
Dr. Mrittika Sen, S19005, Dr. Dada Tanuj, Dr. Ramanjit Sihota, Dr. Dewang Angmo
Abstract
Purpose: Comparing the efficacy of Trabeculectomy with Ologen and Mitomycin C (MMC) vs Trabeculectomy with MMC alone. Method: RCT
29 patients of primary adult glaucoma were randomized. 25 eyes in Group 1 underwent Trabeculectomy with low dose MMC (0.1mg/ml, 1 min). 25 eyes in Group 2 underwent surgery with Ologen (subscleral, subconjunctival) and low dose MMC. Absolute success-IOP</=15 without medications.
Result:
Mean highest recorded IOP (in mmHg) was 35.44+/-13.73 in Group 1 and 33.8+/-14.01 in Group 2. Mean postoperative IOP in Group 1 was 13.2+/-8.72, 12+/-6.60, 11+/-4.53 and in Group 2 was 12.4+/-6.24, 12.24+/-3.43, 13.68+/-4.78 at 1, 3 and 6 months respectively with significant reduction in IOP from baseline(p<0.001) in both. IOP reduction was not significant between groups till 6 months (p= 0.07). Absolute success was achieved in72% of patients in both the groups. There was no difference between the groups in terms of morphology of the blebs, complications and need for postoperative anti-glaucoma medications.
Conclusion:
Combined Ologen and MMC provides no additional benefit over Trabeculectomy with low dose MMC in short term IOP control in moderate to advanced primary glaucoma.
Key words: Trabeculectomy, Mitomycin C, collagen implant, Ologen, Intraocular pressure
Introduction
Glaucoma is a serious sight-threatening disorder aptly named the Silent thief of sight. It is an optic neuropathy with progressive loss of retinal ganglion cells, leading to characteristic structural damage to the optic nerve and visual field defects due to a variety of pathologies.[1]
Glaucoma is the second leading cause of blindness and is responsible for 20% of the blindness in the world and 1.5% of blindness in India. [2,3]The standard of care in glaucoma surgery is Trabeculectomy with Mitomycin C (MMC).[4]The use of mitomycin C as an adjunct in trabeculectomy was reported by Chen in 1983. [5] MMC is an antineoplastic antibiotic isolated from Streptomyces caespitosus. The anti-metabolites being used in glaucoma surgery are double- edged swords. While they help to modify the fibrotic response to surgical insult, they are associated with a number of side effects and complications such as hypotony, hypotony maculopathy, suprachoroidal haemorrhage, choroidal effusion, bleb leak, blebitis, bleb encapsulation, failure and endophthalmitis. [6,7,8,9]Ologen is a tissue engineered biodegradable collagen implant that offers viable solution to the problem of scarring. The copolymer of collagen and glycosaminoglycan allows random and loose reorganization of the regenerating myofibroblasts and extracellular matrix. [10,11] It acts as an aqueous reservoir and prevents a shallow anterior chamber. It acts as a spacer and prevents adhesion between conjunctiva and sclera. Ologen is non-teratogenic and degrades into non-toxic products in 90 to 180 days. Although recent studies have shown successful outcome in the use of these implants among Caucasian patients, a randomized controlled study among Indians is lacking. Therefore, this study was conducted to evaluate the outcome of the combined use of collagen implant with MMC among Indian patients undergoing Trabeculectomy. To the best of our knowledge, this is the first randomized controlled study in which the collagen implant is evaluated with MMC in parallel group against control group (MMC) among patients undergoing Trabeculectomy.
