0.11 at 1 week, 0.21+ 0.11 at 1 month, 0.21 + 0.11 at 3 months, 0.19 + 0.11 at 6 months, 0.18 + 0.10 at 12 months and 0.18 + 0.10 at 18 months. Mean LogMAR BCVA decreased significantly post operatively at 1 month and was sustained through 3, 6, 12 and 18 months post operatively and it was statistically significant.
REFRACTION–
Table 8: Mean sphere of the study sample
| Sphere | Mean | SD | p-value |
| Pre-OP | -1.39 | 2.15 | 0.326 |
| 1wk | -1.38 | 2.15 | |
| Pre-OP | -1.39 | 2.15 | 0.026 |
| 1mth | -1.27 | 2.17 | |
| Pre-OP | -1.39 | 2.15 | 0.018 |
| 3mths | -1.20 | 2.15 | |
| Pre-OP | -1.39 | 2.15 | 0.007 |
| 6mths | -1.13 | 2.13 | |
| Pre-OP | -1.39 | 2.15 | 0.065 |
| 12mths | -1.10 | 2.46 | |
| Pre-OP | -1.39 | 2.15 | 0.049 |
| 18mths | -1.08 | 2.46 |
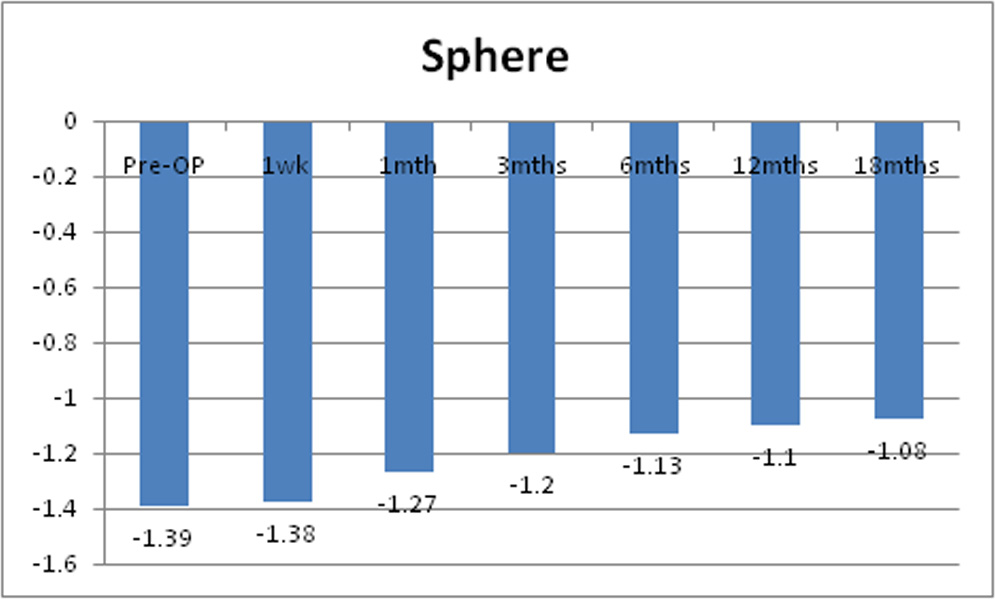 Chart 6: Changes in mean sphere of the study sample
Chart 6: Changes in mean sphere of the study sample
Mean pre-operative sphere was -1.39D + 2.15D. Post operatively it decreased to -1.38 + 2.15D at 1 week, -1.27D + 2.17D at 1 month, -1.20D + 2.15D at 3 months, -1.13D + 2.13D at 6 months, -1.10D + 2.46D at 12 months and -1.08D + 2.46D at 18 months. The decrease was statistically significant from 1 month but decreased significance by 18 months.
Table 9: Mean cylinder of the study sample.
| Cylinder | Mean | SD | p-value |
| Pre-OP | -2.08 | 1.72 | — |
| 1wk | -2.08 | 1.72 | |
| Pre-OP | -2.08 | 1.72 | 0.062 |
| 1mth | -1.95 | 1.76 | |
| Pre-OP | -2.08 | 1.72 | 0.003 |
| 3mths | -1.81 | 1.70 | |
| Pre-OP | -2.08 | 1.72 | 0.000 |
| 6mths | -1.74 | 1.48 | |
| Pre-OP | -2.08 | 1.72 | 0.005 |
| 12mths | -1.67 | 1.45 | |
| Pre-OP | -2.08 | 1.72 | 0.002 |
| 18mths | -1.58 | 1.43 |
Chart 7: Changes in mean cylinder of the study sample
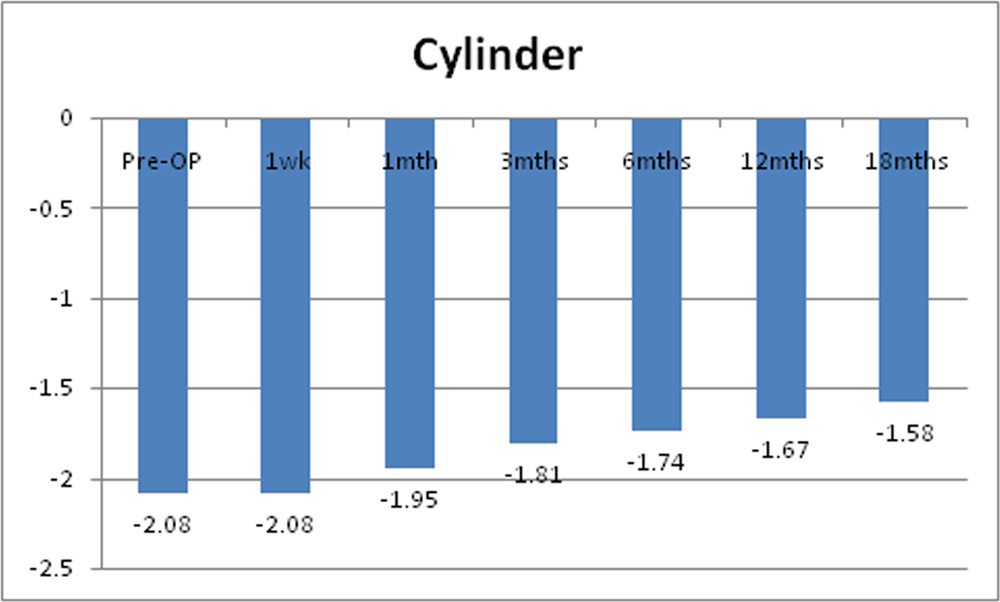
Mean pre-operative cylinder was -2.08D + 1.72D. Post operatively there was no change at 1 week. It reduced to -1.95D + 1.76D at 1 month, -1.81D + 1.70D at 3 months, -1.74D + 1.48D at 6 months, -1.67D + 1.45D at 12 months and -1.58D + 1.43D at 18 months. Statistically significant decrease in mean cylinder was noted at 3, 6, 12 and 18 month.
