
Dr. Madhusmita Das, M20255, Dr. Suchismita Satpathy, Dr. Diptimayee Nayak, Dr. Sumita Mohapatra
INTRODUCTION
Glaucoma is the 2nd most common cause of blindness worldwide. But blindness due to glaucoma is preventable. Prevention of glaucoma related blindness may significantly reduce the world blindness burden. But this is not easy practically due to silent nature of the disease. Somost of the patients are presented late with advanced stage where irreversible damage has already occurred.
Most common type of glaucoma with late presentationis primary open angle glaucoma. Other causes are also there like, angle closure glaucoma, pseudoexfoliation glaucoma,neovascular glaucoma,pigmentary glaucoma which can also cause advanced damage. Higher contribution of POAG may be due to asymptomatic progression of disease. As the disease often causes peripheral visual field constriction,it is difficult for the patients to appreciate it. On the other hand, clinical course of angle closure is more likely to cause symptoms. But if not treated correctly,more risk of blindness in ACG. Pseudoexfoliationglaucoma is also a risk factor for late presentation and more difficult to manage clinically.
Poor compliance to treatment and irregular follow up are other important causes for glaucoma progression. Glaucoma requires very long duration treatment, so patients often stop using regular medications either may due to its high cost or may be due to unawareness of disease severity. Patients who belong to remote areas and with low income can’t visit the ophthalmic clinic regularly.
Comprehensive ocular examination is necessary for all patients who are coming in contact with ophthalmic care. So more number of glaucoma cases can be identified earlier. Casesshould be counselled properly about disease severity and treatment plan. Glaucoma suspects should be advised for regular follow up. Family members of patients should also be screened for the disease as some glaucoma runs in families.
AIM-
Study ofsocial factors responsible for late presentation in glaucoma focusing on which blindness can be prevented.
Method–
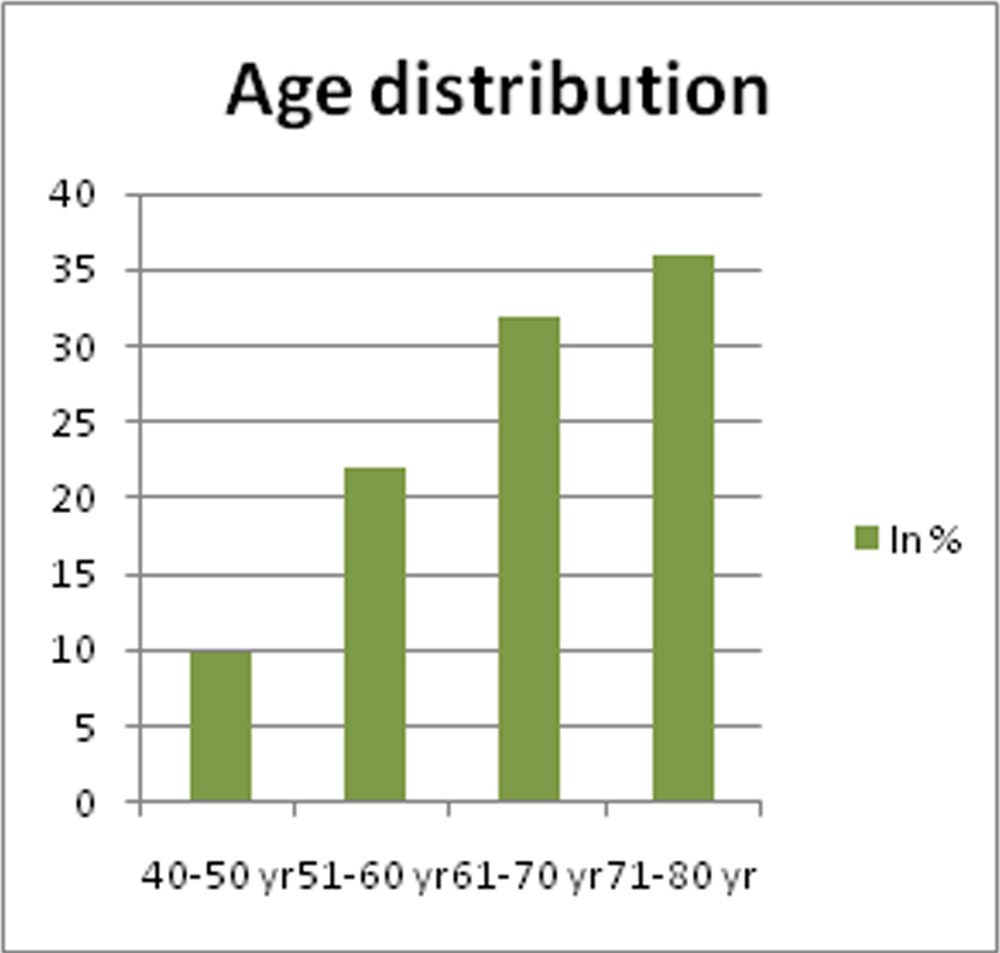
The study includes 42advanced glaucoma cases between 40-80 years of agewho attended a regional institute of ophthalmology fromSeptember 2016-March 2017. Proper history was taken including duration of onset of