
Dr. Lional Raj D, L16453, Dr. Amar Agarwal
Aim
To compare Femto laser assisted crosslinking outcomes with conventional procedures and to prove the concept of deeper stromal crosslinking better dampens progression of ectasias
Materials and Methods
Prospective, non randomized, comparative clinical trial carried out at the department of Cornea and Refractive surgery at Dr. Agarwal’s Eye Hospitals, Tirunelveli, South India. An institutional review board approval was obtained. Informed consent procedure was carried out for each enrolled subjects before any study related procedures.
Major Inclusion criteria: Progressive keratoconus, based on topography and clinical grounds, Thinnest pachymetry over 400 microns, age between 15 and 30 years, specular endothelial cell density (ECD) more than 2000 cells per mm2.
Exclusion criteria: Scarred keratoconus, progressive post lasik ectasias, peripheral corneal degenerations, aborted keratoconus, thin corneas where CXL is contraindicated, pregnant and breast feeding women, patients with immune system disorders.
In conventional group, patients were subjected to a standard epi-off procedure under topical anesthesia, in which a blunt knife was used to remove the epithelium, isotonic riboflavin 0.1 % w/v applied every 2 minutes for 25 minutes followed by UV irradiance for 30 minutes (Appasamy CXL-CL) during which riboflavin was applied every 2 minutes (Dresden protocol of 3mW per cm2). Post operative bandage contact lens were applied.
In Femtosecond CXL group, a stromal bed (140 to 160 microns deep, 8.5 to 9.0 mm in diameter) with two incisions 180 degrees apart was fashioned (Figure 1A). The bed and the incisions are opened up, isotonic riboflavin 0.1 % w/v infused into the bed every 5 minutes (Figure 1B), in addition to trans epithelial application (Figure 1C) every 2 minutes for 25 minutes followed by UV irradiance (Figure 1D) for 30 minutes during which riboflavin was applied every 2 minutes. Finally the bed was washed with balanced salt solution (Figure 1E).
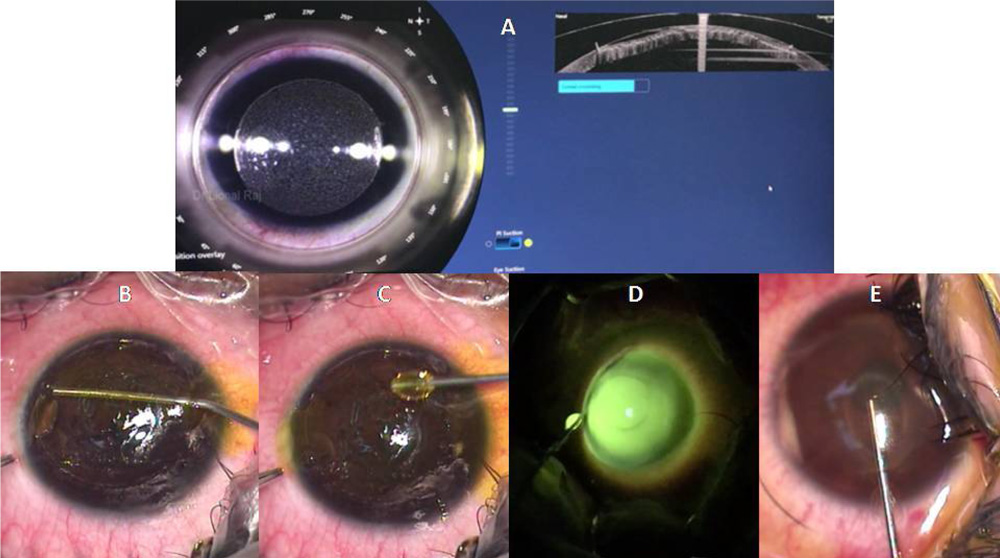
Figure 1 Procedure of FEMTO CXL
Pre operative and post operative variables of uncorrected visual acuity (UCVA) and best corrected visual acuity (BCVA) in Log MAR, simulated astigmatism (Sim K), corneal elevations in relation to Kmax and Kmean in diaptors, minimal central corneal thickness in microns, depth of demarcation line (DL) in microns, specular microscopy for ECD analyses were done. Follow up was 1 year. Corneal OCT was done at 1 month for detection and measurement of demarcation line, corneal thickness measurements, topography by ORB Scan II were done at 6 and 12 months post surgery.
The endpoints are expressed in mean +/- standard deviation. Difference between preoperative and post operative BCVA, UCVA, minimal corneal thickness, SimK, K max and K mean were compared using paired student t test for both conventional and femto CXL groups individually. This difference in each variables was again tested for statistical significance between both groups using a Independent student t test. Demarcation line depth was compared with historical data using one sample t test. Level of significance was set at p value <0.05.
