
Dr. Vanita Pathak Ray, V15422,Dr. Nikhil Choudhari, Dr. Siddharth Dikshit
Authors:
Vanita Pathak-Ray FRCS (Ed), FRCOphth (Lon)1, Swathi Vallabh Badakare MS2, Nikhil Choudhari DNB2,
1Centre for Sight, Road No 2 Banjara Hills, Hyderabad, India 500034
2VST Centre for Glaucoma, L V Prasad Eye Institute, L V Prasad Marg, Hyderabad, India 500034
Short Title: Phaco-ECPLvs Phaco-Trab in angle closure disease
Presented at:
- 7th World Glaucoma Conference, Helsinki, Finland, June-July 2017
- 27th Annual meeting of Glaucoma Society of India, Jaipur, India, September 2017
Phaco-Endocycloplasty vs Phaco-Trabeculectomy in PACG: Results of a Pilot Study
Abstract:
Aim: To investigate efficacy and safety of endocycloplasty (ECPL) vs trabeculectomy (trab), when it is combined with phaco in medically controlled or uncontrolled Primary Angle Closure or Glaucoma (PAC/G), post laser peripheral Iridotomy(LPI).
Methods: Prospective, interventional RCT where subjects above 30 years, with PAC/G and cataract underwent computer generated randomized sequence of either procedure (Phaco-ECPL or Phaco-Trab) for standard indications of combined surgery.
Primary outcome measure was IOP. Secondary: best corrected visual acuity (BCVA), number of AGM, complications and failure.
Result: A total of 42 eyes of 37subjects were included. 22 eyes underwent Phaco-ECPL and 20 eyes underwent Phaco-Trab. Median follow up in each group was 6 months. Median pre-op and post-op IOP, AGM and BCVA did not differ between the groups. However, rate of complications, and interventions, was greater in Phaco-Trab group.
Conclusion: Both procedures are efficacious in lowering IOP in PACG, but rate of complication is more in Phaco-Trab group; further follow-up is required to assess whether this is sustained over longer term.
Introduction:
Trabeculectomy, since its description in the late 1960’s, has been the mainstay of surgical treatment in both open as well as closed angle glaucoma.(1)The guarded filtration technique, as described by Cairns, was an improvement on the full thickness filtration procedure, with unquestionable efficacy specially when adjuvant anti-fibrotics are used. However, it continues to be plagued by unique sight-threatening complications, including and not limited to hypotony and its sequelae and life-long risk of leak and infection. Perhaps this risk of morbidity was the prime determinant of its use mostly in medically resistant, usually advanced glaucoma. Furthermore, morbidity due to angle closure disease is known to be higher and in a developing country like ours, as access to healthcare is not only poor, but also delayed, it increases several-fold.
Surgical management in open angle disease has made progress in recent times; these newer devices and procedures, the so called minimally invasive glaucoma surgery (MIGS) – unlike their predecessors, are bleb-independent and hence have a better safety profile.(2)However IOP reduction is modest at best, and they are thus indicated in early-to moderate open angle disease; these devices do not have relevance in angle closure, unless the angle opens post laser peripheral iridotomy (LPI).(3) A literature search yields approximately 25-59% (4-6) angles that continue to remain occludable post LPI. Thus, there is unmet need in angle closure disease.
Recent evidence from The EAGLE study(7) suggests that lens extraction (clear) alone may be sufficient for control of angle closure disease. However, angle closure exists in various forms and phacoemulsification alone does not seem to resolve the pure plateau mechanism (Figure 1) of angle closuredue to high ciliary body insertion(Plateau Iris Syndrome, PIS).(8)
Endocyclophotocoagulation (ECP) is one such minimally invasive procedure that may be deployed in PIS and angle closure as angle status is inconsequential in the delivery of laser. It has been used with moderate success in open angle, paediatric and refractory glaucomas. (9-12) In a modification of ECP, endocycloplasty (ECPL) has recently been described (13, 14) and combined with Phacoemulsification, itis gathering momentumin PIS.(15)We too conducted a pilot study of 10 eyes of 9 patients who were treated with combined phacoemulsification and ECPL for angle closure disease and did not restrict the procedure to PIS alone. We have a median follow-up of 18 months; median IOP significantly decreased from 20 to 15.5 mm Hg, and the median number of glaucoma medications significantly decreased from 3 to 0 and decimal VA significantly improved from 0.55 to 1. Importantly, no serious sight threatening side-effects were seen in the post-operative period. Table 1.
We thus set out to investigate the efficacy and safety of endocycloplasty compared with the current gold-standard, trabeculectomy, when these are combined with phacoemulsification in medically controlled and uncontrolled Primary Angle Closure/Glaucoma, (PAC/G) post LPI.
Methods:
Study design: Prospective, comparative, interventional
Informed consent was obtained from all participants for the surgical procedure and the study was approved by the ethics committee and review board (IRB).It was conducted in accordance with the tenets of the Declaration of Helsinki. It was also registered with Clinical Trials Registry – India (CTRI).