symptoms, family history and treatment history. Also data regarding frequency of visit to ophthalmic care, annual income,and distance of patient from ophthalmic care,educational status, and awareness level about glaucoma are recorded. Thendetailed ophthalmic evaluation of patients including visual acuity, IOP measurement, slit lamp examination along with +90 D lens evaluation, fundoscopy, and perimetrydone.Advanced glaucoma cases with near total cupping and glaucomatous visual field abnormalities in both hemifields, and or loss within 5 degree of fixation in at least one hemifield were taken into study.
Statistical analysis and results-
Analysis
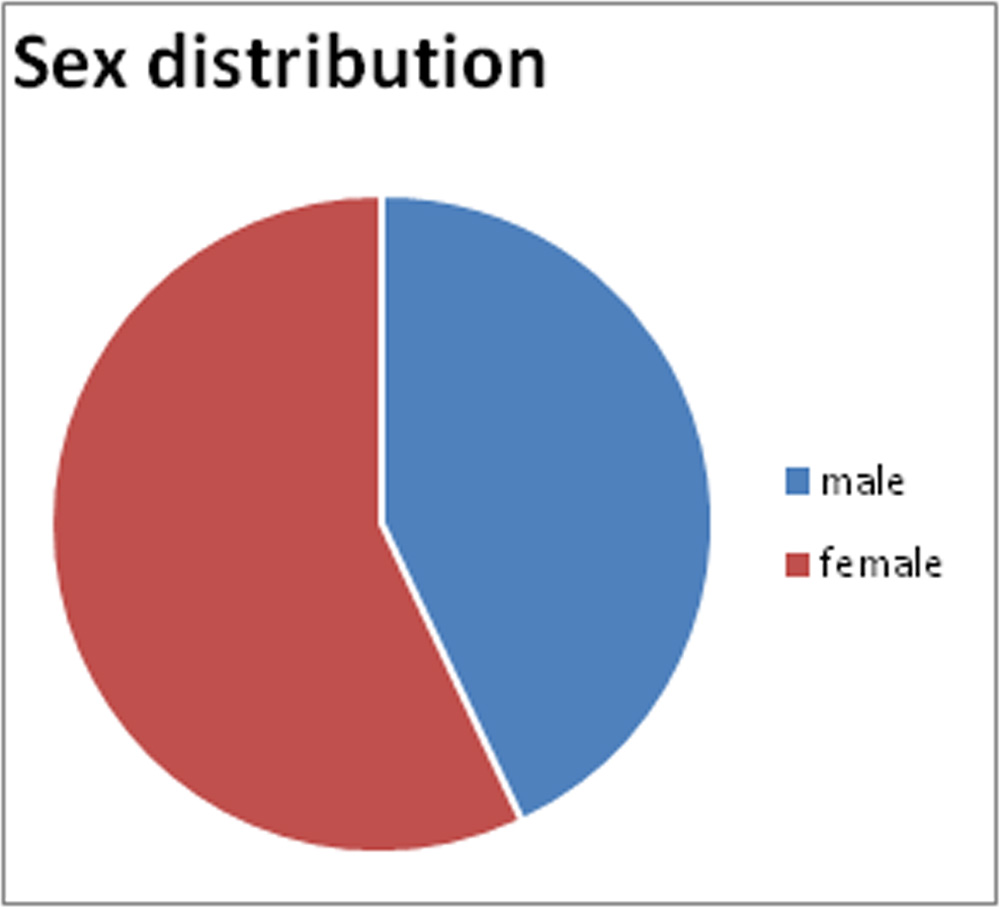
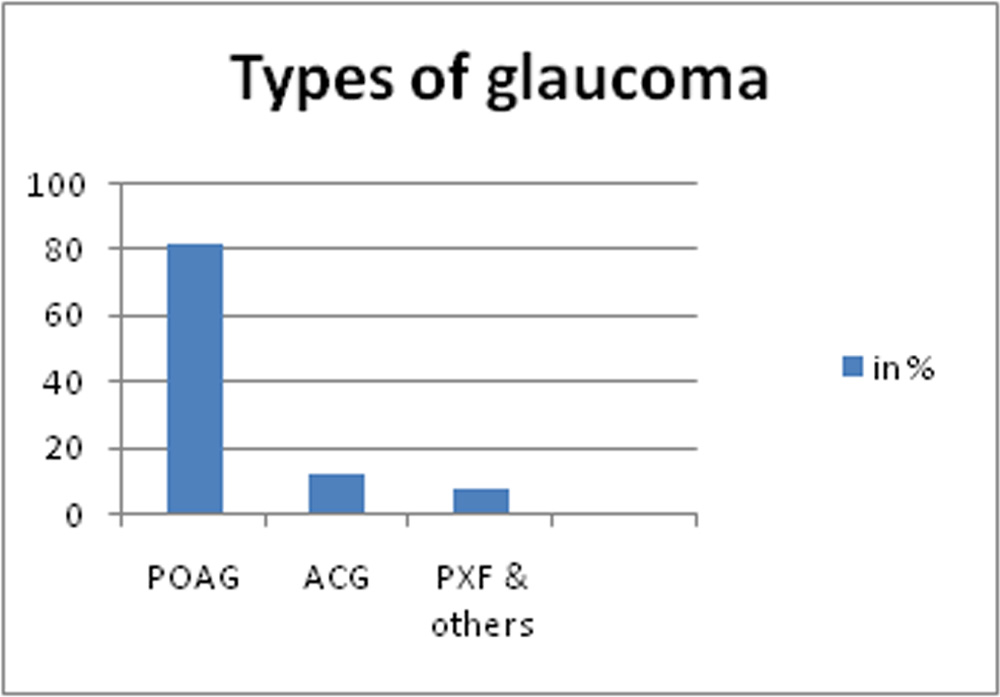
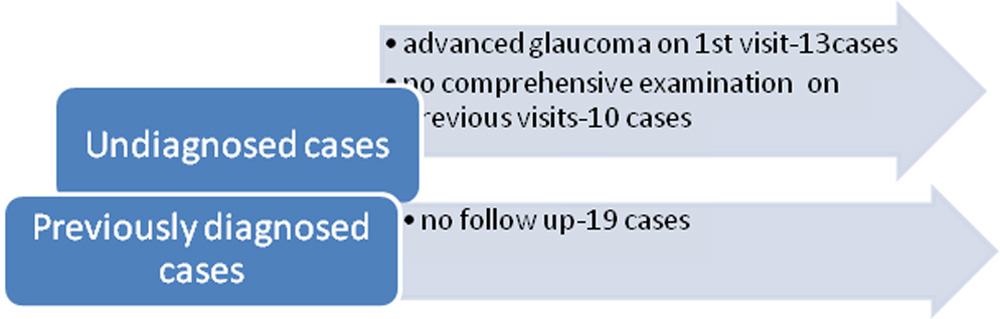
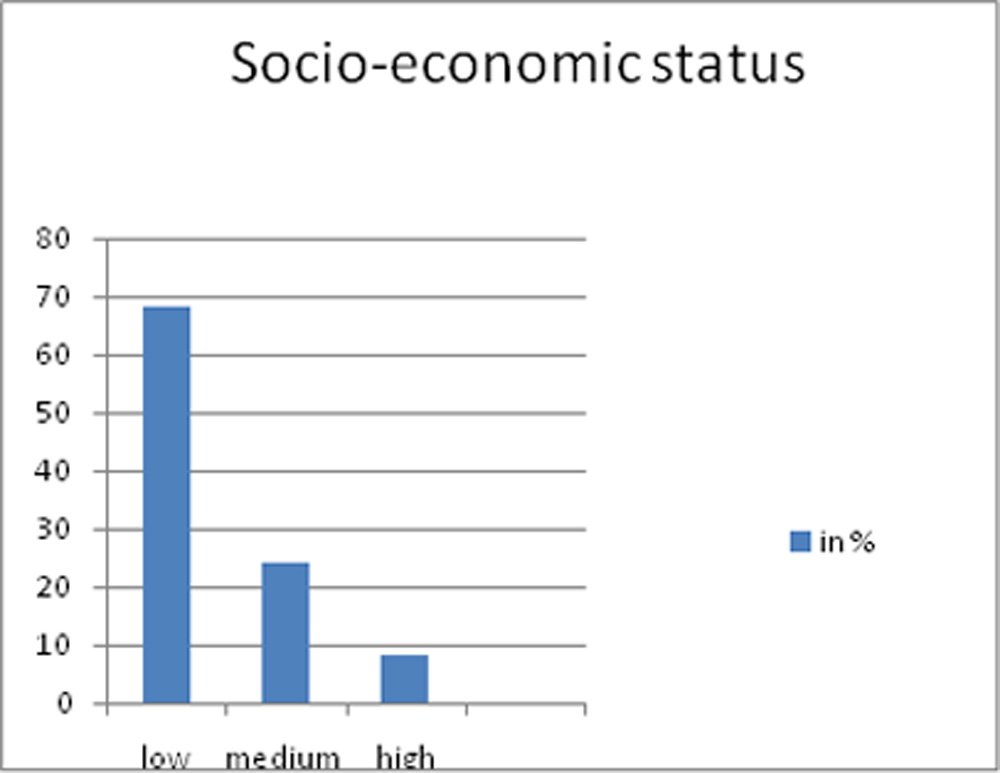
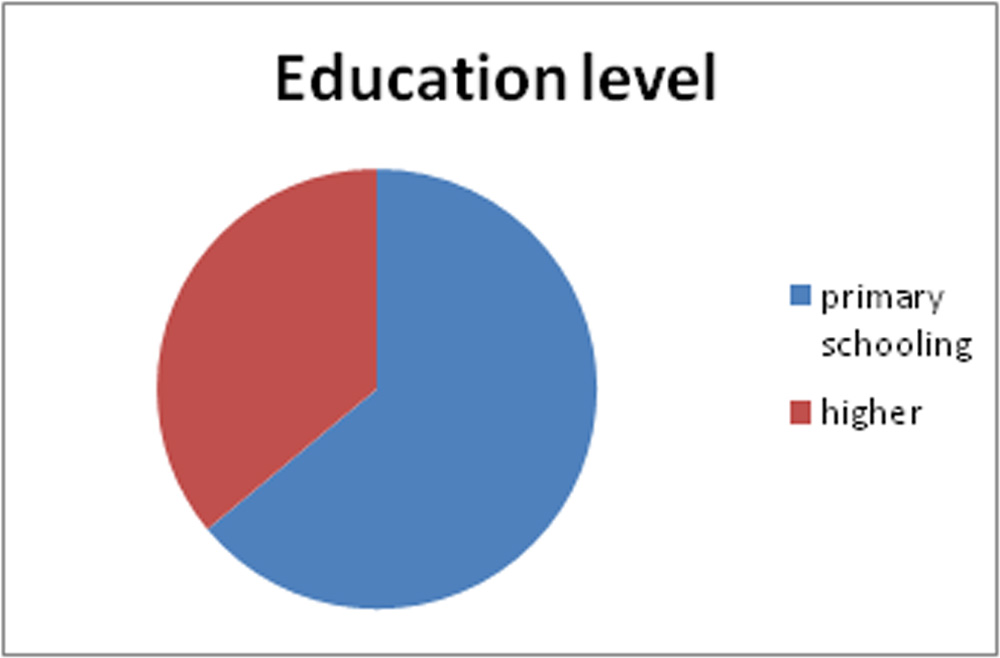
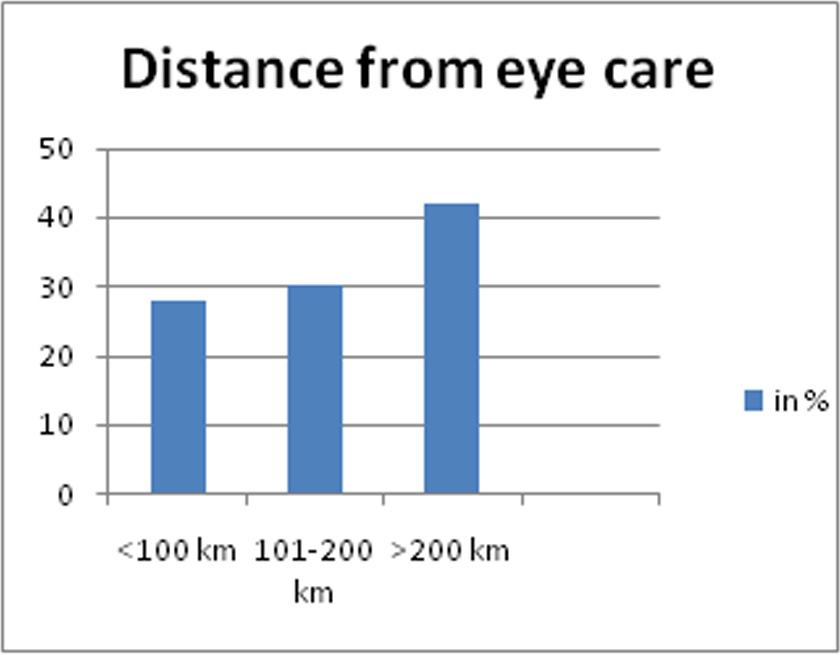
In above study, number ofcases increased with age. In higher age group due to late presentation already disease has progressed to advance stage. Male to female ratio is 0.6:1. Out of all cases studied, 81% cases are of primary open angle glaucoma, 12%cases angle closure glaucoma,7% pseudoexfoliation