
Dr. Prajakta Paritekar, P16971, Dr. Dubey Nidhi
INTRODUCTION
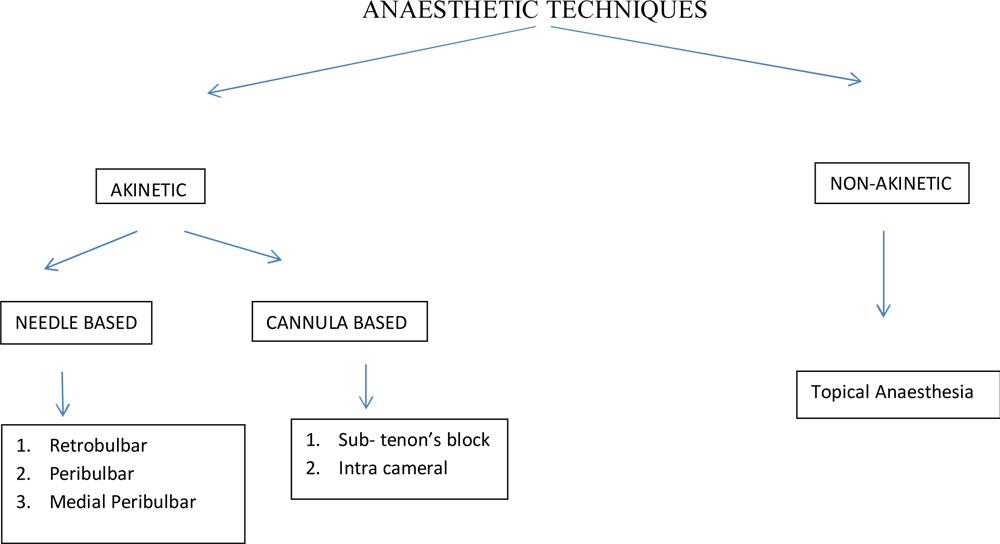
Cataract surgery is the most commonly performed surgery world wide(1). Local anaesthesia is the technique of choice for many ocular surgeries (2). In some cases especially paediatric cases or unco-operative patients, general anaesthesia is mandatory. Local anesthesia involves the blockage of a nerve supplying a given part of the body by infiltration of the area around the nerve with a local anesthetic agent (3). There are different ways of local anaesthetic techniques. Some are akinetic which are needle/canula based and some are non-akinetic like topical technique (4).Regional anaesthesia is popular among ophthalmologists because of its high success rate and wide margin of safety (5). It also ensures quicker patient recovery thus making cataract surgery a day-care procedure and also thereby minimizing the cost of the surgery (6). Peri-bulbar, retro bulbar and sub-tenon’s technique are widely used local anaesthesia techniques in cataract surgery (7). In our study we will compare Peri-bulbar and Sub-tenon technique of local anaesthesia for cataract surgery in view of patient comfort, surgeon comfort and complications. We will analyze which technique is more cost-effective for volume based setup of cataract surgery.
AIMS AND OBJECTIVES:
To compare:
- Pre- operative and post – operative pain and to grade it according to Visual Analogue Scale.
- Akinesia
- Duration of surgery (including the block time)
- Amount of anaesthetic mixture used.
between the two groups namely Peribulbar block and posterior sub tenon block
MATERIALS AND METHODS
This was a prospective longitudinal study consisting of 200 patients who presented to Sankara Eye Hospital, Banglore who fulfil the inclusion criteria and who were willing to participate in the study. Clearance from ethical committee was taken before commencement of the study. 200 patients were included in the study. Two groups were formulated consisting of 100 patients each. Patients were admitted as in-patients for Small Incision Cataract Surgery was performed on all the patients. Patients belonging to Group 1 were administered Peribulbar block and those of group 2 were given Posterior Sub-tenon anaesthesia. All cases were operated by single surgeon.This study was conducted over a period of 10 months from October 2016 to June 2017.
MATERIALS:
- Snellen’s visual acuity chart for testing vision and pre-operative refraction was done.
- TOPCON slit lamp Model no. SL 2G for detailed anterior segment examination and grading of cataract.