Table 10: Mean of spherical equivalent in study sample.
| Spherical equivalent | Mean | SD | p-value |
| Pre-OP | -2.43 | 2.33 | 0.231 |
| 1wk | -2.39 | 2.31 | |
| Pre-OP | -2.43 | 2.33 | 0.012 |
| 1mth | -2.26 | 2.41 | |
| Pre-OP | -2.43 | 2.33 | 0.001 |
| 3mths | -2.10 | 2.44 | |
| Pre-OP | -2.43 | 2.33 | 0.000 |
| 6mths | -2.00 | 2.38 | |
| Pre-OP | -2.43 | 2.33 | 0.023 |
| 12mths | -1.93 | 2.75 | |
| Pre-OP | -2.43 | 2.33 | 0.012 |
| 18mths | -1.87 | 2.76 |
Chart 8: Changes in mean of spherical equivalent of the study sample
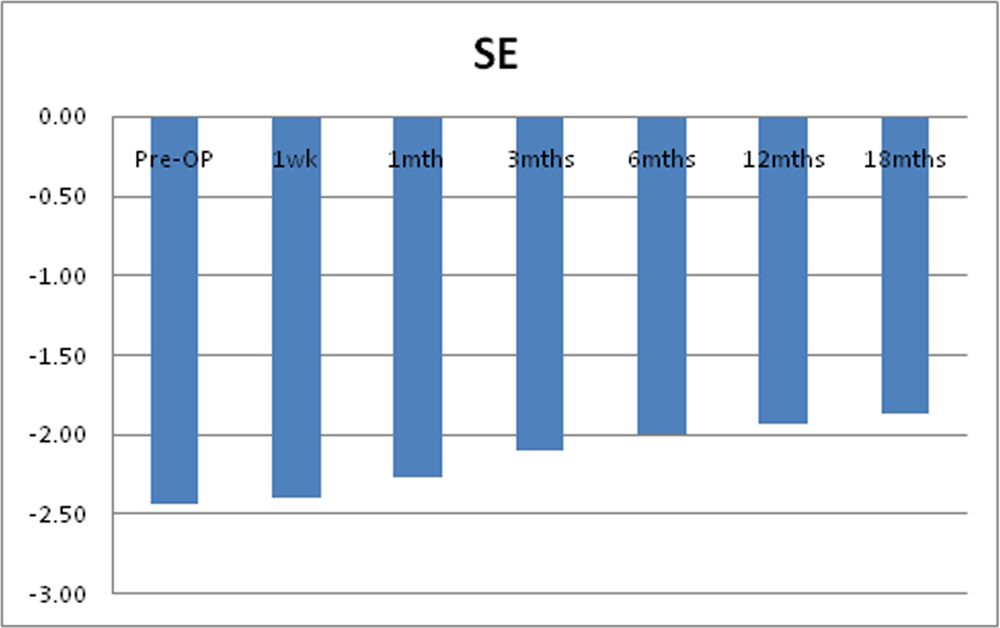
Mean pre-operative spherical equivalent (SE) was -2.43D + 2.33D. Post operatively it decreased to -2.39 + 2.31 t 1 week, -2.26D + 2.41D at 1 month, -2.10D + 2.44D at 3 months, – 2.00D + 2.38D at 6 months, -1.93D + 2.75 at 12 months and -1.87D + 2.76D at 18 months. Post operative decrease in mean spherical equivalent was statistically significant from 1 month through 18 months.
CORNEAL TOPOGRAPHY–
Table 11: Mean of maximum K Value of the study sample.
| Max-K | Mean | SD | p-value |
| Pre-OP | 50.33 | 3.53 | 0.501 |
| 1mth | 50.45 | 3.40 | |
| Pre-OP | 50.33 | 3.53 | 0.263 |
| 3mths | 50.70 | 3.85 | |
| Pre-OP | 50.33 | 3.53 | 0.370 |
| 6mths | 50.54 | 3.82 | |
| Pre-OP | 50.33 | 3.53 | 0.650 |
| 12mths | 50.38 | 3.85 | |
| Pre-OP | 50.33 | 3.53 | 0.893 |
| 18mths | 50.27 | 3.86 |
Chart 9: Changes in mean of maximum K value of the study sample
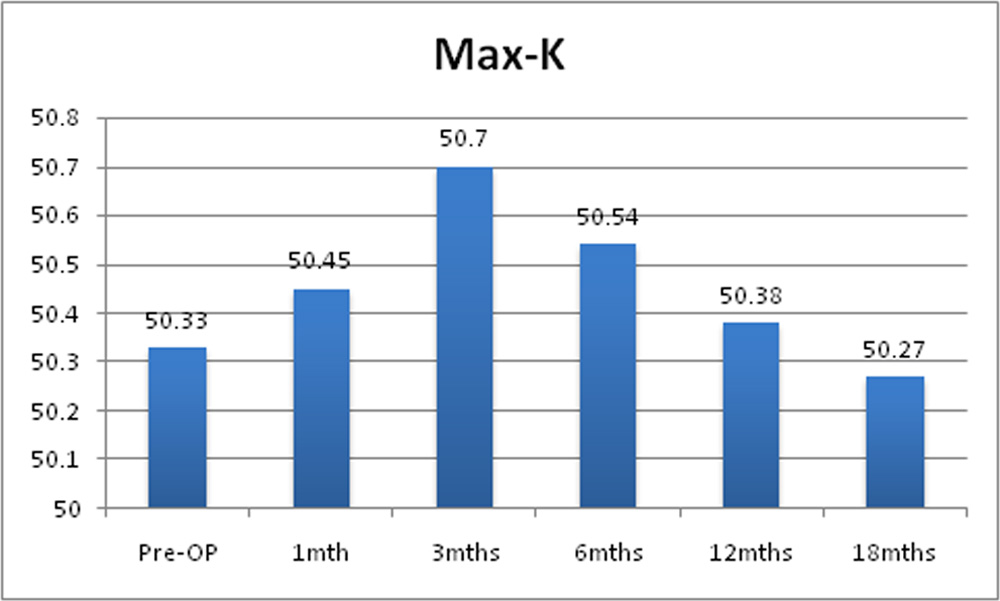
Mean pre-operative minimum K value was 45.92D + 2.59D. Post operatively it was 45.94D + 2.50D at 1 month, 46.92D + 2.42D at 3 months, 45.86D + 2.51D at 6 months, 45.71D + 2.53D at 12 months and 45.67 + 2.67 at 18 months. Post operative decrease in mean of minimum K value was not statistically significant.
