
Dr. Revathy Subramany, S14321
Objective: To study the correlation of Meibomian gland dysfunction (MGD) with anterior and posterior Blepharitis
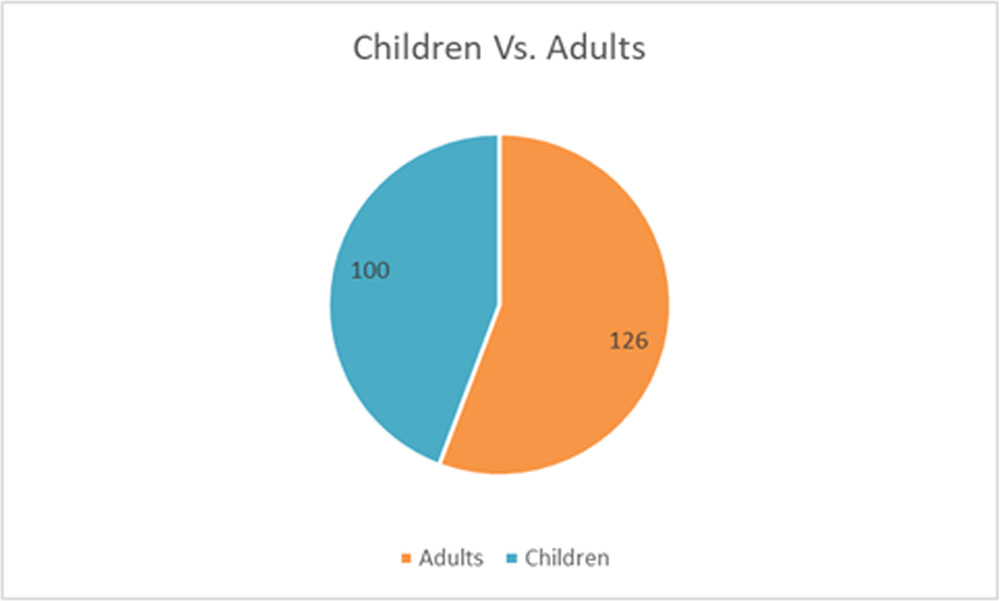
Method: A prospective study was performed on 226 patients with blepharitis from the age ranges of 10 to 73. One hundredpatients were in the age group of 10-18 (children) and 126were in the group of above 18yrs (Adults). Meibography and swab culture and sensitivity were done
Results:
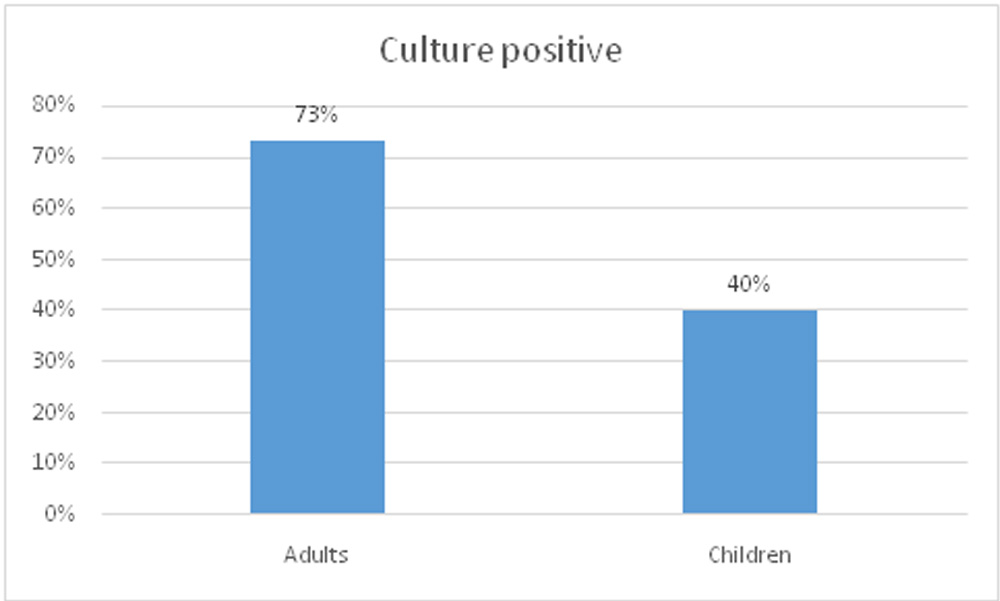
Male female ratio was 67:33 in adults and 68: 32 in children.MGD was observed in 90% of the adults while only 10% in children.Bacterial culture was positive in 73% of adults and 40% of children.Anterior Blepharitis was noted more in children (40%) whichwas associated with allergy. Posterior Blepharitis was more in adults (60%) and 90% of the adults showed MGD and was associated with Dry eye.