- Posterior segment was evaluated using Volk 90D lens.
- GoldmannApplanation tonometer for measuring intra ocular pressure.
- TOPCON Keratometer KR 8800 for keratometry and BioMedixEchorule 2 IOL calculator for calculating IOL power using SRK/T formula.
- Microscope (Takagi OM-8 or Zeiss) for surgery.
- Lox 2% (Neon laboratories) 30ml
- InjHyanidase (Shreya pharmaceuticals) 10ml vial 1500 I.U
- Inj Adrenaline (Lakeside Laboratories) 1:1000 10ml vial
- Paracaine bottle (Sunways India Pvt Ltd)
ELIGIBILITY CRITERIA:
- Patients having senile cataract.
INCLUSION CRITERIA:
- Having any grade of cataract according to LOCS classification and whose fundus examination is possible.
- Well dilated pupil.
- Willing to come for follow up.
EXCLUSION CRITERIA:
- Un-co-operative patients (mentally retarded).
- Complicated cataract.
- Patients allergic to Lignocaine 2%.
- Patients having bleeding tendencies or taking anti-coagulant medication.
- Age <40yrs or >80yrs.
METHODS:
- Cataract assessment and fundus examination of the patients were done pre-operatively and findings were noted.
- Systemic investigations like RBS, BP, cardiovascular examination were done and anaesthetist fitness for surgery under Local Anaesthesia was taken.
- Patients were posted for Manual Small Incision Cataract Surgery (SICS) after taking written informed consent in the language that they understand.
PERIBULBAR BLOCK:
- 5ml of 2% Lignocaine + 1:1000adrenaline (0.3ml) + 1500 IU/ml hyaluronidase.
- 2 injections:
1st– inferior – trans cutaneous route- infero temporal site – along the floor of orbit using 24 gauge, 1 inch needle.
2nd– superior- trans cutaneous route – supero medial site at the superior orbital notch- along the countour of the globe.
- Digital massage was given using gauze pad for 5-10min.
- Appropriate supplemental injection was given in the medial quadrant as per the akinesia required.
- Eye was patched after the surgery.
POSTERIOR SUB-TENON BLOCK:
- Two drops of 2% proparacaine were instilled into the lower fornix.
- Patient was asked to close eyes for 1 min.
- Wire speculum was applied.
- Patient was asked to look down and in to expose the supero temporal quadrant for right eye.
- Patient was asked to look up and in to expose the infero temporal quadrant for left eye.
- Small nick was made in the conjunctiva and tenon’s capsule using conjunctival scissors in the supero temporal quadrant 10mm from the limbus for the right eye and infero temporal quadrant for left eye respectively.
- Blunt dissection was done to expose bare sclera.
- Same anaesthetic mixture was injected using a specially designed 20G blunt cannula length of the cannula 15 mm.
- Pre-operative, Intra-operative and 30min post-operative pain was assesed using visual analogue pain scale. (8)
- In peri-bulbar block pain grading was done before digital massage is given.
- Akinesia was measured using Vernier callipers with limbus being the reference point and noting the excursion of eyeball.Measurement for each quadrant was done separately and noted.
- In peribulbar anaesthesia, akinesia was assesed after digital massage for 5-10min.
- Positive pressure was graded using arbitrary grading as:
Grade 0: Absent
Grade 1: Mild
Grade 2: Moderate
Grade 3: Severe
14.Note of complications that occurred was also done.
15.Duration of surgery was noted from block to patching the eye.
RESULTS
This was a prospective longitudinal study conducted over a period of 1yr. 200 eyes comprising 100 of peribulbar group and 100 of posterior sub-tenon group were included in the study. Among the peribulbar group, 52 were males and 48 were females. In posterior subtenon group 41 were males and 59 were females. The mean age group in peribulbar group was 59 yrs and in posterior sub tenon group was 63 yrs.
The total amount of anaesthetic mixture used in peribulbar block was 8ml and in posterior sub-tenon was 3ml. This value is statistically significant (p <0.001).
The pre-operative pain score in peribulbar group was 6 (according to Visual analogue pain scale is Distressing, miserable pain) while that in posterior sub tenon group was 0 (according to Visual analogue pain scale is no pain). This value is statistically significant (p<0.0001).