Table 13: Mean of mean K Value of the study sample.
| Mean-K | Mean | SD | p-value |
| Pre-OP | 48.12 | 2.82 | 0.587 |
| 1mth | 48.19 | 2.69 | |
| Pre-OP | 48.12 | 2.82 | 0.464 |
| 3mths | 48.32 | 2.85 | |
| Pre-OP | 48.12 | 2.82 | 0.623 |
| 6mths | 48.17 | 2.88 | |
| Pre-OP | 48.12 | 2.82 | 0.951 |
| 12mths | 48.06 | 2.94 | |
| Pre-OP | 48.12 | 2.82 | 0.575 |
| 18mths | 47.92 | 2.94 |
Chart 11: Changes in mean of mean of K of the study sample.
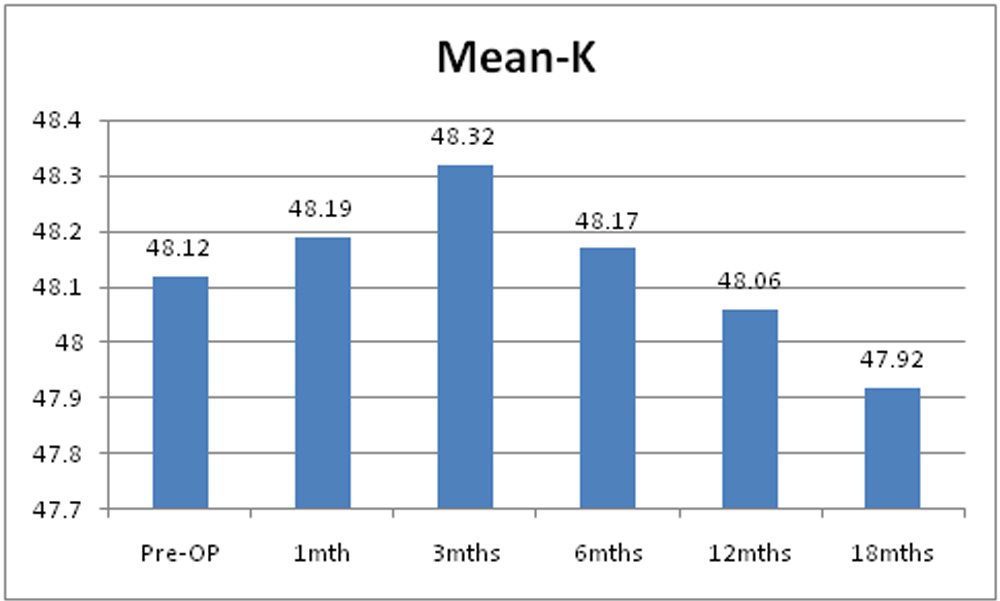
Pre operatively mean of mean K value was 48.12D + 2.78D. Post operatively it was 48.19D + 2.69D at 1 month, 48.32D + 2.85D at 3 months, 48.17D + 2.88D at 6 months, 48.06 + 2.94 at 12 months and 47.92D + 2.94D at 18 months. Post operative decrease in mean of mean K value was not statistically significant.
Table 14: Mean of posterior elevation of the study sample.
| Posterior elevation | Mean | SD | p-value |
| Pre-OP | 80.83 | 29.13 | 0.000 |
| 1mth | 79.38 | 28.92 | |
| Pre-OP | 80.83 | 29.13 | 0.004 |
| 3mths | 77.14 | 27.33 | |
| Pre-OP | 80.83 | 29.13 | 0.000 |
| 6mths | 76.53 | 26.33 | |
| Pre-OP | 80.83 | 29.13 | 0.003 |
| 12mths | 75.07 | 26.49 | |
| Pre-OP | 80.83 | 29.13 | 0.000 |
| 18mths | 73.77 | 27.03 |
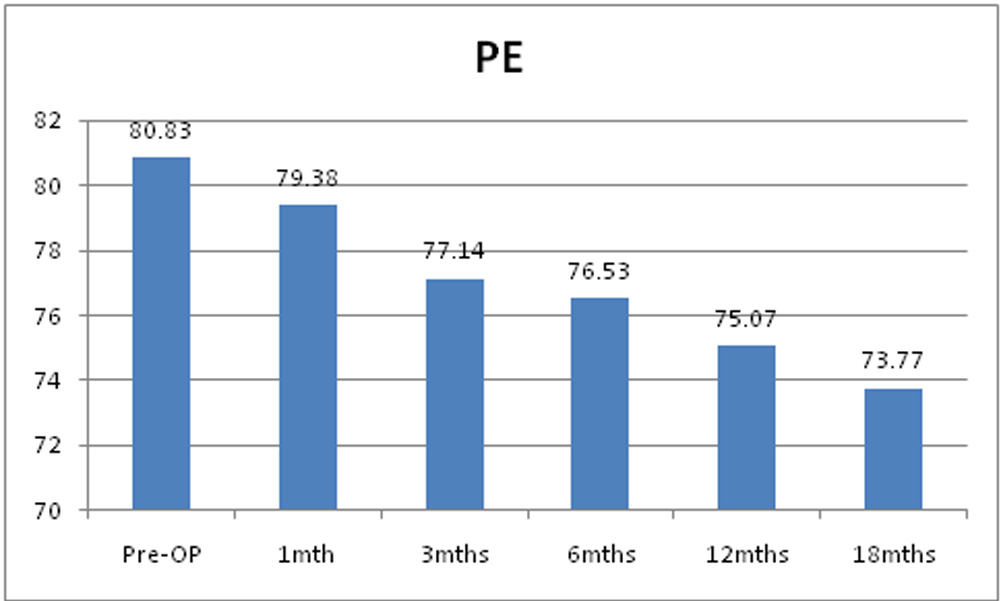
Mean of pre operative posterior elevation was 80.83µm + 29.13µm. Post operatively it decreased to79.38µm + 28.92µm at 1 month, 77.14µm + 27.33µm at 3 month, 76.53µm + 26.33µm at 6 months, 75.05µm + 26.49µm at 6 months and 73.77µm + 27.03µm at 12 months. Post operative decrease in mean of posterior elevation was statistically significant through 18 months.