PAC/G subjects above 30 years and cataract underwent computer generated randomized sequence of either procedure (Phaco-ECPL or Phaco-Trab) for standard indications of combined surgery. These included uncontrolled intraocular pressure (IOP), controlled IOP on maximally tolerated medication and visual field defects involving or very close to fixation. Patients unable to afford anti-glaucoma medications (AGM) as well as those that were poorly adherent to it were also considered.
Inclusion criteria
Lens status – presence of visually significant cataract (20/40 or less) or glaucomflecken and
Primary Angle Closure disease (PAC and PACG) subjects post LPI with standard indications for combined surgery
IOP uncontrolled or
IOP controlled on 3 or more anti-glaucoma medications and / or 10-2 HVF shows involvement of fixation or
Intolerant to or unable to afford anti-glaucoma medication
Exclusion criteria
Age <30 years
Unwillingness or inability to participate
Any ocular surface infection
Any previous incisional surgery
Any cause for secondary glaucoma
One-eyed subject
Depression of any paracentral point on 10-2 of Humphrey Visual Field to 0 dB
Primary outcome measure was IOP with complete success being defined as an IOP > 5 and ≤18 mmHg without medication; if the preoperative IOP was ≤21 mmHg, an IOP reduction of > 20% without medication, was also considered as success. Qualified success was defined as meeting these criteria with medication. Failure to meet these criteria and/or requirement for revision procedures (in phaco-trab group needling permissible within 3 months of surgery) and or reoperation (trabeculectomy or glaucoma drainage device or transcleral-cyclophotocoagulation) was defined as failure of the procedure.
Secondary outcome measures were best corrected LogMAR visual acuity (BCVA), number of AGM, complications and failure (defined as need for second surgery to control IOP).
Surgical technique of Phaco-ECPL:
Procedure was done under regional anaesthesia (peribulbar anaesthesia Bupivacaine 0.5% + Xylocaine 2%, Astra Zeneca)
It involved Phacoemulsification and IOL surgery, performed prior to endocycloplasty (ECPL).
We prefer a clear corneal incision for ease of access and its self-sealing properties. The same incision is typically used for both phacoemulsification and ECPL.
After phaco is completed and the PCIOL is in the bag, the AC is filled with a cohesive visco-surgical device and the endoscope is introduced into the anterior chamber (AC) to visualise the angle. Figure 2A.
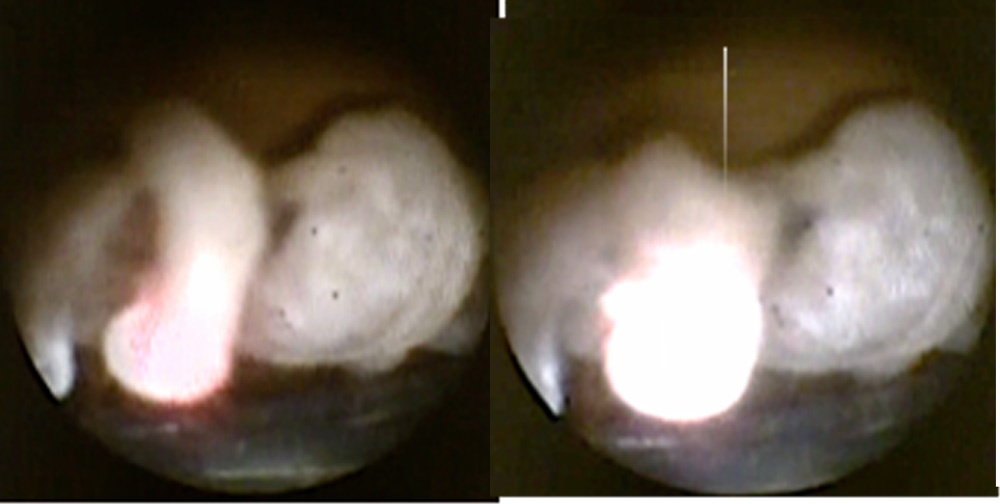
Following this, we injected cohesive ophthalmic visco-surgical device to expand the ciliary sulcus and create space for the endoscopic probe. The 20-gauge curved ECP probe (Endo Optiks, Little Silver, NJ), which consists of a fibre-optic camera and a diode laser is placed through the main incision. We set the laser to continuous-delivery mode with 250 to 500 mW of power. We visualized the ciliary processes by passing the curved probe behind the iris and into the sulcus. A red aiming beam is aligned with the posterior aspect of the ciliary processes. It is important to start lasering at the posterior tail aspect of the ciliary processes and to observe the processes retreat posteriorlyFigure 3. The goal of laser is shrinkage and not destruction so the endpoint of laser treatment is marked by adequate shrinkage and whitening of the ciliary process, strictly avoiding “pops”. The latter occur due to application of too much energy; moreover, overtreatment may lead to excessive postoperative inflammation and a breakdown of the blood-aqueous barrier and its sequelae.