Materials and Methods
This was a prospective, randomized, controlled trial conducted at Dr. Rajendra Prasad Centre for Ophthalmic Sciences, between February 2016 and September 2017. The study was undertaken after approval from the institutional ethics committee and adhered to the tenets of the Declaration of Helsinki. Patients presenting to the outpatient services and Glaucoma Clinic were evaluated for the need for Trabeculectomy. The inclusion criteria were patients >40 years of age with medically uncontrolled moderate to advanced primary open angle glaucoma (POAG) or primary angle closure glaucoma (PACG) identified by IOP> 21 mmHg; glaucomatous visual field defects confirmed by 30-2 SITA Standard Humphrey visual field analysis cluster of 3 points with a probability of 5% on the pattern deviation map in at least 1 hemifield, including at least 1 point with a probability of 1%; and a Glaucoma Hemifield Test outside 99% of age-specific normal limits, and a pattern SD outside 95% of normal limits) and presence of glaucomatous optic disc. Patients with neovascular, uveitic, aphakic and other causes of secondary glaucoma, one-eyed patients, patients with history of cataract surgery in the last 12 months or previous glaucoma surgery or selective laser trabeculoplasty, pregnant or breast -feeding women and those with known allergy to Mitomycin-C or collagen were excluded. Patients were randomised into two groups; in Group 1 patients underwent trabeculectomy with low dose MMC, and in Group 2 patients underwent trabeculectomy with low dose MMC and Ologen implant. Randomization was done using a computer-generated table of random numbers. A written informed consent was obtained from each patient and they were evaluated for the age, gender, type of glaucoma, presence of systemic diseases, highest recorded intraocular pressure (IOP), number of anti-glaucoma medications. The following parameters were recorded: best corrected distance visual acuity, gonioscopy, IOP using Goldmann applanation tonometer and the visual field parameters using 30-2 SITA Standard or 10-2 and GVF wherever applicable.
Surgical Technique
All trabeculectomy surgeries were performed by a single glaucoma surgeon under peribulbar anesthesia. Under aseptic surgical technique, a corneal traction suture was placed using 8-0 vicryl and a fornix-based conjunctival flap was created. Sub-Tenon dissection and hemostasis was performed as required. Multiple sponges (n=4) soaked in a 0.1 mg/mL solution of MMC was applied for 1 minute in a diffuse area under the superior bulbar conjunctiva before dissecting scleral flap. The area was irrigated thoroughly with balanced salt solution after 1 minute. A half-thickness 5.0×5.0mm rectangular scleral flap was made in the superior area. Anterior chamber paracentesis was done.1×1 mm ostium was made. A peripheral iridectomy was performed. The scleral flap was closed with two 10-0 nylon sutures, one at each corner. In Group 2, a deep scleral crater was created using crescent blade before making the full thickness ostium. Ologen Collagen Matrix implant (cylindrical implant with a diameter of 6mm and a height of 2mm) was positioned on top of and under the scleral flap without the use of any suture. While tying suture to scleral flap on each side, a loose stitch was applied as the collagen implant swells up on soaking aqueous and tamponades against the scleral flap preventing excessive outflow. The conjunctiva was closed with 8-0 polyglactin vicryl suture. The postoperative regimen consisted of topical antibiotics 4 times-a-day, steroid drops that were tapered over 6-8 weeks and tropicamide cycles twice a day.
The patients were followed up on day 1, day 7 and at 1, 3 and 6 months post-surgery. At each of the visits the IOP was measured using Goldmann Applanation Tonometer, the bleb morphology was evaluated using Indiana Bleb Appearance Grading Scale and AS-OCT was done at 1, 3 and 6 months. AS-OCT of the blebs was performed using the Visante time domain OCT. A visual field was repeated at 6 months.
Primary outcome measure was measurement of the intraocular pressure with absolute success being defined as IOP ≤15 mmHg without any anti-glaucoma medication and qualified success defined as postoperative IOP ≤15 mmHg with anti-glaucoma medication. Secondary outcome measures included the need for postoperative anti-glaucoma medications, complications, need for adjunctive procedures like needling and evaluation of the bleb morphology.
Statistical Analysis
The data was recorded in Microsoft Excel Spreadsheet. Analysis was done using Stata software version 12 and SPSS. Chi square test or Fischer exact test was applied for the qualitative data.
Student’s t-test, Wilcoxon Rank-Sum test for continuous variables. A p value < 0.05 was considered as significant.