Results
25 Femto-CXL, 21 Conventional-CXL eyes enrolled, and followed-up for 1year.
Table 1 Comparison between pre and post operative visual acuities
| Visual Acuity | Femto CXL | Conventional CXL | |||||||||
| (LogMAR) | Mean | S.D | 95% CI | P value | Mean | S.D | 95% CI | P value | |||
| Lower | Upper | ||||||||||
| Lower | Upper | ||||||||||
| BCVA | Pre OP | 0.243 | 0.18 | -0.0385 | 0.0991 | 0.364 | 0.277 | 0.18 | -0.021 | 0.162 | 0.126 |
| Post OP | 0.213 | 0.16 | 0.206 | 0.13 | |||||||
| UCVA | Pre OP | 0.81 | 0.28 | 0.0588 | 0.2741 | 0.005 | 0.742 | 0.36 | -0.037 | 0.247 | 0.139 |
| Post OP | 0.65 | 0.26 | 0.637 | 0.32 | |||||||
Table 2 Comparison of changes in visual acuity following Femto CXL and Conventional CXL
| Visual Acuity Difference | Mean | S.D | 95% CI | P value | ||
| Lower | Upper | |||||
| BCVA | Femto CXL | 0.03 | 0.13 | -0.156 | 0.075 | 0.486 |
| Conventional CXL | 0.07 | 0.2 | ||||
| UCVA | Femto CXL | 0.16 | 0.2 | -0.118 | 0.241 | 0.495 |
| Conventional CXL | 0.1 | 0.31 | ||||
Table 3 Comparison of pre and post operative minimal corneal thickness
| Minimal Corneal Thickness | Femto CXL | Conventional CXL | ||||||||
| Mean | S.D | 95% CI | P value | Mean | S.D | 95% CI | P value | |||
| Lower | Upper | Lower | Upper | |||||||
| Pre OP | 469.88 | 36.64 | -21.36 | 1.132 | 0.075 | 434.38 | 56.24 | 0.789 | 54.44 | 0.044 |
| Post OP | 480 | 32.75 | 406.76 | 66.85 | ||||||
Table 4 Comparison of changes in corneal thickness following Femto CXL and Conventional CXL
| Minimal Corneal Thickness Difference | Mean | S.D | 95% CI | P value | |
| Lower | Upper | ||||
| Femto CXL | -10.11 | 21.88 | -68.36 | -7.107 | 0.017 |
| Conventional CXL | 27.61 | 58.94 | |||
Minimal central pachymetry was maintained in Femto-CXL and reduced by 25 microns (p<0.05) in conventional-CXL. Femto-CXL was better (p=0.01) in retention of corneal thickness. Deeper stiffening reduces keratolysis and restores corneal thickness.
Table 5 Comparison of pre and post operative corneal elevations
| K Max | Femto CXL | Conventional CXL | ||||||||
| Mean | S.D | 95% CI | P value | Mean | S.D | 95% CI | P value | |||
| Lower | Upper | Lower | Upper | |||||||
| Pre OP | 48.88 | 2.01 | 0.523 | 1.088 | <0.0001 | 51.24 | 3.99 | 0.265 | 1.125 | 0.003 |
| Post OP | 48.08 | 2.01 | 50.55 | 4.14 | ||||||
Both Femto and Conventional CXL flattened corneas significantly
Table 6 Comparison of changes in corneal elevations following Femto CXL and Conventional CXL
| K Max Difference | Mean | S.D | 95% CI | P value | |
| Lower | Upper | ||||
| Femto CXL | 0.8 | 0.54 | -0.414 | 0.635 | 0.672 |
| Conventional CXL | 0.69 | 0.94 | |||
No significant difference in both groups.
Table 7 Comparison of pre and post operative mean keratometry in FEMTO CXL group
| K Mean | Femto CXL | ||||
| Mean | S.D | 95% CI | P value | ||
| Lower | Upper | ||||
| Pre OP | 46.65 | 1.9 | 0.72 | 0.66 | 0.018 |
| Post OP | 46.28 | 1.82 | |||
Femto CXL improved mean K significantly.