The post – operative pain grading in both the groups was 0.
Sum total of extraocular movements in peribulbar group was minimum 0 tomaximum 4 whereas in posterior sub tenon group minimum was 0 to maximum 16. The mean movement in all four quadrant in peribulbar group was 0.52 and in posterior sub tenon group was 5.7. This value is statistically significant (p<0.0001)
Out of 100 patients of peribulbar block group, 73 patients had no block complications. 8 patients had chemosis, 11 had sub-conjunctival haemorrhage and 8 patients had both chemosis and sub-conjunctival haemorrhage.
Among 100 patients of posterior sub-tenon block group, 90 patients had no block complications. Seven patients had chemosis and 2 patients had sub-conjunctival haemorrhage. The number of patients in both groups who did not have complications was statistically significant (p<0.0002)
All the cases were uneventful except 1 case among posterior sub tenon group who had temporal Zonular dialysis of 2 clock hours.
None of the cases among peribulbar block group had positive pressure. Two cases among posterior sub-tenon group had positive pressure. This was statistically significant (p=0.155)
The total duration required for Peribulbar block group was 26min while that of posterior sub tenon group was 10min. This difference is statistically significant (p<0.0001)
We have also observed that older patients have less threshold of pain. In patients who have more residual movement especially posterior sub-tenon group took longer time of surgery.
CONCLUSION
This was a hospital based study carried out on 200 patients.
We conclude that:
- Peribulbar block is a more painful procedure compared to posterior sub-tenon block for cataract surgery.
- Incidence of complications is more in the peribulbar block group.
- Duration of procedure is more in peribulbar group compared to posterior sub-tenon group.
- The amount of anaesthetic mixture used is more in peribulbar group.
- Number of injections required is more. Hence more tramatizing to the patient as well as more chances of complication.
Hence we would like to emphasize that,
- Posterior sub-tenon block is more patient friendly type of anaesthesia technique especially for cataract surgery which is a routinely performed surgery in Ophthalmology.
- It is also economical as the amount of mixture used is almost half than that required for peribulbar. This is of advantage in a volume cataract surgery setup.
- Posterior sub tenon block also cuts down the duration of surgery which is prolonged in peribulbar group due to slow on set of action of the block and requirement of good massage. This is also beneficial in high volume setup where it is mandatory to achieve the daily basis target of number of surgeries.
But there are certain disadvantages of this technique. Like:
- There is a learning curve to master this technique.
- Until the technique is mastered there will be persisting extra ocular movements which may make the surgery difficult.
- Also because of pain, applying of speculum is difficult as patient tends to squeeze the eye. This causes inadequate exposure of the surgical field which may also lead to difficulty in surgery.
- As a result of improper applying of speculum eyelashes may come in the surgical field which may act as source of infection.
- Inadvertant injection of the anaesthetic can occur in the subconjunctival space.
- But all the above limitations can be overcome by mastering the technique.
DISCUSSION
Cataract surgery is widely performed ocular surgery (1). Local anaesthesia is preferred for cataract surgery world wide because of less complications and early post operative rehabilitation. Thus cataract surgery can be a called a day care procedure. With the advent of newer operative techniques like phacoemulsification, newer techniques of anaesthesia like sub-tenon or topical have been practiced by the surgeons for better patient comfort.
RELEVANT ANATOMY
ORBIT
The two bony orbits are quadrangular truncated pyramids situated between anterior cranial fossa above and maxillary sinus below. The medial walls of the two orbits are parallel to each other and lateral walls are at 90 degrees to each other. Lateral walls lie at an angle of 45 degrees to medial wall. Medial wall is in close relation with ethmoid sinus. Perforation of medial wall by needle can cause orbital cellulitis or abscess (9).
GLOBE
The globe is situated in the orbital cavity nearer to the roof and towards lateral wall. Globe is at high risk of perforation during needle blocks (4).