Results
A total of 50 eyes of 50 patients were included in the study and randomized into 2 groups: 25 eyes to trabeculectomy with low dose MMC group and 25 eyes to trabeculectomy with combined Ologen and low dose MMC group. The mean age of the patients in group 1 was 55.96±8.46 years (range, 40 to 72 years). Of these, there were 12 males and 13 females. Similarly, in group 2 the mean age of the study participants was 60.12±7.46 years (range, 60 to 46 years). There were 16 males and 9 females. The two groups were comparable in terms of the baseline parameters and these are summarized in Table 1.
The mean highest recorded preoperative intraocular pressure in group 1 was 35.44±13.73mmHg and in group 2, it was 33.8±14.01mmHg, (p=0.72). There was a significant reduction in IOP at all postoperative visits in both the groups as compared to the baseline (p<0.001). There was mean reduction of 62.8% in the IOP in group 1 and 54.97% in group 2 at the end of 6 months. There was no statistically significant difference between the two groups in terms of IOP at any point of time (Table 2).
The BCVA was reduced to 1.18±1.45 at 6 months in group 1 and 0.74 ± 0.58 in group 2 but it was not statistically significant (p=0.07). The mean deviation on Humphrey Visual Field Analyzer (SITA Standard) increased to -23.35 ± 9.99dB in group 1 and -28.15 ± 2.92dB in group 2 which was again not significant as compared to the baseline values(p=0.668).
There was a significant reduction in the need for anti-glaucoma medications in the post-operative period in both the groups (p<0.001) with19 patients in group 1 and 21 patients in group 2 being off ocular hypotensives at the end of 6 months of follow up. The mean number of drugs reduced significantly from 3.64±0.67 and 3.2±0.92 in the preoperative period to 0.52±1.06 and 0.24±0.64 in group 1 and group 2 respectively in the postoperative period. Six patients in group 1 and four patients in group 2 had to be started on anti-glaucoma medications in the postoperative period.
Overall success rate was 84% in Group 1 and 76% in Group 2 at the end of 6 months. 18 patients in each group had an IOP of ≤15mmHg without any anti-glaucoma medication at the end of 6 months. Qualified success was attained by 3 patients in group 1 and 1 patient in group 2. There was no statistically significant difference between the success rates of the two groups at 6 months (p=0.583).
Both the groups were similar in terms of bleb morphology in each of the follow up visits with majority of the blebs being moderately elevated, mildly vascular and having an extent of 2-4 clock hours as per IBAGS. In the Ologen group there were more blebs (3 V3 and 1 V4 blebs) with moderate to extensive vascularization. The blebs in group 1 were more diffuse with 3 blebs having an extent of >4 clock hours. However, this difference in morphology was not statistically significant. The internal structure of the blebs was assessed with AS-OCT. The mean total height and the height of the suprascleral fluid cavity of the blebs was more in the Ologen group at 1, 3 and 6 months but was statistically significant (two sample t-test) at only 1 and 3 months (p<0.05). There was no significant difference between the two groups in the thickness of the bleb wall or the radial width measured from the limbus towards the fornix.
Complications
Two patients in group 1 and 3 patients in group 2 had a shallow anterior chamber within 2 weeks of the surgery with no leak (Seidel test negative) and required AC reformation. One eye in group 1 and 2 eyes in group 2 developed Tenon cysts, all of them presenting within 4 weeks of surgery. These were managed with needling with 5 mg 5-FU injection. One patient in group 1 had to undergo a re-trabeculectomy with 0.2mg/ml MMC at the end of 3 months of follow up.