Table 15: Mean of optical pachymetry value of the study sample.
| Optical pachymetry | Mean | SD | p-value |
| Pre-OP | 455.07 | 37.48 | 0.000 |
| 1mth | 379.17 | 41.82 | |
| Pre-OP | 455.07 | 37.48 | 0.000 |
| 3mths | 405.97 | 45.41 | |
| Pre-OP | 455.07 | 37.48 | 0.000 |
| 6mths | 425.77 | 40.35 | |
| Pre-OP | 455.07 | 37.48 | 0.001 |
| 12mths | 447.10 | 35.86 | |
| Pre-OP | 455.07 | 37.48 | 0.120 |
| 18mths | 452.47 | 36.40 |
Chart 13: Changes in mean of optical pachymetry of the study sample.
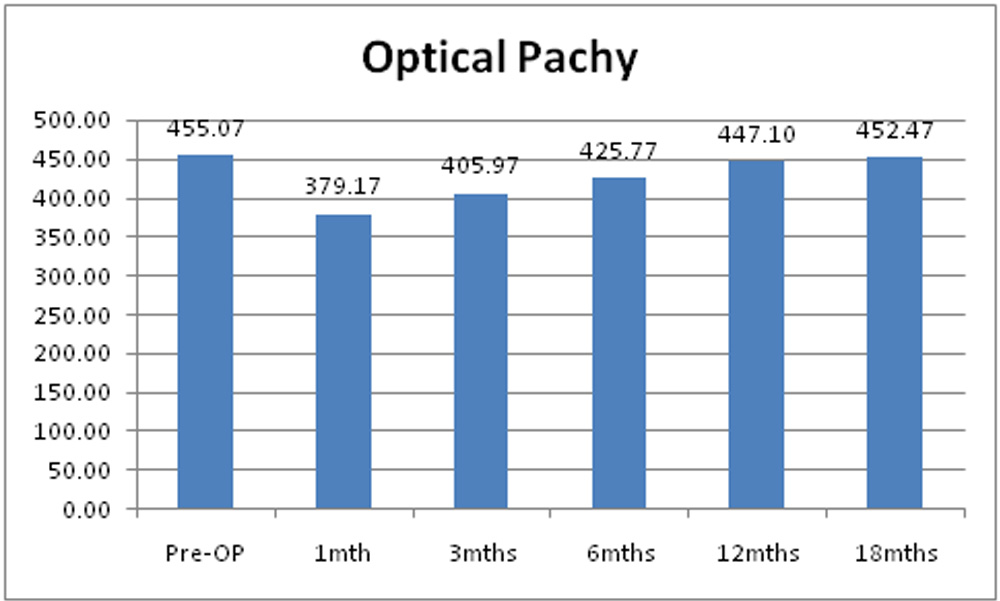
Mean of optical pachymetry value was 455.07µm + 37.48m. Post operatively it decreased to 379.17µm + 41.82µm at 1 month, 405µm + 45.41m at 3 months, 425.07µm + 40.35µm at 6 months, 447.10µm + 35.86µm at 12 months and 452.47 + 36.40. Mean optical pachymetry value decreased significantly at 1, 3, 6 and 12 months. But decrease in optical pachymetry value was not statistically significant at 18 months.
ULTRASOUND PACHYMETRY –
Table 16: Mean of USG pachymetry value of the study sample.
| USG pachymetry | Mean | SD | p-value |
| Pre-OP | 465.83 | 37.35 | 0.000 |
| 1mth | 464.00 | 36.50 | |
| Pre-OP | 465.83 | 37.35 | 0.090 |
| 3mths | 465.21 | 36.53 | |
| Pre-OP | 465.83 | 37.35 | 0.062 |
| 6mths | 463.60 | 36.49 | |
| Pre-OP | 465.83 | 37.35 | 0.171 |
| 12mths | 463.37 | 36.10 | |
| Pre-OP | 465.83 | 37.35 | 0.030 |
| 18mths | 463.17 | 37.99 |
Chart 14: Changes in mean of USG pachymetry of the study sample.
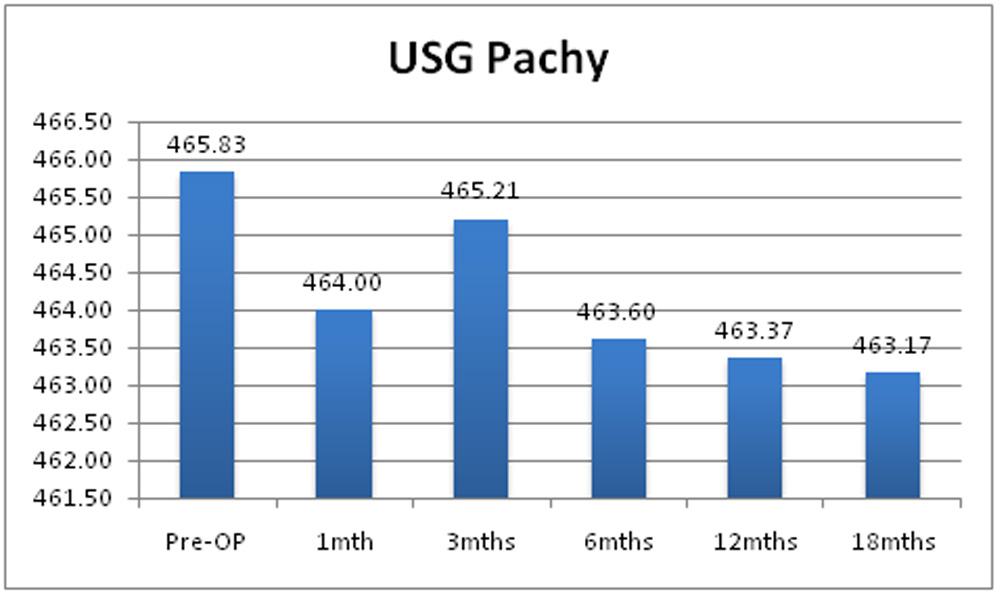
Mean of pre operative USG pachymetry value was 453.83um + 28.46um. Post operatively it was 453.43um + 28.40um at 1 month, 454.94um+ 26.49um at 3 months, 453.35um + 27.38um at 6 months and 453.94um + 28.59um at 12 months. Change in mean USG pachymetry value was not statistically significant at 1, 3, 6 and 12 months.