EXTRAOCULAR MUSCLES
There are in all 6 extraocuular muscles (4 recti and 2 obliques). Recti originate from annulus of Zinn and insert anterior to equator and obliques are inserted behind the equator. The recti are supplied by Occulomotor Nerve. To eliminate the action of the recti muscles, occulomotor nerve needs to be blocked.
FORWARD SET GLOBE
The globe extends quite forwardly over the infraorbital rim (>8 mm) and associated eyelids will be lax with wide palpebral fissure and high brows. Here, the structures in the apex of the orbit are vulnerable to get injured with needle blocks (4).
DEEP SET GLOBE
In this condition, there is high chance for the needle to come in contact with the globe. Associated eyelids will be short and tight. From the point of insertion, at the inferolateral quadrant, the needle must not be angulated more than 10° elevation from the transverse plane (4).
RETROBULBAR BLOCK
TECHNIQUE:
- After appropriate patient preparation, monitoring and positioning, Patient must be facing straight in primary gaze position.
- Inferior lid is then prepared with alcohol swab. Inferior orbital rim should be located and palpated while the globe is mildly pushed to elevate and clear the path for the needle insertion.
- Bevel of the needle should face upward towards the globe to avoid perforation of the globe.
- Needle is inserted perpendicular through the inferior eyelid at the superior edge of the inferior orbital rim in the saggital plane of the temporal limbus to avoid major vessels and decrease the risk of a retrobulbarhemorrhage. The needle is advanced parallel to the orbital floor with an inclination of 10 to 15 degrees. Approximately 1 cm after penetrating the orbital septum, posterior to the equator, the needle is redirected 30 to 45 degrees superonasal and advanced 2.5 to 3.5 cm until the intraconal space.
- Once inside the intraconal space, gently move the needle and beware of any resistance or significant rotation of the globe to assure no perforation of the globe has occurred.
- Aspirate syringe to ensure no blood return and confirm no vessels compromise.
- Slowly inject 3 to 4 ml of anesthetic and remove needle.
- With the eye closed apply resistance to the volume injected making pressure with gauzes or Honan ballon at 20 to 30 mmHg for 5 minutes to prevent a hemorrhage and increase diffusion of the anesthetic agent.
- Assess the degree of akinesia and anesthesia 5 minutes posterior to the injection.
- 23G, 31mm long needle is preferred.
COMPLICATIONS:
- Retrobulbarhemorrhage
- Ocular perforation
- Subarachnoid or intradural injection
- Diplopia secondary to miotoxicity
- Cardiorespiratory distress
- Contusion and atrophy of the optic nerve
- Vascular retinal occlusion
- Seizure
- Corneal abrasion
- Chemosis
- Ptosis
PERIBULBAR BLOCK
The first injection is given inferiorly with a 23 g needle at the junction of outer one third and inner two third of the lower orbital rim(5cc).This technique involves giving two injections of long acting anaesthetic at least 20 minutes before the surgery.TECHNIQUE:
- The second injection is given superonasally beneath the superior orbital notch(3cc) . Immediately following this injection superpinky is placed on the eye for 10-15 minutes .
- Intermittent pressure with superpinky should be given to prevent occlusion of vessels.
SUB TENON’S BLOCK
The injection is made on a supine patient with an i.v. cannula in situ.TECHNIQUE (2)
- The conjunctiva is anaesthetized with topical anaesthetic solution. An eyelid speculum should be inserted at this point to improve access.
- Throughout the procedure, the patient is asked to look up and outwards to expose the infero-nasal quadrant.
- A small tent of conjunctiva is raised with a pair of ®ne non-toothed forceps approximately mid-way between the limbus of the eye and the visible edge of the inferonasal portion of the conjunctiva.
- A small incision is made in the tented conjunctiva with a pair of ophthalmic scissors
- The closed scissors are introduced through the aperture created and a tunnel is fashioned to the bare sclera by blunt dissection through Tenon’s capsule.
- A curved, blunt irrigating cannula is then inserted with the syringe of anaesthetic solution attached.
- The cannula is introduced along the contour of the globe and gentle contact of its tip is maintained with the sclera until it lies in the posterior segment
- Occasionally, resistance to the needle is felt around the equator where a fibrous band can form as the ocular muscles broach the capsule. This is usually easily overcome by gentle pressure.