Discussion
Patients with moderate or advanced glaucomatous optic neuropathy often need surgery to achieve low ‘target’ IOPs. The Advanced Glaucoma Intervention Study, the Early Manifest Glaucoma Trial, and the Ocular Hypertension Treatment Study have demonstrated that lower IOP is associated with a reduced risk for progression of visual field damage.[12,13,14]Surgical management for glaucoma is usually reserved for cases that are unresponsive or noncompliant to medical therapy or in which target pressure cannot be achieved despite maximum tolerable medical therapy. Trabeculectomy augmented with MMC is the most commonly performed surgery for glaucoma. The anti-proliferative agents like 5-fluorouracil and MMC have improved the success rate of glaucoma filtration surgeries. A Cochrane review has shown that MMC application in primary trabeculectomy surgeries lowers the IOP significantly.[15] The dose of MMC used in literature has varied from 0.1 to 0.5 mg/ml and in exposure time from 0.5 to 5 min. While it reduces fibrosis on one hand, it leads to a number of complications like hypotony, bleb leaks, blebitis, and a significant loss of vision. Higher dose and duration of exposure of MMC has been reported to lead to lower IOPs and better success of trabeculectomy but the associated complications are also more. Sihota et al showed in their prospective randomized study that 0.1 mg/ml MMC is non-inferior to 0.2 mg/ml MMC in achieving low ‘target’ IOPs in primary adult trabeculectomy surgeries and is probably a safer alternative, as thinning of the bleb is significantly less frequent in the long term. [4]
Ologen, is a porous biodegradable collagen polymer. The pores, having a size of 10 to 300µ, guide the fibroblasts to grow through the body of the implant randomly and reduce formation of an organized scar.
A number of studies have been undertaken to evaluate the role of Ologen as a substitute for the anti-metabolites as an adjunct in trabeculectomy. Aptel et alreported that deep sclerectomy with Ologen implantation is effective.[16] However, the results of trials of trabeculectomy with Ologen alone as an adjunct have not been encouraging. In a prospective randomized study by Rosentreter et althey noted that the success rate in the trabeculectomy with Ologen group was half of that of the trabeculectomy with MMC group.[17] But the blebs were more vascular as compared to the ones in the MMC group. Cillino and colleagues performed a five year follow up study comparing Ologen and MMC (concentration: 0.2mg/mL) as adjuncts in trabeculectomy. There was no significant difference between the two groups in terms of IOP lowering effect, bleb morphology on SD-OCT or the safety profile.[18] Papaconstantinou et aldid not find any significant difference between patients undergoing trabeculectomy alone and those who underwent trabeculectomy with Ologen in a randomized controlled trial.[19] In our study, we evaluated the results of conventional trabeculectomy with low dose MMC (0.1mg/ml for 1 minute)with trabeculectomy using subconjunctival and subscleral Ologen implantation combined with low- dose MMC.
The intraocular pressure was reduced significantly from the baseline in both the groups. There was no statistically significant difference between the two groups in terms of their ability to lower the intraocular pressures in patients with moderate to advanced glaucoma. Overall success was achieved in 84% of the patients in group 1 and 76% of the patients in group 2 with 72% of the patients achieving absolute success in either group at the end of 6 months. There was 62.8% reduction in IOP in the MMC group which was more as compared to 54.97% reduction achieved by the Ologen and MMC combination group but not statistically significant. In the sub-group analysis, the success rate was similar in patients with POAG (83.33%) and PACG (76.92%).