SLIT LAMP EXAMINATION–
Table 17: Post-operative corneal haze formation in the study sample.
| Haze Formation | Present | Absent | Total |
| 1 week | 12 | 18 | 30 |
| 40.00% | 60.00% | 100.00% | |
| 1 Month | 8 | 22 | 30 |
| 26.67% | 73.33% | 100.00% | |
| 3 Months | 7 | 23 | 30 |
| 23.33% | 76.67% | 100.00% | |
| 6 Months | 3 | 27 | 30 |
| 10.00% | 90.00% | 100.00% | |
| 12 Months | 0 | 30 | 30 |
| 0.00% | 100.00% | 100.00% | |
| 18 Months | 0 | 30 | 30 |
| 0.00% | 100.00% | 100.00% |
Chart 15: Presence of corneal haze formation in the study sample.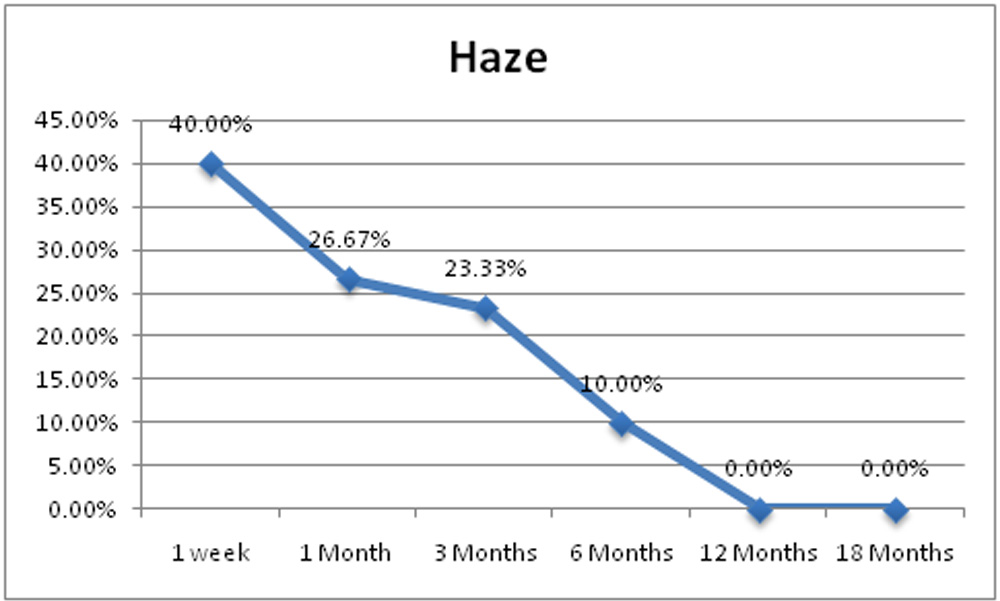
Corneal haze clinically detectable by slit lamp examination was present in 40% eyes (12eyes) at 1 week, 26.67% eyes (8 eyes) at 1 month, 23.33% eyes (7 eyes) at 3 month and 10% eyes (3 eyes) at 6 month. No patient had clinically detectable haze at 12 months and 18 months post operatively.
ENDOTHELIAL COUNT-
Table 18: Mean endothelial count of study sample.
| Endothelial count | Mean | SD | p-value |
| Pre-OP | 3252.97 | 211.61 | 0.732 |
| 1mth | 3259.27 | 177.97 | |
| Pre-OP | 3252.97 | 211.61 | 0.136 |
| 3mths | 3226.00 | 158.64 | |
| Pre-OP | 3252.97 | 211.61 | 0.810 |
| 6mths | 3248.97 | 187.01 | |
| Pre-OP | 3252.97 | 211.61 | 0.163 |
| 12mths | 3226.33 | 191.25 | |
| Pre-OP | 3252.97 | 211.61 | 0.823 |
| 18mths | 3249.43 | 197.04 |
Chart 16: Changes in mean endothelial count of the study sample.
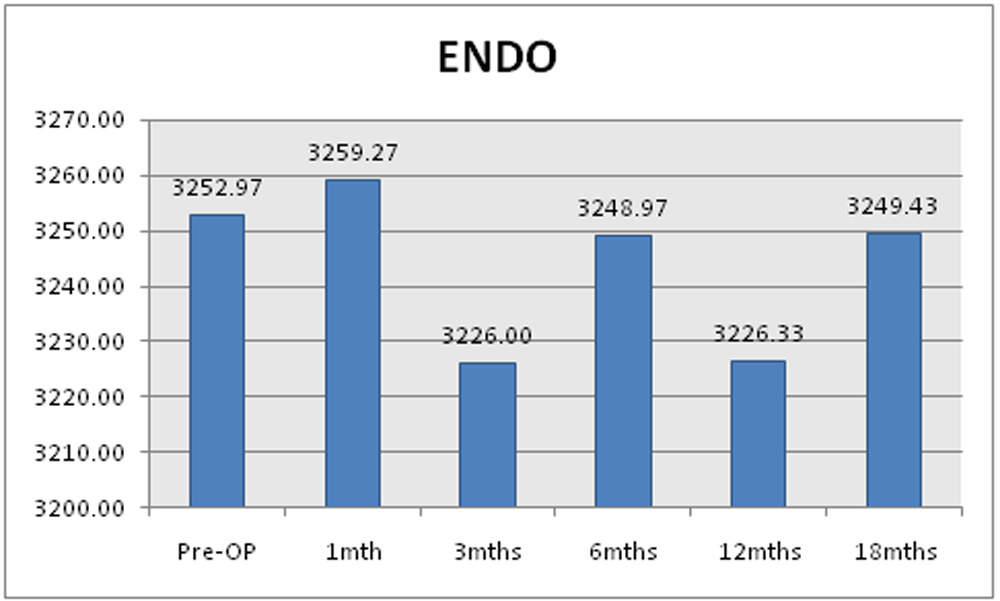
Mean of preoperative endothelial count was 3252.97 + 211.61. Postoperatively it was 3259 + 177.97 at 1 month, 3226.00 + 158.64 at 3 months, 3248 + 187.01 at 6 months, 3226.33 + 191.25 at 12 months and 3249.43 + 197.04 at 18 months. These changes are not statistically significant.
DISCUSSION
Keratoconus is common condition with incidence of 1per 2000 general population [2, 3]. The onset of disease occurs in puberty [7]. Because of young age of patients, keratoconus has significant negative effect on quality of life [24]. Additionally, the disease tends to be more aggressive and difficult to treat in younger individuals. There was no treatment to stop the progression of disease before the advent of CXL. Thus, because of its progressive nature, keratoconus was the most frequent reason for keratoplasty in past 3 decades [25].