The endoscope is re-introduced into the AC, to visualise the angle yet again. In this case, in stark contrast to the view after phaco alone (figure 2A), immediately prior to endocycloplasty, appositionally closed angle opens up to scleral spur in the inferior 180 degrees. Figure 2B.
At the end of the procedure, viscoelastic was washed and sub-conjunctival steroid administered (Dexamethasone 2mg).
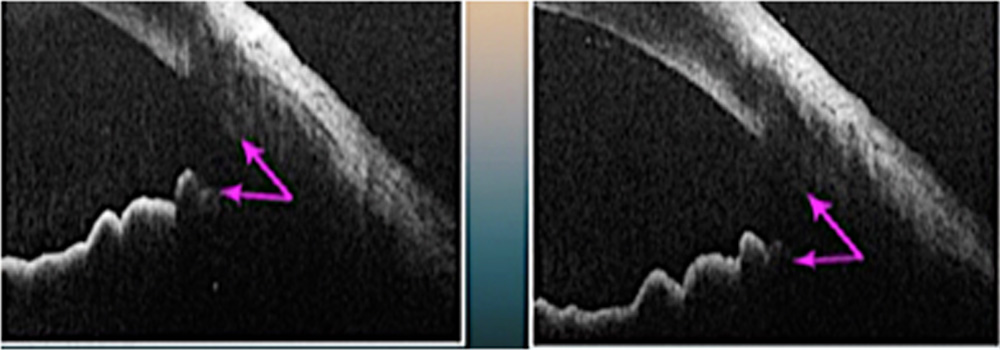
We have performed intra-operative anterior segment OCT to demonstrate change in angle recess, when synaechial angle closure is absent. Images were obtained after phaco (and before ECPL) and again after ECPL.Figure 4.
Phaco-Trab:
Procedure was done under regional anaesthesia (peribulbar anaesthesia Bupivacaine 0.5% + Xylocaine 2%, Astra Zeneca)
Phaco and trabeculectomy were done through separate sites – both incisions were superior.
Trabeculectomy – conjunctival incision was supero-nasal in the right eye and supero-temporal in the left eye. Sponge application of Mitomycin C (MMC Inj, Biochem) 0.4 mg/ml was used for 2 minutes after rectangular scleral flap was raised.
Phaco was undertaken through a clear corneal supero-temporal wound in the right eye or a supero-nasal one in the left eye. Post PCIOL insertion, clear-corneal wound was sutured with 10/0 nylon.
Trabeculectomy was completed by creating an ostium with a Descemet’s punch and peripheral Iridectomy with Vannas scissors. Scleral flap is sutured with 2 10/0 nylon sutures; conjunctiva was closed with 10/0 vicryl running mattress sutures.
At the end of the procedure, viscoelastic was washed and sub-conjunctival steroid administered (Dexamethasone 2mg)
Post-operatively all subjects were administered topical Prednisolone Acetate 1% (Predforte, Allergan, Irvine, CA, USA) for 6-8 weeks (in tapering dose), Moxifloxacin Hydrochloride 0.5% (Vigamox, Alcon, Fort Worth, TX, USA) four times daily for one week and cycloplegic eyedrops (Homatropine Hydrochloride 2%, Homide, Warren Excel) thrice daily for 1-2 weeks.
Results:
We recruited 42 eyes of 37 patients in this pilot study; 22 subjects were females. 22 eyes underwent phaco-ECPL; 2 were excluded as laser parameters were not as per protocol. 20 eyes were recruited in the phaco-trab group. Mean f/u in the phaco-trab group was11.5 ± 5.2 months and that in the phaco-ECPL group was 8.0 ± 4.9 months. Both groups were very well matched pre-operatively and no difference was seen between the groups, notably in IOP, number of AGM, pre-operative visual acuity and angle status. Table 2.
At last follow-up, there was no difference in IOP, anti-glaucoma medication and vision in either groupTable 3; however, the phaco-ECPL group not only had a much lesser number of complicationsbut also lower rate of interventions for these complication, both of which were statistically significant (p=0.02 and 0.03 respectively, chi square test)Table 4.
Complete success, as per our criteria, was 75% in phaco-ECPL group and 65% in phaco-trab group; total success was 95% in the former and 90% in the latter(p=0.74). There was 1 failure in the phaco-ECPL group on IOP criterion alone; phaco-trab group had 2 failures.1 eye required a major bleb revision at 7 weeks post phaco-trab whilst the other eye required a needling at 12 months.
Both groups had per-operative complications – I eye in phaco-ECPL group had zonular dehiscence of <3 clock-hours and an endo capsular ring was used. Both eyes of one patient in the phaco-trab group developed aqueous misdirection per-operatively for which Irido-Zonulo-Hyaloido-Vitrectomy (IZHV) was performed via the ostium created as part of trabeculectomy.