Six patients in Group 1 required at least one ocular hypotensive medication in the postoperative period. In group 2, four patients had to be started on anti-glaucoma medications. In terms of complications, the two groups were again similar. Two patients in group 1 and 3 patients in group 2 had a shallow anterior chamber within 2 weeks of the surgery due to over-filtration. Anterior chamber reformation was done for the patients. Early conjunctival leakage was reported by Rosentreter et alin 30% of their cases undergoing trabeculectomy with Ologen implantation.[17] It is important that during surgery the conjunctiva is carefully draped over the implant and closed meticulously to avoid postoperative wound leaks. The implant should be placed at a slightly posterior position such that it does not impinge on the suture line at the limbus. One eye in group 1 and 2 eyes in group 2 developed Tenon cysts, all of them presenting within 4 weeks of surgery. These were managed with needling with 5 mg 5-FU injection. It is important to emphasize that needling in cases with an Ologen implant differs from routine trabeculectomy cases as the needle has to be passed through the implant itself to create multiple porous channels and enhance the flow of the aqueous. One patient in group 1 had a flat avascular bleb and had to undergo a re-trabeculectomy with 0.2mg/ml MMC at the end of 3 months of follow up.Rosentreter et alreported early hypotony (<7 days) in the Ologen group.[17]Papaconstatinouet al documented among the complications, a case of endophthalmitis in one patient and bleb leaks in two patients who had undergone trabeculectomy with Ologen.[19] Senthil et al noted hyphaema as an early post-operative complication occurring more in the group with the Ologen implant. [20]This they attributed to the loose apical scleral suture which would be more likely to allow any ooze from the cut ends of the sclera to seep into the AC. However, no such complications were noted in our study. No Ologen specific side-effects like translocation of implant, erosion of conjunctiva or allergy was detected. The absence of complications like bleb leak, hypotony, blebitis in our study as compared to other studies can be attributed to the lower dose and duration of MMC applied.
The blebs in both the groups were similar in morphology when graded according to the standard set of pictures provided by IBAGS. Majority of the blebs were moderately elevated, mildly vascular and extending over 2-4 clock hours. More number of blebs in the Ologen + MMC group showed moderate to extensive vascularity (V3, V4) but the numbers were not statistically significant. The patient in Group 1 who had to undergo a second surgery with 0.2mg/ml MMC had a flat avascular bleb with no identifiable fluid cavity on ASOCT. At 6 months follow up, 76% of the blebs in group 1 and 79.17% of the blebs in group 2 were noted to have cystic elements on slit lamp examination.
The AS-OCT analysis of the internal structure of bleb revealed that the Ologen group had greater bleb height and internal fluid cavity as compared to the MMC group till 3 months of follow up. At 6 months, there was no significant difference in these parameters between the two groups. This can be attributed to the presence of Ologen as a spacer, which degrades within 6 months. The bleb wall thickness and radial width of the bleb were similar in both the groups. In this study, we also documented the number of microcystic spaces, defined ashyporeflective space >10µ, in the bleb wall. At 1 month and 3 months, the blebs with only MMC had more number of microcystic spaces ranging from 0-8 as compared to the combined Ologen and MMC group (range 1-3) (p= 0.004 at 1 month and 0.026 at 3 months). The difference ceased to be significant at 6 months (p=0.099) but the range of number of cystic spaces in group 1 (0-8) was still more as compared to group 2 (1-4).This finding is in agreement with the clinical assessment of bleb morphology by the IBAGS criteria which also showed no statistically significant difference between the blebs of the two groups.
In conclusion, the addition of a biodegradable collagen implant (Ologen) to trabeculectomy with Mitomycin C does not offer any significant advantage over conventional trabeculectomy with Mitomycin C alone in patients with moderate to advanced glaucoma. The added cost of the implant also does not make the combination feasible in a developing country for patients with primary glaucoma. A longer duration of study is necessary to evaluate the success of the blebs and ability to control intraocular pressure.
REFERENCES
- Foster PJ, Buhrmann R, Quigley HA, Johnson GJ. The definition and classification of glaucoma in prevalence surveys. British journal of ophthalmology. 2002 Feb 1;86(2):238-42.
- Kingman S. Glaucoma is second leading cause of blindness globally. Bulletin of the World Health Organization. 2004 Nov;82(11):887-8.
- Resnikoff S, Pascolini D, Etya’Ale D, Kocur I, Pararajasegaram R, Pokharel GP, Mariotti SP. Global data on visual impairment in the year 2002. Bulletin of the world health organization. 2004 Nov;82(11):844-51.
- Sihota R, Angmo D, Chandra A, Gupta V, Sharma A, Pandey RM. Evaluating the long-term efficacy of short-duration 0.1 mg/ml and 0.2 mg/ml MMC in primary trabeculectomy for primary adult glaucoma. Graefe’s Archive for Clinical and Experimental Ophthalmology. 2015 Jul 1;253(7):1153-9.
