
Dr.Saumendra Nath Ghose, G11293, Dr. Tushar Kanti Hazra, Dr. Debashis Dutta
Introduction:
Congenital nasolacrimal duct obstruction is a very common cause of epiphora in children of 1-year age. It occurs in up to 20% of normal infants1. Most of the obstructions occur at distal end of the duct at the level of valve of Hasner. General stenosis of the duct is the second most common cause, followed by the proximal dysgenesis of the duct, which includespunctal and canalicularmaldevelopment. Ninety percent of these obstructions resolve spontaneously within the 1st year of life1,2,3. In unresolved cases probing is a very successful surgical option, though little controversy remains regarding the ideal timing of probing. Traditionally probing is a blind procedure without direct visualization and may lead to false passage formation. In this study probing was done under direct visualization by nasal endoscope and it’s utility was assessed in detection of actual anatomical site of obstruction, prevention of false passage and improving success rate of the procedure.
Material and Method:
It was a prospective interventional case series, done in a single tertiary ophthalmology institute by a single surgeon. Aim ofthe study was to assess the success rate of primary endoscopy guided probing in different age groups, to establish the cause and site of obstruction by direct visualisation and to determine role of obstruction site onover all prognosis. Inclusion criteria for the study were-1) history of watering since birth 2) age one year or more and 3) Failed fluorescein dye disappearance test(FDDT). Children with history of failed probing and association of any secondary causes like trauma, lid abnormalities etc were excluded from the study.
Surgical steps:
All the cases were done under general anaesthesia without intubation. A nasal pack soaked with 1:100000 adrenalin was placed in the nasal cavity five minutes before the procedure. Initially both upper and lower puncta were inspected under microscope to exclude atresia or stenosis. This was followed by upper punctal dilatation with a Nettleship punctum dilator. Then irrigation of the upper canaliculi with diluted fluorescein dye and examination of nasal cavity with endoscope were done simultaneously. If no free flow of dye noted, elevation of inferior turbinate or infracture was done for better visualization of the area. A 00 Bowman probe was then introduced through upper puncta and progressed to the naso-lacrimal sac. Then it was gently advanced until resistance was encountered. The site and the type (membranous or osseous) of the obstruction was noted. A steady and firm pressure by the probe was applied to overcome the obstruction.
Post operatively all patients received Tobramycin eye drops four timed daily and xylometazoline nasal drop three times daily for 7 days. They were reviewed on day 7, 1st month and 6th months post procedure.
The probing was considered successful if patients became asymptomatic with negative FDDT. The procedure was considered a failure in cases with persistent watering even after 1 month and positive FDDT.
Result:
In thisstudy 32 eyes of 24 children (8 children had bilateral NLD obstruction) were examined. Table 1 & 2 showing the sex and age distributions of the children.
Table 1:
| Sex | |||||
| Frequency | Percent | ||||
| Valid | Female | 12 | 37.5% | ||
| Male | 20 | 62.5% | |||
| Total | 32 | 100.0% | |||
Table 2
| Age | |||||
| Frequency | Percent | ||||
| Valid | 12 to 23 months | 18 | 56.3% | ||
| 24 to 35 months | 13 | 40.6% | |||
| 36 months onward | 1 | 3.1% | |||
| Total | 32 | 100.0% | |||
Intraoperative findings during procedure can be broadly divided in 5 groups-
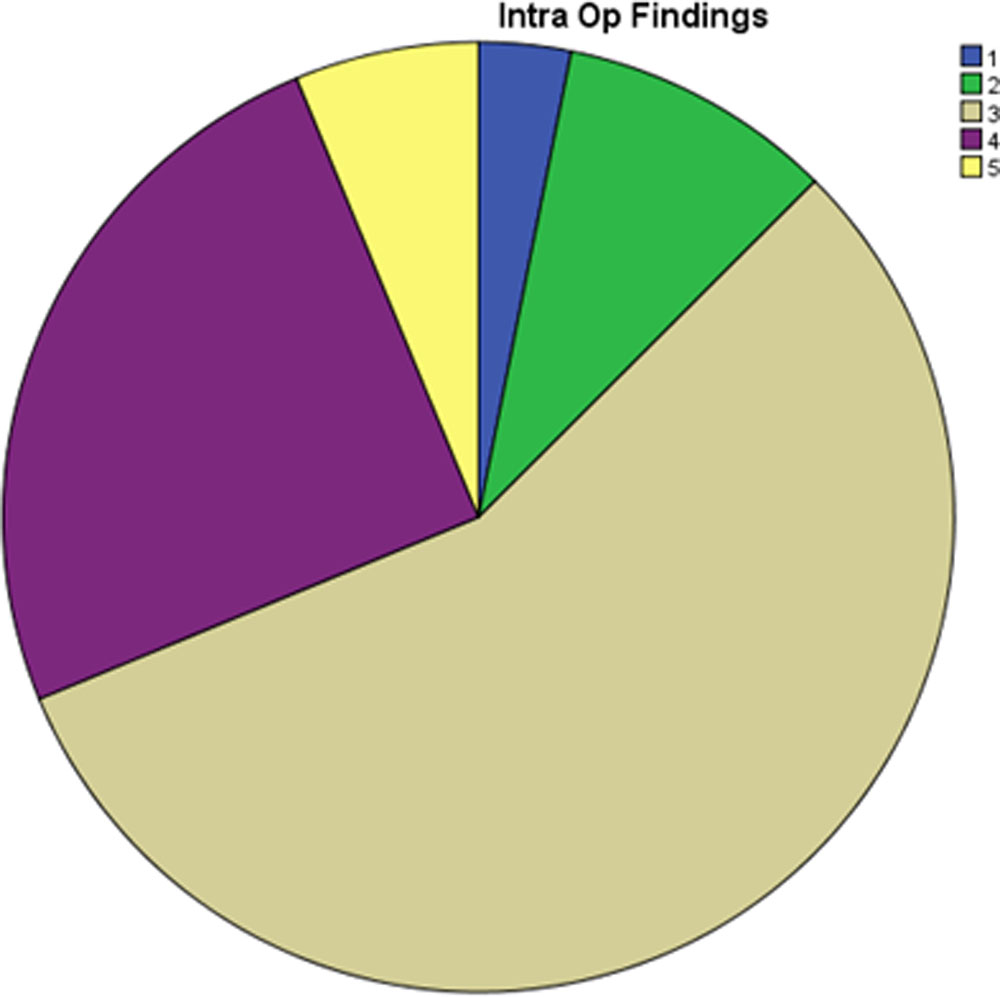