Post-operatively both groups had few eyes with fibrinous uveitis; 6 eyes in phaco-ECPL group and 2 in phaco-trab group. Phaco-ECPL group had no further complications but phaco-trab group had several bleb-related complications. Table 4.
One further eye in the latter group had aqueous misdirection post-operatively and required Yag laser hyaloidotomy. This eye also eventually failed.
Discussion:
Cataract (or clear lens) extraction (7, 16)alone is said to be successful in acute angle closure; however, it is known that lens extraction alone does not modify angle morphology in PIS(8). Furthermore, it may not be sufficient in controlling IOP when synaechial angle closure exists simultaneously(17).
We conducted this randomised trial of phaco-ECPL with phaco-trab in angle closure disease only after the results of a previous pilot study of10 eyes of 9 patients who were treated with combined phacoemulsification and ECPL for angle closure disease, in all standard indications of combined phaco-filtration surgery, appeared very encouraging. This study also revealed phaco-ECPL to be a very efficacious procedure in the reduction of IOP, just as phaco-trab is in angle closure disease. Phaco-ECPL has recently gained a fair amount of terrain in the surgical management of PIS (15, 18, 19)but unlike all these authors, wedid not restrict the procedure to PIS alone; instead we extended it to relative pupillary block, and eyes that had synaechial angle closure too.
Similar to IOP control, no difference was seen between groups in terms of number of AGM required and BCVA. Complete success, as per our criteria, was also virtually identical in both groups (p=0.74). However, what separated the two was the number of complications and the rate of intervention for these complications, both of which were statistically significant.
Both groups had per-operative complications– 1 eye in phaco-ECPL group had mild zonular dehiscence of <3 clock-hours without vitreous loss, which under usual circumstances would have been managed conservatively; however, as there is a minor concern about zonular damage during endocyclophotocoagulation, we preferred to use an endo-capsular ring per-operatively. This eye did not demonstrate any subluxation or dislocation of PCIOL in the post-operative period.
Perhaps as anticipated, and in contrast to the phaco-trab group, phaco-ECPL group had fibrinous uveitis (n=6, 30%) as the commonest post-operative complication, even though we made all efforts to avoid ‘pops’ during deliver of laser, a condition whereby breakdown of blood-aqueous barrier occurs with excessive inflammation.In two eyes, it also resulted in closure of peripheral iridotomy, with secondary pupillary block, so LPI was repeated. We did not encounter any case of hypotony or lost vision due to ECPL; treatment of less than three quadrants of ciliary body made hypotony a remote possibility. The ECP collaborative study group(in 5824 eyes), have reported very low rates of hypotony (0.12%) and choroidal haemorrhage(20)(0.09%).(21)
Other serious vision threatening complications, like choroidal detachment, hypotony or aqueous misdirection (AM) also did not occur in the phaco-ECPL group.
In contrast, in the phaco-trab group AM occurred in 3 eyes; 2 eyes of the same patient per-operatively and 1 eye post-operatively. AM is known to occur with greater frequency in filtration surgery for angle closure disease post-operatively (20), but per-operative AM can occur and is recognised by a non-deepening anterior chamber (AC), even after cataract extraction and intense cycloplegic application. Both these eyes with AM were managed successfully with IZHV via pre-existing ostium and iridectomy, to render the eye unicameral. Following the occurrence of AM in one eye, alertness during surgery for its occurrence in the fellow second eye was high, as this has been reported in literature. (22, 23)IZHV has been described for management of pseudophakic AM (24, 25)but its prompt usage per-operatively averted any further intervention for this dreaded complication and resulted in complete resolution of AM and the AC remained deep throughout follow-up period with good recovery of vision. One further eye,which developed AM post-operatively, received Yag laser hyaloidotomy, which temporised the condition. However, this eye eventually failed with an engorged bleb and required major bleb revision with reformation of AC; it also happened to be the only eye on 4 AGM at last follow-up for control of IOP.
The phaco-trab group had other bleb-related complications including leak (n=4, 20%) and has been reported as 14% and 17.6% in two large studies of trabeculectomy respectively (26, 27). It is possible that all 4 eyes recognised with suture-track leak per-operatively may not have had any on day 1 post-operative after the routine overnight pressure patching. Nonetheless, they all received a bandage contact lens (BCL) per-operatively for fear of triggering a shallow anterior chamber, and sequelae, in this very high-risk group (for AM). BCL was left in situ for at least 1 week; only one eye showed overt leak after this period and BCL was replaced for another week. None of the leaks required resuturing.
There was 1 failure in the phaco-ECPL group on IOP criterion alone; as it was borderline it was being observed. However, patient was lost to follow-up before AGM need for AGM could be ascertained. Phaco-trab group had 2 failures; 1 eye required a major bleb revision at 7 weeks post phaco-trab whilst the other eye required a needling at 12 months. As per protocol, needling was permissible only in the second and third months post-surgery and an intervention after this was considered a failure of the procedure.