- Chen CW. Enhanced intraocular pressure controlling effectiveness of trabeculectomy by local application of mitomycin-C. Trans Asia Pac AcadOphthalmol. 1983;9:172-177.
- Azuara-Blanco A, Katz LJ. Dysfunctional filtering blebs. Survey of ophthalmology. 1998 Oct 31;43(2):93-126.
- Singh, K., Mehta, K., Shaikh, N.M., Tsai, J.C., Moster, M.R., Budenz, D.L., Greenfield, D.S., Chen, P.P., Cohen, J.S., Baerveldt, G.S. and Shaikh, S., 2000. Trabeculectomy with intraoperative mitomycin C versus 5-fluorouracil: prospective randomized clinical trial.Ophthalmology, 107(12), pp.2305-2309.
- Skuta GL, Beeson CC, Higginbotham EJ, Lichter PR, Musch DC, Bergstrom TJ, Klein TB, Falck FY. Intraoperative mitomycin versus postoperative 5-fluorouracil in high-risk glaucoma filtering surgery. Ophthalmology. 1992 Mar 1;99(3):438-44.
- WuDunn D, Cantor LB, Palanca-Capistrano AM, Hoop J, Alvi NP, Finley C, Lakhani V, Burnstein A, Knotts SL. A prospective randomized trial comparing intraoperative 5-fluorouracil vs mitomycin C in primary trabeculectomy. American journal of ophthalmology. 2002 Oct 31;134(4):521-8.
- Yannas IV, Burke JF, Orgill DP, Skrabut EM. Wound tissue can utilize a polymeric template to synthesize a functional extension of skin. Science. 1982 Jan 8;215(4529):174-6.
- Hsu WC, Spilker MH, Yannas IV, Rubin PA. Inhibition of conjunctival scarring and contraction by a porous collagen-glycosaminoglycan implant. Investigative ophthalmology & visual science. 2000 Aug 1;41(9):2404-11.
- Agis Investigators. The Advanced Glaucoma Intervention Study (AGIS): 7. The relationship between control of intraocular pressure and visual field deterioration. The AGIS Investigators. Am J Ophthalmol. 2000;130:429-40.
- Bengtsson B, Leske MC, Hyman L, Heijl A, Early Manifest Glaucoma Trial Group. Fluctuation of intraocular pressure and glaucoma progression in the early manifest glaucoma trial. Ophthalmology. 2007 Feb 28;114(2):205-9.
- Gordon MO, Beiser JA, Brandt JD, Heuer DK, Higginbotham EJ, Johnson CA, Keltner JL, Miller JP, Parrish RK, Wilson MR, Kass MA. The ocular hypertension treatment study. Arch Ophthalmol. 2002 Jun;120(6):714-20.
- Wilkins M, Indar A, Wormald R. Intra-operative mitomycin C for glaucoma surgery. Cochrane Database Syst Rev. 2001;1.
- Aptel F, Dumas S, Denis P. Ultrasound biomicroscopy and optical coherence tomography imaging of filtering blebs after deep sclerectomy with new collagen implant. Eur J Ophthalmol. 2009 Mar;19(2):223-30.
- Rosentreter A, Schild AM, Jordan JF, Krieglstein GK, Dietlein TS. A prospective randomised trial of trabeculectomy using mitomycin C vs an ologen implant in open angle glaucoma. Eye. 2010 Sep 1;24(9):1449-57.
- Cillino S, Casuccio A, Di Pace F, Cagini C, Ferraro LL, Cillino G. Biodegradable collagen matrix implant versus mitomycin-C in trabeculectomy: five-year follow-up. BMC Ophthalmology. 2016 Mar 5;16(24).
- Papaconstantinou D, Georgalas I, Karmiris E, Diagourtas A, Koutsandrea C, Ladas I, Apostolopoulos M, Georgopoulos G. Trabeculectomy with OloGen versus trabeculectomy for the treatment of glaucoma: a pilot study. Actaophthalmologica. 2010 Feb 1;88(1):80-5.