- Then the anesthetic mixture is injected
- Slight proptosis of the eyeball is normal after a correctly sited injection
- After removal of the cannula, pressure is applied by massaging the globe
COMPLICATIONS
- Chemosis
- Sub conjunctival haemorrhage
- Globe perforation (rare) if sharp cannula is used
TOPICAL ANAESTHESIA
TECHNIQUE (10)
- Use of topical drops or viscous gels
- Eye Drops: Propacaine0.5%
Tetracaine
Lidocaine
Bupivacaine
Benoxinate
Viscous lidocaine gel 2%
ADVANTAGE
- Fast recovery
- Patient friendly
DISADVANTAGE
- Topical anesthetic agents block trigeminal nerve endings in the cornea and the conjunctiva only, leaving the intraocular structures in the anterior segment unanesthetized.
- Thus, manipulation of the iris and stretching of the ciliary and zonular tissues during surgery can irritate the ciliary nerves, resulting in discomfort.
- High or prolonged doses of local anesthetic agents are toxic to the corneal epithelium, and this prolongs wound healing and causes corneal erosion.
- Also, repeated administration of drops can cause clouding of the cornea, rendering surgery more difficult.
INTRA CAMERAL ANAESTHESIA
Injecting preservative free anaesthetic mixture by a cannula into the Anterior chamber at the beginning of the surgery. (0.1 to 0.5ml)TECHNIQUE
ADVANTAGES: (10)
- injuries to ocular tissue or life-threatening systemic side-effects are minimal,
- the vision is restored instantly after the operation,
- the undesirable cosmetic side effects are avoided,
- the technique is economical, and
- there is no need for an anesthetist to be present.
REFERENCES
- Kendall E. Donaldson, Rosa Braga-Mele, Florence Cabot, Richard Davidson, Deepinder K. Dhaliwal, L.Ac, Rex Hamilton, Mitchell Jackson, Larry Patterson, Karl Stonecipher, Sonia H. Yoo. Femtosecond laser–assisted cataract surgery. J Cataract Refract Surg 2013; 39:1753–1763.
- S. Canavan, A. Dark and M. A. Garrioch. Sub-Tenon’s administration of local anaesthetic: a review of the technique. Br J Anaesth 2003; 90: 787-93.
- Ogbonnaya N. Iganga, OluyemiFasina, Charles O. Bekibele, Benedictus G. K. Ajayi and Ayobade O. Ogundipe. Comparison of Peribulbar with Posterior Sub-Tenon’s Anaesthesia in Cataract Surgery Among Nigerians. Middle East Afr J Ophthalmol2016 Apr-Jun; 23(2): 195–200.
- Jaichandran V V. Ophthalmic regional anaesthesia: A review and update. Indian J Anaesth [serial online] 2013 [cited 2016 Jul 26];57:7-13.
- McLure HA, Rubin AP. Local anaesthesia for ophthalmic surgery.CurrAnaesthCrit Care. 1999;10:40–7.
- Malik A, Fletcher EC, Chong V, Dasan J. Local anesthesia for cataract surgery.J Cataract Refract Surg. 2010;36:133–52.
- Sherry N. Rizk, Mona R. Fahim, Ehab S. El-Zakzouk .Peribulbar versus sub-Tenon block in cardiac patients undergoing cataract surgery during warfarin therapy. Egyptian Journal of anaesthesia (2014) 30, 255-59.
- Parkar T, Gogate P, Deeshpande M, Adenwala A, Maske A, Verappa K. Comparison of subtenon anaesthesia with peribulbar anaesthesia for manual small incision cataract surgery.Indian J Ophthalmol2005;53:255-9.
- A K Khurana, Aruj K Khurana.The Skull, Orbit and ParanasalSinuses .In:A K Khurana. Comprehensive Ophthalmology,4th Edition. New Delhi:New Age International (P) Limited;2007.p.249.
- Adeela Malik. Efficacy and Performance of Various Local Anesthesia Modalities for Cataract Surgery. Malik, J Clinic Experiment Ophthalmol 2013, S:1
Leave a Comment