Our pilot study has successfully demonstrated the ability of ECPL in not only controlling IOP in angle closure disease, when combined with phaco surgery, but being as efficacious as phaco-trab. The mechanism of action of ECPL appears to be two-pronged; firstly, it modifies angle anatomy by widening the angle recess (especially when synaechial angle closure does not exist) and secondly, the photocoagulation effect of the laser helps in IOP control. It need not be restricted to PIS; it appears to effective in synaechial angle closure as well. Studies hitherto have mainly concentrated in open angle or refractory glaucomas.
Thus, in a head-to-head comparison with phaco-trabeculectomy, currently the gold standard procedure, phaco-ECPL is quicker surgery, with faster recovery, and appears to be equally efficacious without the incumbent serious complications related to trabeculectomy in angle closure disease.
Furthermore, it can be repeated if required and if it is still not effective, it does not preclude, or compromise, future trabeculectomy as conjunctiva is unscathed. It can be easily combined with cataract surgery by anterior segment surgeons and usually adds no more than 5-10 minutes to a phaco procedure.
Moreover, on an average, we used only one-fourth the total energy, or less, when compared to trans-scleral cyclophotocoagulation. Hence direct visualisation of ciliary processes for precise delivery of reduced laser energy helped to avoid pain, excessive inflammation, hypotony, phthisis and visual loss associated with trans-scleral delivery of the same(28)where absorption across sclera is erratic and unpredictable, at best of times.
This technology is readily available but expense may be a consideration, especially in a developing country like ours. However, it should be considered as a one-time capital expenditure, just like a phaco machine. The possibility of acquiring an endoscope alone and coupling it with a pre-existing diode laser machine, if available, can also be contemplated, driving down expenditure.
Cost notwithstanding, when seen from the perspective of the patient, this freely-available, relatively new technology not only improves their quality of life, with none or fewer anti-glaucoma medications, but also faster visual rehabilitation, lesser number of complications and interventions for the same, with fewer post-operative visits.The benefit of any glaucoma procedure reducing intraocular pressure needs to be weighed against its adverse events. Creation of a bleb in trabeculectomy, efficacious though it may be, is the source of most serious sight threatening complications.
To conclude, removal of the lens is advocated early in angle closure disease and when it is combined with ECPL, it has the ability of controlling IOP, with minimal side-effects. Further follow-up is required to assess whether this is sustained over longer term.
References:
- Cairns JE. Trabeculectomy. Preliminary report of a new method. American journal of ophthalmology. 1968;66(4):673-9.
- Saheb H, Ahmed, II. Micro-invasive glaucoma surgery: current perspectives and future directions. Curr Opin Ophthalmol. 2012;23(2):96-104.
- Pathak-Ray V. Advances in glaucoma surgery: Paradigm shift in management2016 Oman J Ophthalmol. 2016. 9(1): 1-2.
- Kumar RS, Tantisevi V, Wong MH, Laohapojanart K, Chansanti O, Quek DT, et al. Plateau iris in Asian subjects with primary angle closure glaucoma. Archives of ophthalmology. 2009;127(10):1269-72.
- Thomas R, Arun T, Muliyil J, George R. Outcome of laser peripheral iridotomy in chronic primary angle closure glaucoma. Ophthalmic Surg Lasers. 1999;30(7):547-53.
- He M, Friedman DS, Ge J, Huang W, Jin C, Cai X, et al. Laser peripheral iridotomy in eyes with narrow drainage angles: ultrasound biomicroscopy outcomes. The Liwan Eye Study. Ophthalmology. 2007;114(8):1513-9.
- Azuara-Blanco A, Burr J, Ramsay C, Cooper D, Foster PJ, Friedman DS, et al. Effectiveness of early lens extraction for the treatment of primary angle-closure glaucoma (EAGLE): a randomised controlled trial. Lancet. 2016;388(10052):1389-97.
- Tran HV, Liebmann JM, Ritch R. Iridociliary apposition in plateau iris syndrome persists after cataract extraction. American journal of ophthalmology. 2003;135(1):40-3.
- M U. Combined phacoemulsification, endoscopic ciliary process photocoagulation, and intraocular lens implantaion in glaucoma management. Ophthalmic Surg. 1995;26:346-52.
- Kahook MY, Lathrop KL, Noecker RJ. One-site versus two-site endoscopic cyclophotocoagulation. Journal of glaucoma. 2007;16(6):527-30.
- Carter BC, Plager DA, Neely DE, Sprunger DT, Sondhi N, Roberts GJ. Endoscopic diode laser cyclophotocoagulation in the management of aphakic and pseudophakic glaucoma in children. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus / American Association for Pediatric Ophthalmology and Strabismus. 2007;11(1):34-40.
- Neely DE, Plager DA. Endocyclophotocoagulation for management of difficult pediatric glaucomas. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus / American Association for Pediatric Ophthalmology and Strabismus. 2001;5(4):221-9.