Conclusion:
MGD is more observed in adults. Posterior Blepharitis showed a significant correlation with MGD while anterior Blepharitis is correlated with allergy.
Introduction
Blepharitis a common disorder of the eye and is characterized by visible inflammation of the eyelids.It is associated with irritation, hyperemia, foreign body sensation, grittiness, photophobia, eyelid crusting, and swollen eyes. Although it does not cause permanent damage to vision, blepharitis has been implicated as a major contributor to the development of dry eye complaints1
The two primary distinctions in blepharitis are anterior versus posterior blepharitis. With anterior blepharitis, the inflammation is localized to the lid margin anterior to the gray line, with inflammation concentrated around the base of the lashes in the form of squamous debris (derived from squamous epithelial cells) or collarets, which may spill onto the posterior lid margin.1
Posterior Blepharitis occurs at the inner edges of the eyelids and involves the meibomian glands2 Meibomian gland dysfunction (MGD) is often used synonymously with posterior blepharitis1; MGD is a chronic, diffuse abnormality of the meibomian glands, commonly characterized by terminal duct obstruction and/or qualitative/quantitative changes in the glandular secretions. This may result in alterations of the tear film, symptoms of eye irritation, clinically apparent inflammation, and ocular surface disease.1MGD is one of the most common causes for the development of ocular surface disease symptoms, specifically those associated with dry eye conditions.
Studies have shown that in cases of chronic blepharitis (including both anterior and posterior), symptoms may occur due to MGD and its associated lipid anomalies, or by way of a direct effect of bacterial toxins in the aqueous layer and on the ocular surface and eyelid skin margin3-5. The purpose of current study was to assess the correlation of MGD with anterior and posterior Blepharitis.
Patients and Method
This was a prospective study included 226 patients with blepharitis. Patients’between10 to 73 years of age were recruited. A detailed history was elicited for symptoms of recurrent lid inflammation, Seborric dermatitis,keratitis and dandruff,. Based on their age,patients were divided into 2 groups, 100 patients were in the age group of 10-18 (children) and 126were in the group of above 18yrs (Adults). Patients who had any previous lid diseases were excluded from the study.Meibography and swab for bacterial culture and sensitivity were done on all patients.
Based on clinical features, slit lamp examination and Meibographyand culture and sensitivity result, patients were classified as Anterior Blepharitis group and posterior Blepharitis group. Clinical features of patients with Anterior Blepharitis included discomfort, mild photophobia, sticky lids, lid margin hyperemia and lid ulceration and the symptoms were more in the morning with series of remissions and exacerbations. While posterior blepharitis had mucous discharge and thick secretion in addition to lid margin hyperemia and discomfort. These patients had complaints of dry eye.
Slit lamp examination of anterior blepharitis patients revealed the evidence of lid margin hyperemia, edema, telengiectasis of anterior lid margin. Scaling and collarets were visible at the base of lash follicles. Poliosis, ulceration, madrosis and scarring were observed in few cases.
While in posterior blepharitis patients slit lamp examination showed the lid margin crusting behind the grey line extended to the base of lashes. Signs of dry eye with tearfilm debris and saponification of tearfilm with low meniscus height also observed. Peripheral corneal vascularization and marginal keratitis was evident in few cases.