Table 8 Comparison of pre and post operative astigmatism
| Sim K | Femto CXL | Conventional CXL | ||||||||
| Mean | S.D | 95% CI | P value | Mean | S.D | 95% CI | P value | |||
| Lower | Upper | Lower | Upper | |||||||
| Pre OP | 4.09 | 1.36 | -0.263 | 0.71 | 0.345 | 4.95 | 2.49 | -1.16 | 0.619 | 0.532 |
| Post OP | 3.87 | 1.3 | 5.22 | 2.54 | ||||||
Table 9 Comparison of changes in astigmatism following Femto CXL and Conventional CXL
| Sim K Difference | Mean | S.D | 95% CI | P value | |
| Lower | Upper | ||||
| Femto CXL | 0.22 | 0.94 | -0.55 | 1.54 | 0.346 |
| Conventional CXL | -0.27 | 1.95 | |||
Astigmatism reduced in Femto-CXL by 0.25D and increased by 0.27D in conventional-CXL was only a clinical relevance with no statistical significance
Table 10 Comparison of depth of demarcation line in microns following Femto CXL and Conventional CXL
| DL | Mean | S.D | 95% CI | P value | |
| Lower | Upper | ||||
| Femto CXL | 393.6 | 34.15 | 162.85 | 196.81 | <0.0001 |
| Conventional CXL | 243.8 | 15.86 | |||
DL detected at 1 month, deep in Femto-CXL (393.6 +/- 34.1 microns) versus (243.8 +/- 15.9 microns) in conventional-CXL (p<0.0001). Femto CXL stiffens posterior cornea as well.
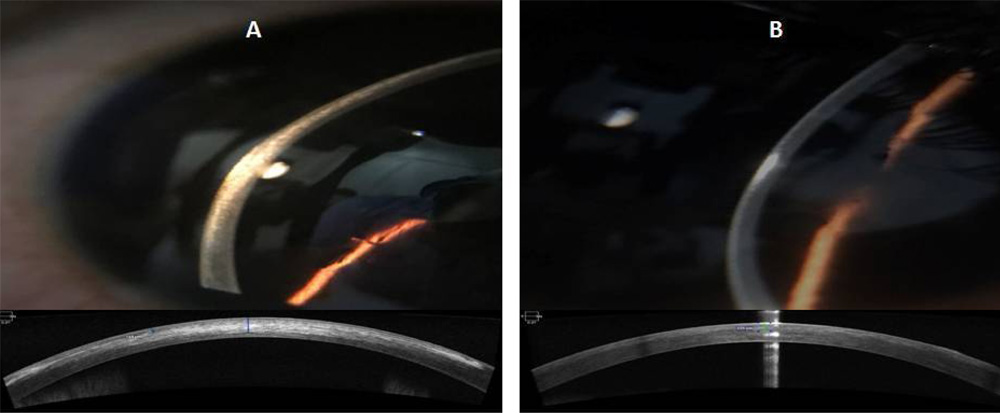
Figure 2 Depth of demarcation line in microns at 1 month, clinically and by AS-OCT (A-Femto CXL, B-Conventional CXL)
Table 11 Comparing the present study with historical controls of DL by various cross-linking techniques
| Study | Patients (N) | CXL protocol | DL depth |
| Lional Raj D | 21, 25 | Conventional, Femto CXL | 243 µm, 393 µm |
| Seiler and Hafezi | 16 | Conventional | 300 µm |
| Doors et al | 28 | Conventional | 313 µm |
| Yam et al | 40 | Conventional | 281 µm |
| Filippello et al | 20 | Transepithelial | 100 µm |
| Kymionis et al | 16 | Conventional vs accelerated | 351 µm, 288 µm |
| Mazzotta et al | 20 | Accelerated PL vs CL | 215 µm PL, 160 µm CL |
| Moramarco et al | 60 | Accelerated PL vs CL | 213 µm PL, 149 µm CL |
| Bonnel et al | 12 | iontophoresis | 247 µm |
| Kymionis et al | 29 | Conventional vs accelerated | 342 µm, 313 µm |
| Bikbova and Bikbov | 119 | Conventional vs iontophoresis | 292 µm, 172 µm |
Femto stromal bed enables deeper crosslinking than any other modalities
Table 12 Comparison of changes in endothelial health following Femto CXL and Conventional CXL
| Endothelial Analysis | Femto CXL | Conventional CXL | P value | ||
| Mean | S.D | Mean | S.D | ||
| Cell Density (per sq..mm) | 2523.19 | 312.54 | 2566.31 | 261.38 | 0.675 |
| Coefficient of Variance | 35.19 | 6.74 | 35.44 | 7.89 | 0.924 |
| Hexagonality (percentage) | 54.44 | 11.31 | 49.81 | 10.55 | 0.241 |
No endothelial changes noted in either groups
Conclusions
Crosslinking of posterior corneal stroma deeper than 250 microns could be achieved with Femto laser assisted CXL than any other conventional procedures, thus favoring an effective stabilization of keratoconus in terms of preventing steepening and further thinning of cornea, as a proof of “Deeper the Better” concept.
Leave a Comment