- Senthil S, Rao HL, Babu JG, Mandal AK, Garudadri CS. Comparison of outcomes of trabeculectomy with mitomycin C vs. ologen implant in primary glaucoma. Indian journal of ophthalmology. 2013 Jul;61(7):338.
Table 1. Comparison of demographic and the preoperative clinical features between the two groups.
| GROUP 1 (n=25) | GROUP 2 (n=25) | P VALUE | |
| AGE* | 55.96±8.46 | 60.12±7.46 | 0.072 |
| SEX (M:F) | 12:13 | 16:9 | 0.245 |
| BCVA (LogMAR)* | 0.99± 1 | 0.64± 0.54 | 0.54 |
| HVF (MD)(dB)* | -19.55±9.17 | -23.67±8.45 | 0.33 |
| TOPICAL ANTI-GLAUCOMA MEDICATIONS* | 3.64 ±0.67 | 3.2 ±0.92 | 0.59 |
| DIAGNOSIS (POAG:PACG) | 12:13 | 12:13 | |
| HIGHEST IOP (MMHg)* | 35.44±13.73 | 33.8±14.01 | 0.72 |
IOP: intraocular pressure, MAR: minimum angle of resolution, MD: Mean seviation, dB: Decibel, POAG: Primary Open- Angle Glaucoma, PACG: Primary Angle-Closure Glaucoma, *values in mean ± standard deviation.
Table 2: Comparison of Postoperative IOP readings between group 1 and group 2