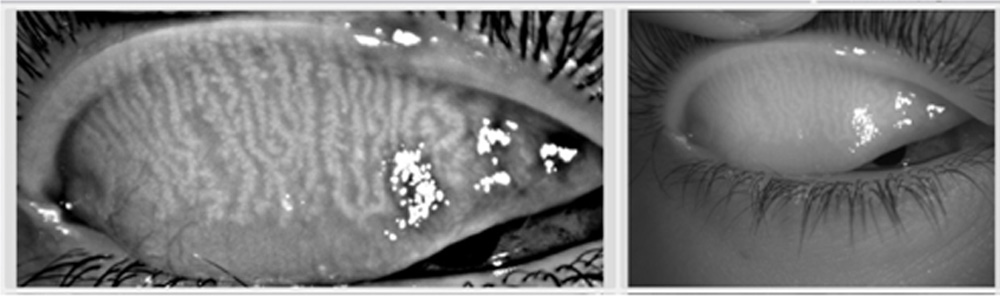
Meibography is anon-invasive specialized imaging study developed exclusively for the purpose of directly visualizing the morphology of meibomian glands in vivo6-9(Fig. 1). Meibography was performed on all patients with Keratograph4 (OCULUS, Wetzlar, Germany) 10-11. Keratograph 4 primarily functions as a corneal topographer, but can also be used to undertake pupilometer, utilizing an in-built IR bulb and camera (Fig. 3, left). The participant is seated and asked to focus on the target at the centre of the placido disc and then the upper and lower lids everted using a cotton-tipped applicator. The intensity of the IR illumination can be manually adjusted with software built into the device, but is kept consistent throughout the study. When observing the palpebral surface of the eyelids