The specific cause of keratoconus is not known. Keratoconus changes are associated with increased degradative enzyme levels and increased free radicals, causing oxidative stress and damage. It is also associated with increased apoptosis of stromal keratocytes. All these changes lead to alterations in collagen compound and their bondings causing stromal lamellar slippage and altered collagen scaffold [26].
Corneal collagen cross linking technique was developed to counteract the progressive corneal thinning and progression of keratoconus, thus maintaining the visual status and preventing its further deterioration [27]. With CXL additional covalent bonding between collagen molecules can be achieved, which restores the strength of the cornea.
Studies in adult populations of more than a decade have shown the efficacy as well as the safety of CXL. Thus it can and must be used to treat even the younger individuals.
Our study included 30 eyes of 23 individuals aged less than 17 years.
The present study demonstrates improvement in UCVA and BCVA which was statistically significant at 3 months and improvement remained significant at 6, 12 and 18 months. Caporossi et al have shown similar improvement in UCVA and BCVA [28].
In current study, decrease in sphere, cylinder and spherical equivalent started at 1 month, became statistically significant at 3 months and remained significant thereafter till 18 months of follow up. Vinciguerra et al., have demonstrated similar decrease in sphere, cylinder and spherical equivalent in their study [29].
Mean, maximum and minimum keratometry readings decreased, but did not reach statistical significance similar to the study by Bakshi et al [30].
Posterior elevation in our study, decreased significantly at 1 months and reduction remained significant at 3, 6, 12 and 18 months. Significant PE changes have been well documented in adult studies.
Optical pachymetry value reduced significantly at 1, 3, 6 and 12 months. At 18 months follow up reduction was not significant. Optical pachymetry data recorded by Orbscan analysis in first 6 – 12 post operative months was affected negatively by changes in stromal reflectivity [31, 32]. Stromal reflectivity changes are documented after CXL procedure, by in vivo confocal analysis. Over months, stromal reflectivity becomes more homogenous reducing visibility of demarcation line [16]. This leads to increase in pachymetry value on Orbscan after 12 months.
Ultrasound pachymetry is less influenced by CXL induced stromal microstructural changes, providing more reliable post operative pachymetry measurements [16]. In our study there was no statistically significant difference between mean pre and post operative pachymetry value at any visit.
Corneal haze was present in 40% eyes (12eyes) at 1 week, 26.7% eyes (8 eyes) at 1 month, 23.3% eyes (7eyes) at 3 month and 10% eyes (3 eyes) at 6 month. No patient had clinically detectable haze at 12 months post operatively.
Two eyes of two patients showed initial stabilization till 6month follow-up visit. They showed worsening from 12 month visit. These two patients were habitual eyes rubbers. They were adviced re-treatment, results of which are still awaited.
No infections, infiltrates or corneal opacities were noted in post operative period.
CONCLUSION
In conclusion CXL is safe, effective and minimally invasive procedure to stop progression of mild to moderate grade keratoconus. However, further follow-up and additional patients must be reviewed to draw final conclusions about the efficacy and safety.
LIMITATIONS OF THE STUDY
- Small sample size.
- Duration of follow – up was 18 months. Long term follow up required for assessing the duration of efficacy of procedure.
- Anterior segment OCT and confocal microscopy would have been useful to assess depth of treated cornea and to demonstrate stromal changes after CXL procedure.
- Only transepithelial CXL was done. It should have been compared with epithelium off standard procedure to compare the efficacy.
REFERENCES
- 1.Edmund, “Assessment of an elastic model in the pathogenesis of keratoconus,” Acta Ophthalmologica, vol. 65, no. 5, pp. 545– 550, 1987.
- S. Rabinowitz, “Keratoconus,” Survey of Ophthalmology, vol. 42, no. 4, pp. 297–319, 1998.
- E. Davidson, S. Hayes, A. J. Hardcastle, and S. J. Tuft, “The pathogenesis of keratoconus,” Eye, vol. 28, no. 2, pp. 189–195, 2014.
- Gordon-Shaag, M. Millodot, E. Shneor, and Y. Liu, “The genetic and environmental factors for keratoconus,” BioMed Research International, vol. 2015, Article ID 795738, 19 pages, 2015.
- Pflugfelder SC, Liu Z, Monroy D, et al: Detection of sialomucin complex (MUC4) in human ocular surface epithelium and tear fluid. Invest Ophthalmol Vis Sci2000; 41:1316-1326.
- Rabinowitz YS, Maumenee IH, Lundergan MK: Molecular genetic analysis in autosomal dominant keratoconus. Cornea. 1992; 11(4):302-8
- Kennedy RH, Bourne WM, Dyer JA: A 48 year clinical and epidemiological study of keratoconus. Am J Ophthamol. 1986; 101:267-273
- Gonzalez and P. J. McDonnell, “Computer-assisted corneal topography in parents of patients with keratoconus,” Archives of Ophthalmology, vol. 110, no. 10, pp. 1412–1414, 1992.
- S. Rabinowitz, J. Garbus, and P. J. McDonnell, “Computer assisted corneal topography in family members of patients with keratoconus,” Archives of Ophthalmology, vol. 108, no. 3, pp. 365–371, 1990.
- S. Malik, S. J. Moss,N.Ahmed,A. J. Furth,R. S.Wall, and K. M. Meek, “Ageing of the human corneal stroma: structural and biochemical changes,” Biochimica et Biophysica Acta, vol. 1138, no. 3, pp. 222–228, 1992.
- Daxer, K. Misof, B. Grabner, A. Ettl, and P. Fratzl, “Collagen fibrils in the human corneal stroma: structure and aging,” Investigative Ophthalmology and Visual Science, vol. 39, no. 3, pp. 644–648, 1998.
- E. Smiddy, T. R. Hamburg, G. P. Kracher, and W. J. Stark, “Keratoconus. Contact lens or keratoplasty?” Ophthalmology, vol. 95, no. 4, pp. 487–492, 1988.
- J. Tuft, L. C. Moodaley, W. M. Gregory, C. R. Davison, and R. J. Buckley, “Prognostic factors for the progression of keratoconus,” Ophthalmology, vol. 101, no. 3, pp. 439–447, 1994.
- Sp¨orl, M. Huhle, M. Kasper, and T. Seiler, “Increased rigidity of the cornea caused by intrastromal cross-linking,” Der Ophthalmologe: Zeitschrift der Deutschen Ophthalmologischen Gesellschaft, vol. 94, no. 12, pp. 902–906, 1997.