- Pathak-Ray VA, I.I.K. Phaco-endocycloplasty: A novel technique for management of ring iridociliary cyst presenting as acute angle closure.Oman J Ophthalmol. 2016. 9(1): 63–5
- JM G. Combined cataract and glaucoma surgery: Trabeculectomy vs endoscopic laser cycloablation. J Cat Refractive Surg. 1999;25:1214-9.
- Francis BA, Pouw A, Jenkins D, Babic K, Vakili G, Tan J, et al. Endoscopic Cycloplasty (ECPL) and Lens Extraction in the Treatment of Severe Plateau Iris Syndrome. Journal of glaucoma. 2015. doi: 10.1097/IJG.0000000000000156. PubMed PMID: 25794042.
- Jacobi PC, Dietlein TS, Luke C, Engels B, Krieglstein GK. Primary phacoemulsification and intraocular lens implantation for acute angle-closure glaucoma. Ophthalmology. 2002;109(9):1597-603.
- Zhuo YH, Wang M, Li Y, Hao YT, Lin MK, Fang M, et al. Phacoemulsification treatment of subjects with acute primary angle closure and chronic primary angle-closure glaucoma. Journal of glaucoma. 2009;18(9):646-51.
- Podbielski DW VD, Tam DY, et al. Endocycloplasty: a new technique for managing angle-closure glaucoma secondary to plateau iris syndrome. Glaucoma Today. 2010:29-31.
- Ahmed IK PD, Naqi A, et al. Endoscopiccycloplasty in angle closure glaucoma secondary to plateau iris. American Glaucoma Society Annual Meeting; March 5-8, 2009; San Diego, CA2009.
- Balekudaru S, Choudhari NS, Rewri P, George R, Bhende PS, Bhende M, et al. Surgical management of malignant glaucoma: a retrospective analysis of fifty eight eyes. Eye (Lond). 2017;31(6):947-55. Epub 2017/03/04.
- Noecker RJ. Complications of endoscopic cyclophotocoagulation: ECP Collaborative Study Group. Paper presented at: The ASCRS Symposium on Cataract, IOL and Refractive Surgery: May 1, 2007 San Diego CA2007.
- Saunders PP, Douglas GR, Feldman F, Stein RM. Bilateral malignant glaucoma. Can J Ophthalmol. 1992;27(1):19-21.
- Chaudhry NA, Flynn HW, Jr., Murray TG, Nicholson D, Palmberg PF. Pars plana vitrectomy during cataract surgery for prevention of aqueous misdirection in high-risk fellow eyes. Am J Ophthalmol. 2000;129(3):387-8.
- Lois N, Wong D, Groenewald C. New surgical approach in the management of pseudophakic malignant glaucoma. Ophthalmology. 2001;108(4):780-3.
- Madgula IM, Anand N. Long-term follow-up of zonulo-hyaloido-vitrectomy for pseudophakic malignant glaucoma. Indian J Ophthalmol. 2014;62(12):1115-20.
- Kirwan JF, Lockwood AJ, Shah P, Macleod A, Broadway DC, King AJ, et al. Trabeculectomy in the 21st century: a multicenter analysis. Ophthalmology. 2013;120(12):2532-9.
- Edmunds B, Thompson JR, Salmon JF, Wormald RP. The National Survey of Trabeculectomy. III. Early and late complications. Eye (Lond). 2002;16(3):297-303.
- Bloom PA, Tsai JC, Sharma K, Miller MH, Rice NS, Hitchings RA, et al. “Cyclodiode”. Trans-scleral diode laser cyclophotocoagulation in the treatment of advanced refractory glaucoma. Ophthalmology. 1997;104(9):1508-19.