illuminated with IR light, the Meibomian glands are revealed and can be captured using either video or still images (Fig. 3, right).Meibo-Scan reveals morphological changes in the glandular tissue
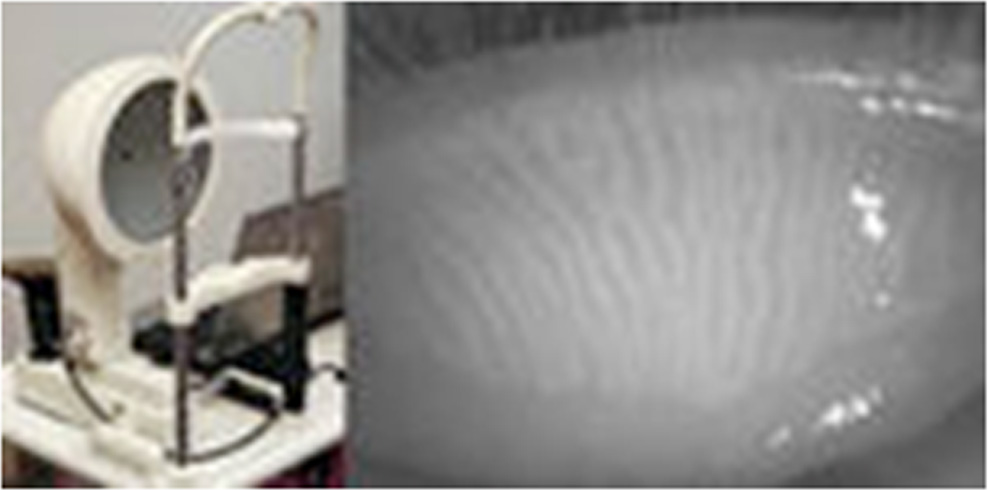
Figure 3.The OCULUS Keratograph4; the infrared diode intended for pupillometryis used as an infrared illumination source for meibography (left). An everted superior eyelid reveals long thin MGs running vertically on the palpebral side as visualized by the OCULUS Keratograph 4 in infrared light (right).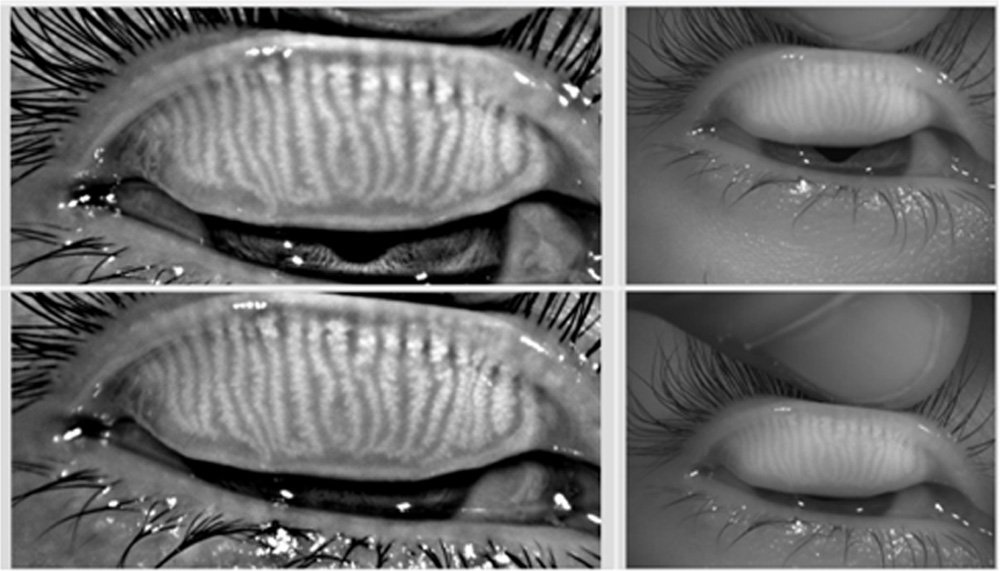
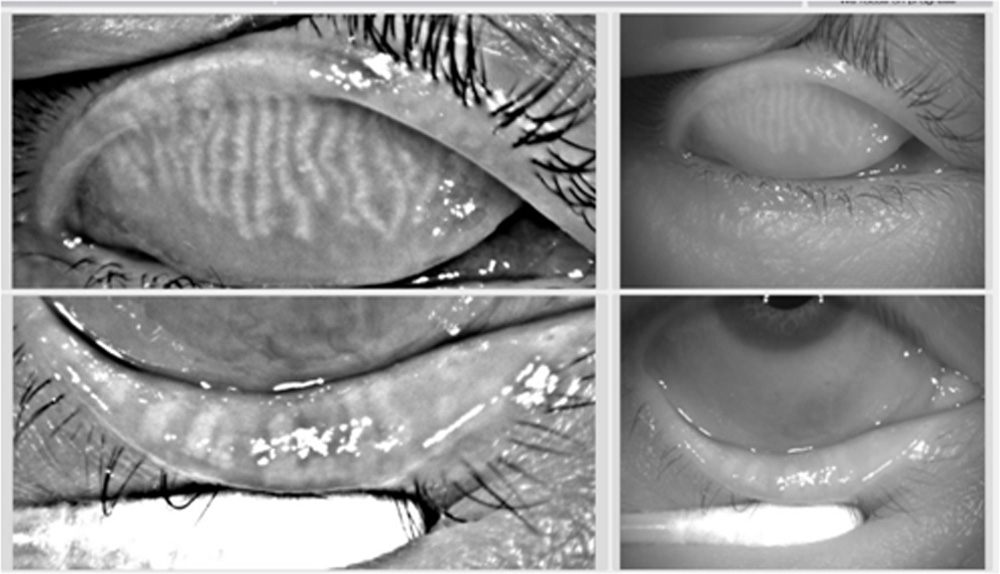
Figure 4. (0.06MB).The entire superior palpebral surface could be imaged using the OCULUS Keratograph 5M (right). A processed image of the same eyelid highlights the Meibomian glands to make them more visible (left).