- Touboul D, Efron N, Smadja D, Praud D, Malet F, Colin J. Corneal confocal microscopy following conventional, transepithelial, and accelerated corneal collagen cross‑linking procedures for keratoconus. J Refract Surg 2012;28:769‑
- Caporossi,C.Mazzotta, S. Baiocchi, and T.Caporossi, “Longterm results of riboflavin ultraviolet a corneal collagen crosslinking for keratoconus in Italy: the Siena eye cross study,” American Journal of Ophthalmology, vol. 149, no. 4, pp. 585–593, 2010.
- D. Kymionis, M. A. Grentzelos, D. A. Liakopoulos et al., “Long-term follow-up of corneal collagen cross-linking for keratoconus—the cretan study,” Cornea, vol. 33,no. 10,pp. 1071– 1079, 2014.
- Theuring, E. Spoerl, L. E. Pillunat, and F. Raiskup, “Corneal collagen cross-linking with riboflavin and ultraviolet-a light in progressive keratoconus,” Der Ophthalmologe, vol. 112, no. 2, pp. 140–147, 2015.
- Léoni‑Mesplié S, Mortemousque B, Touboul D, Malet F, Praud D, Mesplié N, et al. Scalability and severity of keratoconus in children. Am J Ophthalmol 2012;154:56‑
- Ertan A, Muftuoglu O. Keratoconus clinical findings according to different age and gender groups. Cornea 2008;27:1109‑
- Reeves SW, Stinnett S, Adelman RA, Afshari NA. Risk factors for progression to penetrating keratoplasty in patients with keratoconus. Am J Ophthalmol 2005;140:607–11.
- Kamiya K, Shimizu K, Ohmoto F. Effect of aging on corneal biomechanical parameters using the ocular response analyzer. J Refract Surg 2009;25:888‑
- Vanathi M, Panda A, Vengayil S, Chaudhuri Z, Dada T. Pediatric keratoplasty. Surv Ophthalmol 2009;54:245‑71
- Nottingham J. Practical observations on conical cornea: and on the short sight, and other defects of vision connected with it. 1854; London, John Churchill.
- Maeno A, Naor J, Lee HM: Three decades of corneal transplantation: indications and patient characteristics. Cornea. 2000;19:7-11.
- Polack F: Contribution of electron microscopy to the study of corneal pathology. Surv Ophthalmol.1976; 20:375-414.
- Vinciguerra, E. Alb`e, S. Trazza, T. Seiler, and D. Epstein, “Intraoperative and postoperative effects of corneal collagen cross-linking on progressive keratoconus,” Archives of Ophthalmology, vol. 127, no. 10, pp. 1258–1265, 2009.
- Caporossi A, Mazzotta C, Baiocchi S, Caporossi T, Denaro R, Balestrazzi A. Riboflavin‑UVA‑induced corneal collagen cross‑linking in pediatric patients. Cornea 2012;31:227‑
- Vinciguerra P, Albé E, Frueh BE, Trazza S, Epstein D. Two‑year corneal cross‑linking results in patients younger than 18 years with documented progressive keratoconus. Am J Ophthalmol 2012;154:520‑
- Bakshi E, Barkana Y, Goldich Y, Avni I, Zadok D. Corneal Cross‑Linking for Progressive Keratoconus in Children: Our Experience. Int J Keratoco Ectatic Corneal Dis 2012;1:53‑
- Mazzotta C, Traversi C, Baiocchi S. Corneal healing after riboflavin ultraviolet A collagen cross-linking determined by confocal laser scanning microscopy in vivo: early and late modifications. Am J Ophthalmol. 2008; 146:527-533.
- Mazzotta C, Balestrazzi A, Traversi C, Baiocchi S. Treatment of progressive keratoconus by riboflavin UV-A induced cross-linking of corneal collagen: ultrastructural analysis by Heidelberg Retinal Tomograph II in vivo conofocal microscopy in humans. Cornea. 2007; 26:390-397.
COLOUR PHOTOGRAPHS

Fig. 17: Iroc UV-X system.

Fig. 18: Operation theatre assembly for performing CXL.

Fig. 19: UV meter.

Fig.20: Iroc UV-X machine.
Fig. 21: Isotonic Riboflavin solution.
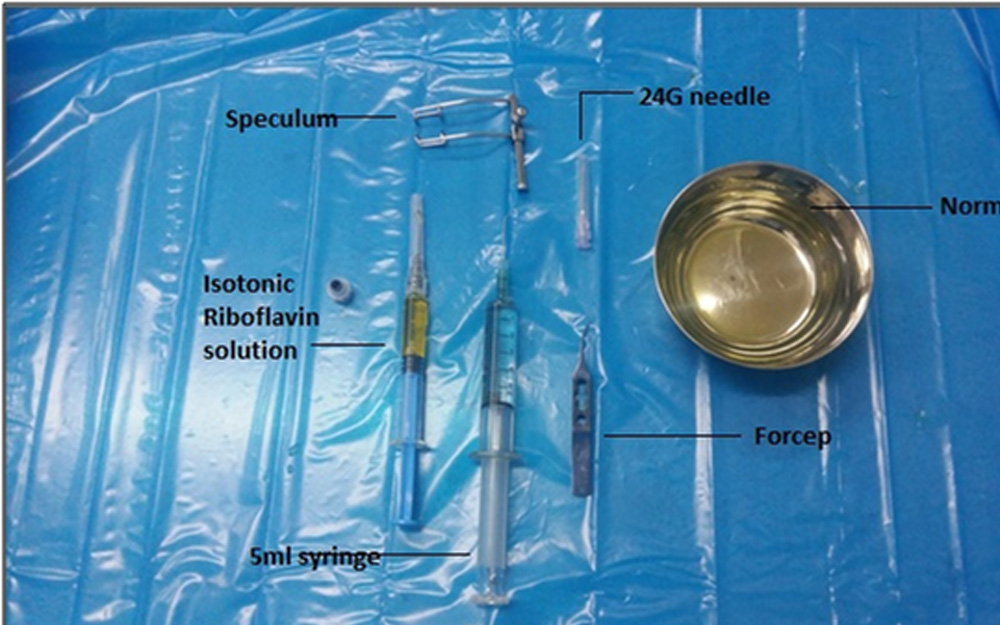
Fig. 22: Instruments used for CXLprocedure.