Table 1. Results of a pilot study of phaco-endocycloplasty alone in angle closure disease
| Parameter | Pre Phaco-ECPL | Post Phaco-ECPL | p | |
| Median IOP mmHg
(Quartiles, IQR) |
20 (Q1 18, Q3 23.5, IQR 5.5) | 14(Q1 12, Q3 16, IQR 4) | <0.01 | |
| IOP (range) mmHg | 11-46 | 12-20 | ||
| Median AGM*
(Quartiles, IQR) |
3 (Q1 2, Q3 3.75, IQR 1.75) | 0 | <0.01 | |
| AGM (range) | 1-4 | |||
| Median logMAR BCVA**
(Quartiles, IQR) |
0.55 (Q1 0.425, Q3 0.825, IQR 0.4) | 0 (Q1 0, Q3 0.075, IQR=0.075) | <0.01 | |
| *AGM – anti glaucoma medication | ||||
| **BCVA – best corrected visual acuity | ||||
Table 2: Pre-operative characteristics of Phaco-endocycloplasty and Phaco-trabeculectomy groups
| Phaco-ECPL
n=20 |
Phaco-Trab
n=20 |
p value | ||
| Age, Median (IQR)
|
65 (12) | 59 (13) | 0.23 | |
| IOP, Median (IQR)
|
20 (15.5) | 17 (13) | 0.76 | |
| Uncontrolled IOP
n, % |
10, 50% | 10, 50% | 0.25 | |
| AGM, Median (IQR) | 3 (1) | 3 (2) | 0.93 | |
| LogMAR BCVA
Median (IQR) |
0.3 (0.25) | 0.4 (0.3) | 0.9 | |
| Post-LPI occludable; n, % | 10, 50% | 14, 70% | 0.28 | |
| Synaechial closure
Median (IQR) |
0 (1.5) | 0 (2) | 0.62 | |
| Lens rise
Median (IQR) |
690 (330) | 630 (340) | 0.5 | |
| VFI
Median (IQR) |
36 (47.5) | 66 (13.5) | 0.14 | |
Table 3. Post-operative results Phaco-endocycloplasty vs Phaco-trabeculectomy groups
| Phaco-ECPL
n=20 |
Phaco-Trab
n=20 |
p value | |
| IOP, Median (IQR)
|
15 (5.5) | 16 (6) | 0.8 |
| AGM, Median (IQR) | 0 | 0 | 0.9 |
| LogMAR BCVA, Median (IQR) | 0.1 (0.25) | 0.1 (0.25) | 0.7 |
Table 4. Post-operative complications in Phaco-endocycloplasty vs Phaco-trabeculectomy
| Complication | Phaco-Trab | Intervention | Phaco-ECPL | Intervention |
| Intra-op | Aqueous Misdirection (AM) n=2 | IZHV n=2 | Zonular Dehiscence n=1 | Endo-capsular
Ring n=1 |
| Post-op | Fibrinous uveitis n=2 | Yag to membrane n=1 | Fibrinous uveitis n=6 | Repeat LPI n=2 |
| Bleb Leak n=4 | Bandage contact lens n=4 | – | – | |
| Hyphaema n=1 | – | – | – | |
| Encysted bleb n=1 | – | – | – | |
| AM n=1 | Yag Hyaloidotomy n=1 | – | – | |
| Failure n=2 | Bleb revision n=1
Bleb needling n=1 |
– | – |
Fig 1. UBM: persistence of irido-ciliary apposition, before and after lensectomy in PIS (with kind permission from Dr. Iqbal Ike Ahmed, MD)
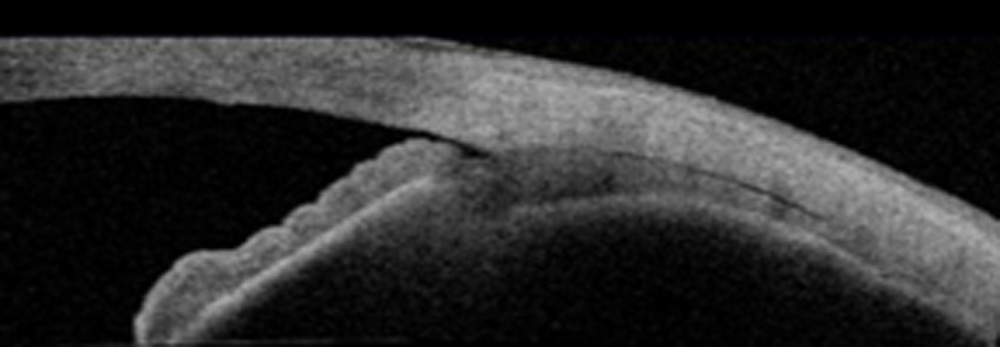
Figure 2A: Endoscopy pre-ECPL, post phaco – except for 1 clock hour (arrows), the rest of the angle in the inferior 180 degrees appears closed.