Results:
There were a total of 100 children and 126 adults in the study;inadult’s group 84 males and 42 females and in Children group 68 boys and 32 girls. (Fig1). MGD was observed in 90% of the adults while only 10% in children. In both groups, both Blepharitis and MGD were more in males than females.
Bacterial culture was positive in 73% of adults and 40% of children (fig2).
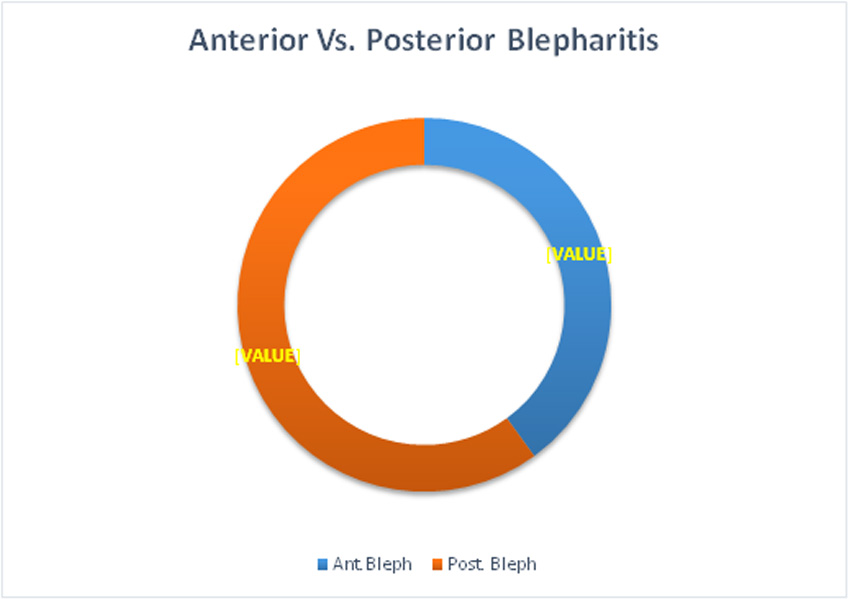
40% of the patients had Anterior Blepharitis and 60% had Posterior Blepharitis (fig.3). Anterior Blepharitis was more in children; 78% of children had anterior Blepharitis and 80% of the children with anterior blepharitis had ocular allergies.(fig4). Association of anterior blepharitis with dermatitis and dandruff was observed in few patients.
Posterior Blepharitis was observed more in adults and 90% of the adults with posterior blepharitis showed MGD and was associated with Dry eye while only 10% anterior blepharitis showed MGD (Fig5)
Only 40% of the anterior blepharitis was showed positive culture result and the organism was staphylococcus epidermis.73% of the posterior Blepharitis had positive culture results and the organisms were staph. Aureus and epidermidis. 10% of patients with posterior blepharitis had marginal keratitis. Patients with distorted glands, shortened glands and absence of glands and madarosis were also seen in posterior blepharitisfig6.