| IOP (mean±SD) (mmHg) | BASELINE | DAY 1 | DAY 7 | 1 MONTH | 3 MONTHS | 6 MONTHS |
| GROUP 1 | 35.44±13.73 | 8.8±3.41 | 9.04±3.06 | 13.2±8.72 | 12±6.60 | 11±4.53 |
| GROUP 2 | 33.8±14.01 | 8.88±4.4 | 10±4.51 | 12.4±6.24 | 12.24±3.43 | 13.68±4.78 |
| P value | 0.72 | 0.82 | 0.54 | 0.82 | 0.22 | 0.07 |
IOP: Intraocular pressure

Fig 1: 6 months postoperative slit-lamp photograph showing a bleb after trabeculectomy with low dose MMC
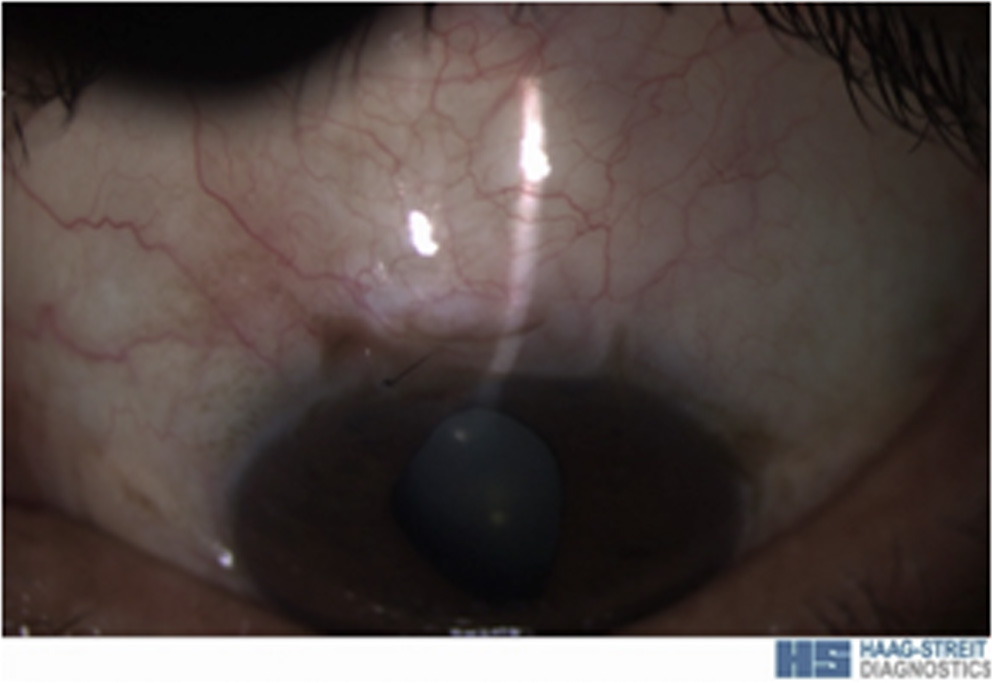
Fig 2: 6 months postoperative slit-lamp photograph showing a bleb after trabeculectomy with Ologen and low dose MMC
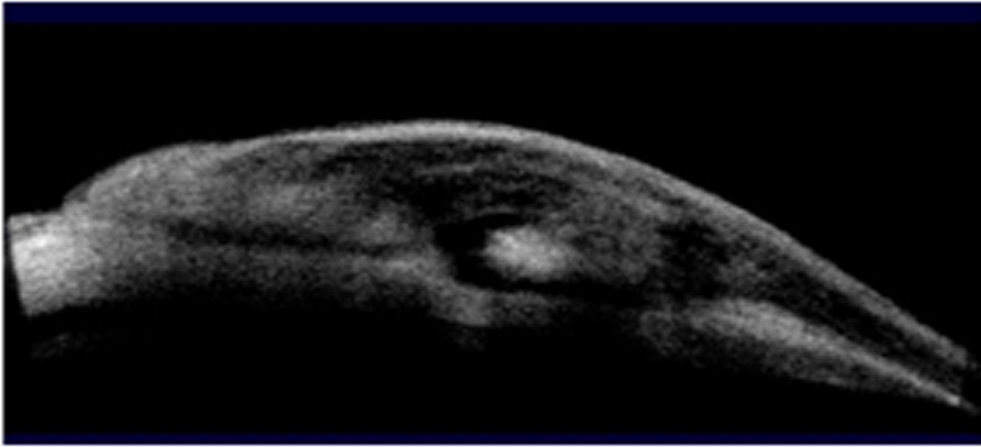
Fig 3: 3 months postoperative period. A well- functioning bleb in the MMC group showing hyporeflective spaces in the bleb was and the scleral flap.
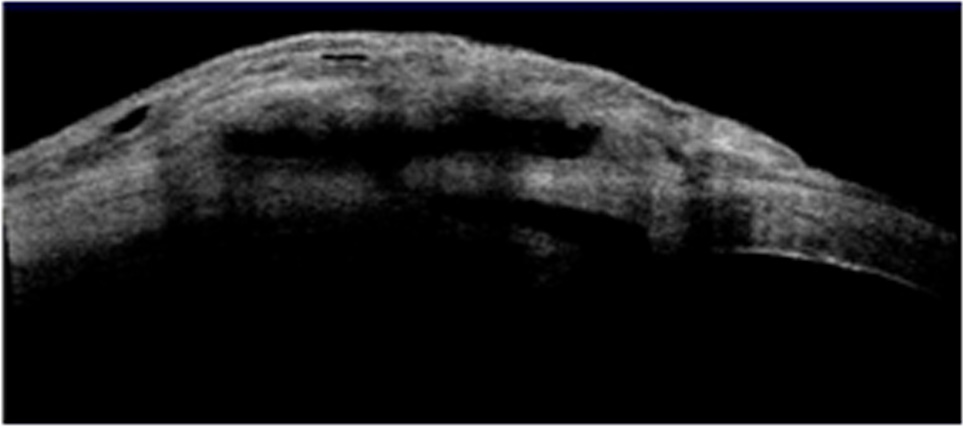
Fig 4: 3 months postoperative period. The bleb with Ologen shows a bleb with patent ostium and microcysts in the bleb wall
Leave a Comment