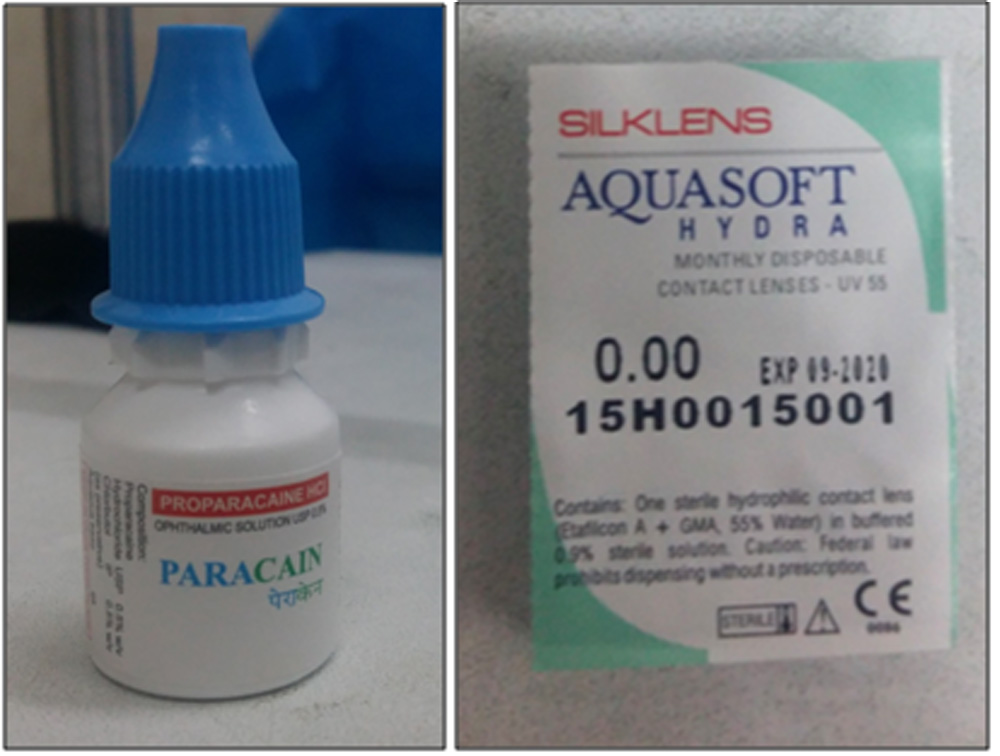
Fig. 23: Topical Anesthetic eye drop and
Bandage contact lens.
Fig. 24: Patient undergoing CXL.

Fig. 25: UV- A delivery to patient’s cornea.
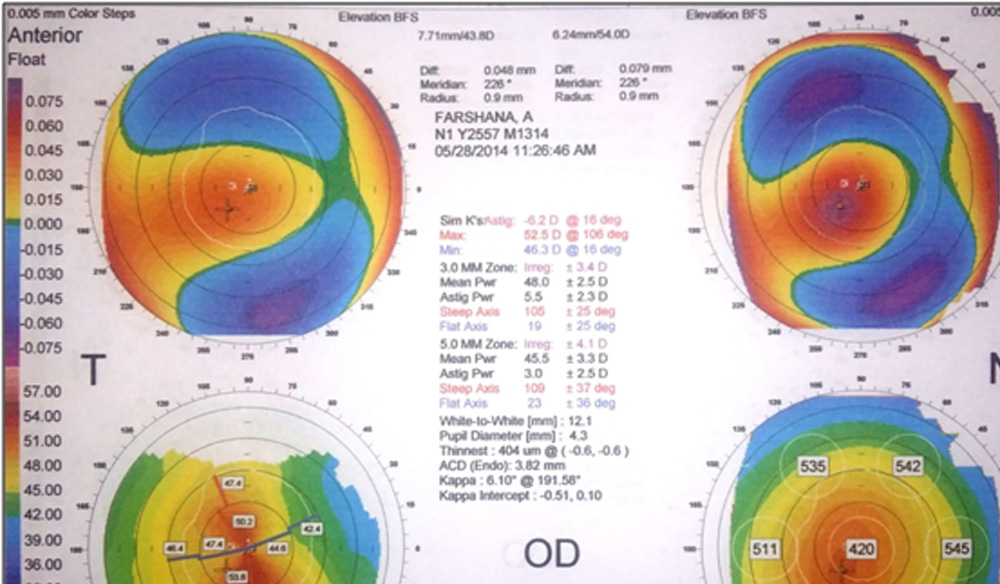
Fig. 26: Orbscan of a patient before CXL.
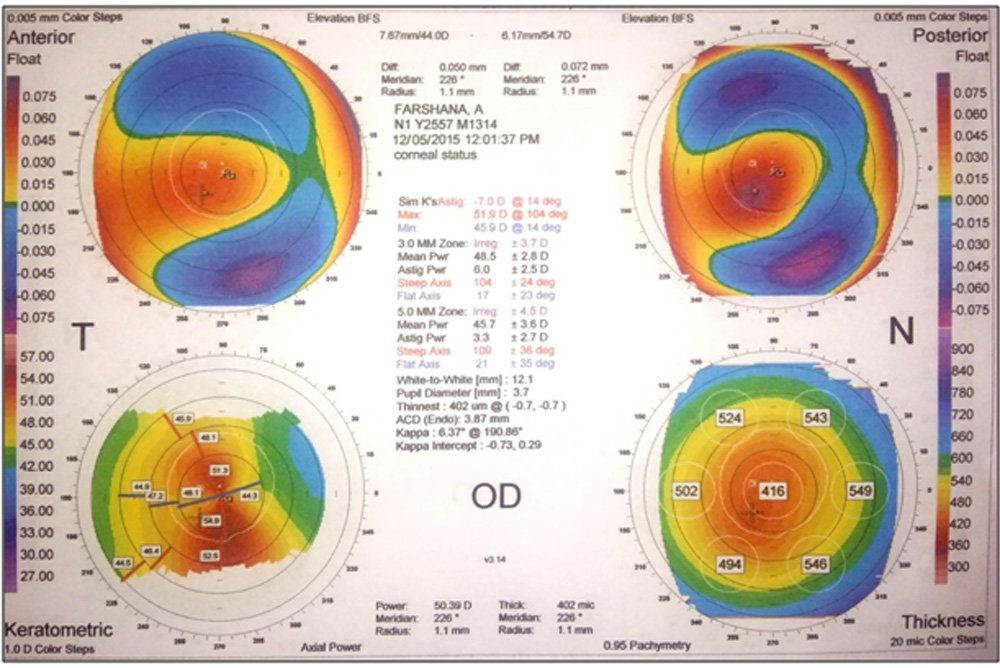
Fig. 27: Orbscan of the same patient at 18 months after CXL.
COLOUR PHOTOGRAPHS
Leave a Comment