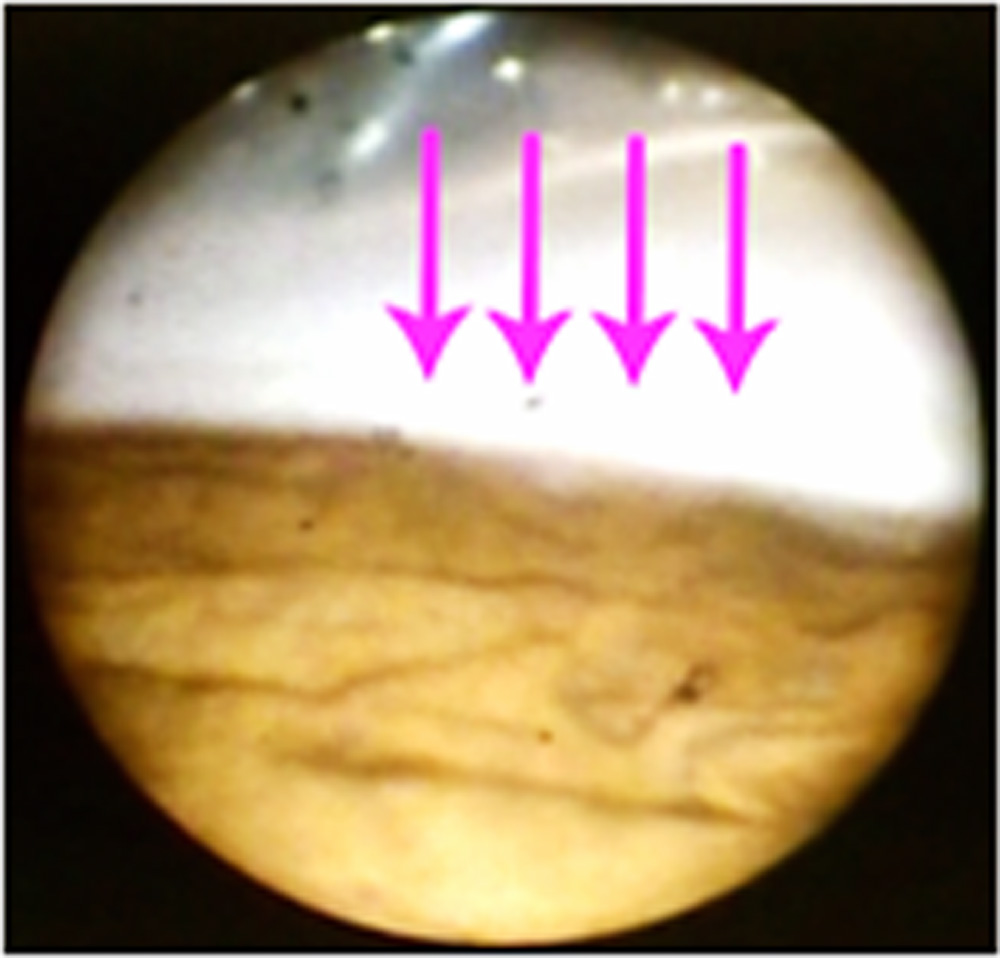
Figure 2B: Endoscopy post phaco-endocycloplasty – scleral spur is visible throughout inferior 180 degrees.
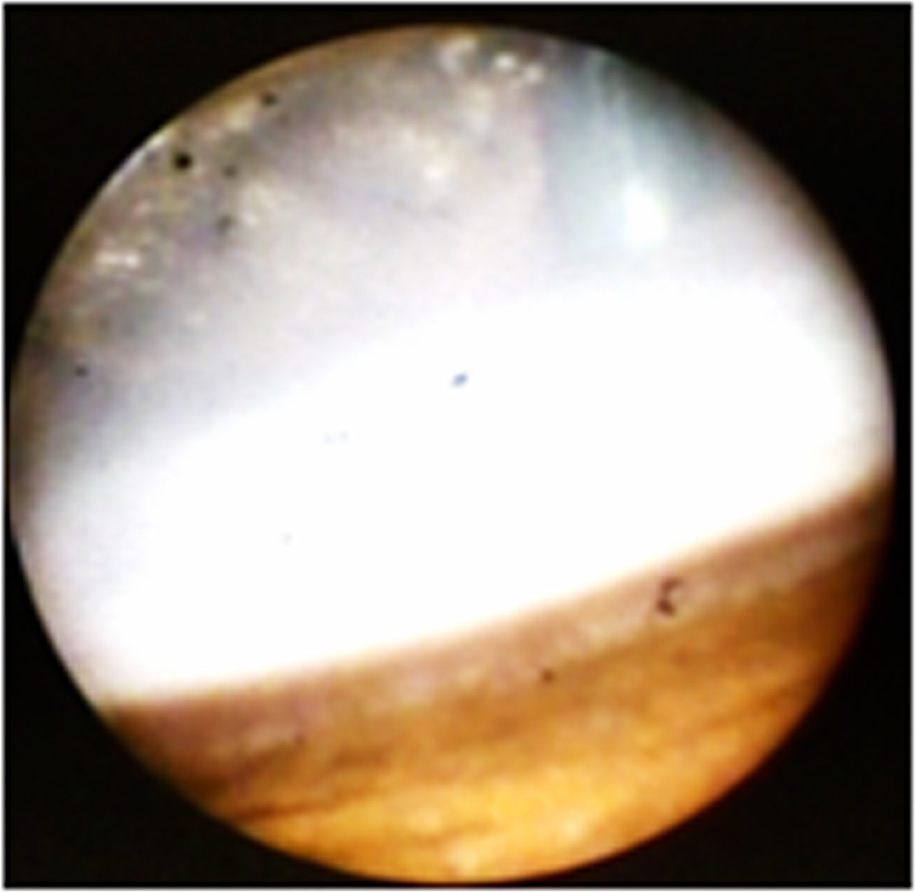
Figure 3: Left – laser is aimed at the tail of the ciliary process (red) and Right –whitens, contracts and retracts posteriorly post laser, as ascertained by its height in relation to the ciliary process adjacent to it
Figures 4: Intraoperative ASOCTLeft –angle recess before ECPL (after phaco) and Right – after phaco-ECPL
Leave a Comment