- Punctal stenosis.
- Canalicular block detected during syringing and confirmed by probing, having a soft stop at the level of canaliculi.
- Ballooning of mucosa seen during syringing and soft stop noted during probing at the level of valve of Hasnerà puncture of the mucosa was done with the probe à re-syringing confirmed the patency.
- Firm obstruction noted at the distal end à finer probe successfully penetrated.
- Firm obstruction noted at the distal end à finer probe failed to penetrate.
The following pie chart (Figure 1) shows the distribution of different type of findings during surgery.

Endoscopy guided probing was successful in 87.5%(28/32) of total cases. Location wise success rate was -100%(1/1) for punctal stenosis, 0%(0/3) for canalicular block, 100%(18/18) for distal soft NLD block and 90%( 9/10) distal bony NLD block.
We did not find any significant role of age and sex in prognosis of the procedure (p value 0.886 & 0.852 respectively). However, site of obstruction appears to play very significant role (p=0.000) in achieving success. All canalicular obstructions failed while nearly all distal obstructions were successfully treated.
Discussion:
Congenital nasolacrimal duct obstruction is a very common condition affecting 5% of infants. Persistent obstructions after age one are effectively treated with probing. Most common cause of CNLDO is membranous obstruction at the level of valve of Hasner, followed by complex causes (firm, non-membranous or complex)4-7. Membranous obstructions are easy to resolve but complex cases need more understanding of local anatomy. For this reason, success rate of blind conventional probing varied from 55-90%2,6. Although simple probing is a very safe procedure, being blind it may create false passage, cause bleeding that contribute to failure of the surgery. It is also difficult to locate actual site of obstruction by conventional method. Endoscopy guided probing on the other hand allows direct visualization of the site. Thereby it minimises chance of false passage and related complications. As it allows us to intervein, if necessary, during primary procedure, it increases the success rate of probing. It also increases our understanding regarding the cause of failure in a particular case and thus prognosticate, thereby reducing chance of replication of same/ second procedure in future8.
Conclusion:
Endoscopy guided probing allows direct visualization of nasal structures and gives clear idea about the site of obstruction. Site of obstruction is a major determining factor in the success of probing.
Reference:
- MacEwen CJ, Young JDH. Epiphora in the first year of life.Eye 1991;5:596–600
- Katowitz JA, Welsh MG. Timing of initial probing and irrigationin congenitalnaso-lacrimal duct obstruction.Ophthalmology 1987;94:698–705.
- Paul TO. Medical management of congenital naso-lacrimalduct obstruction. J PediatrOphthalmol Strabismus 1985;22:68–70.
- Kushner BJ. Management of nasolacrimal obstruction in children between 18 months and 4 years old. JAAPOS 1998; 2:57-60.
- Honavar SG, Prakash VE, Rao GN. Outcome of probing for congenital nasolacrimal duct obstruction in older children. Am J Ophthalmol2000; 130:42-48.
- Kashkouli MB, Beigi B, Parvaresh MM, Kassaee A, Tabatabaee Z. late and very late initial probing for congenital nasolacrimal duct obstruction: What is the cause of failure? Br J Ophthalmol2003; 87:1151-3.
- Robb RM. Success rates of nasolacrimal duct probing at time intervalsafter 1 year of age. Ophthalmology 1998; 105:1307–1310.
- C J MacEwen, J D H Young, C W Barras, B Ram and P S White. Value of nasal endoscopy and probing in the diagnosis and management of children with congenital epiphora. Br J Ophthalmol2001 85: 314-318
Leave a Comment