glaucoma and other secondary glaucomas.28% cases had advanced glaucoma on presentation. In 20% cases comprehensive ocular examination wasn’t done though they had earlier contact with eyecare.42% cases were previously diagnosed with glaucoma but discontinued medication and didn’t come for follow up.16% cases stopped glaucoma treatment after improved vision with cataract surgery. These glaucoma patients having cataract gained good vision after cataract surgery and neglected the glaucoma treatment, so presented with advanced glaucoma later. 68% cases belong to low economic class. So it is difficult for them to afford the cost of medication for long duration and regular follow up.64% cases had educational status below primary schooling.Around 72 % casesbelong to remote areas with poor transport facilities, so they had less number visits to eye care.
Conclusion –
These are the social factors which may be responsible for late presentation of glaucoma. So by curbing these factors we can prevent glaucoma related blindness. It requires adequate awareness among population about the disease symptoms, its progression, severity and importance of regular medication. It is more effective by health education at sub-centre level. Mass media involvementmay create public awareness. Also in eye care centre, comprehensive ophthalmic evaluation should be done for early detection of glaucoma cases. All known cases should be counselled properly about the importance of proper medication and regular follow up. So by early detection, proper treatment and regular follow up, we can stop disease progression and reduce the load of glaucoma related blindness.
References –
- Risk factors for late presentation in glaucoma in Iranian population, Behzad Fallahi Motlagh and Tahere Jangjou Pirbazari, Oman Journal of Ophthalmology
- Fraser S, Bunce C, Wormald R. Risk factors for late presentation in chronic glaucoma.
- Relationship between intraocular pressure and primary open angle glaucoma among white and black Americans. Arch ophthalmology
- Grant WM, Burke JF, why do some people go blind from glaucoma?
- Wilson R, Walker A, Dueker DK, Pitts-Crick R. Risk factors for late progression of glaucomatous visual field loss. Arch Ophthalmol
- Milkelburg FS,Schulzer M,Drance SM,Lau W . The rate of progression of scotomas in glaucoma.AM J ophthlmology
Leave a Comment