Anterior Blepharitis with normal Meibomian gland. But presence of follicles of allergic conjunctivitis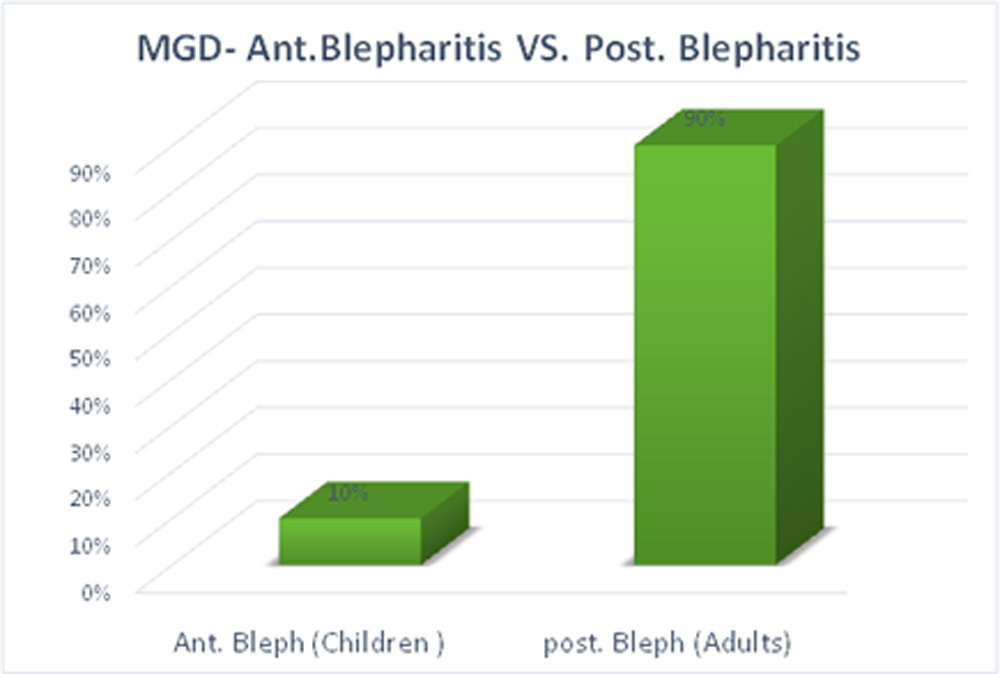
Discussion
In our study majority of the adults fall into the category of posterior Blepharitis and the majority of children had anterior Blepharitis. Anterior blepharitis is defined as inflammation affecting the lash margin, involving both staphylococcal and seborrheic blepharitis; with anterior blepharitis the inflammation is localized to the lid margin anterior to the gray line. Although precise mechanism behind the development of anterior blepharitis is unclear, three convergent pathways likely underlie the pathophysiology: 1. direct bacterial infection, 2. Exotoxin hypersensitivity and 3. Delayed cell – mediated immune hypersensitivity response12. In this study 40% of the anterior blepharitis showed positive culture result and the organism was staph epidermidis. In addition to infectious causes, anterior blepharitis also had seborrheic dermatitis association. Seborrhea is a papulo-squamous disorder of the trunk, scalp, and face. It can be characterized by intermittent, active phases, manifesting as burning, scaling, and itching, alternating with inactive periods13.

Clinical presentations range from mild dandruff to exfoliative erythroderma. Seborrheic blepharitis occurs when the pilosebaceous glands located within the lid margin become involved, primarily affecting the glands of Zeis, and the meibomian glands to a lesser degree. In seborrheic blepharitis, there is less inflammation and telangiectasia than staphylococcal blepharitis, and more over it commonly presents with greasy lashes that cause matting across the anterior lid margins of both eyes14
The identified culture positive for S.epidermidis in anterior blepharitis in our study support the theory of toxins released by Staphylococcal organisms or seborrheic dermatitis is the main cause of anterior blepharitis. Symptoms such as mild sticky eyelids, thicker margins of the eyelid, and missing eyelashes occur due to Staphylococcal blepharitis.
A strong correlation of adults and posterior blepharitis was observed in this study. Posterior blepharitis is characterized by inflammation of the posterior lid margin and has various etiologies, including MGD, infectious and allergic conjunctivitis, as well as systemic conditions such as rosacea, eczema, and atopy1
90% of adults with posterior blepharitis had Meibomian gland dysfunction and are associated with dry eyes. Meibomian glands are modified, holocrine, sebaceous glands that are embedded in the tarsal plate of the both the upper and lower eyelid and excrete lipid onto the surface of the eye to form the lipid layer of the tear film to reduce aqueous tear evaporation15. MGD is defined as a chronic, diffuse abnormality of the meibomian gland characterized by terminal duct obstruction and qualitative or quantitative changes in glandular secretion1.
Dysfunction of the meibomian gland (MGD) is a common eyelid disorder with the incidence increasing with age 16-19. MGD is also a major cause of evaporative dry eye disease (EDED) with loss of glands resulting in decreased tear film lipid, increased aqueous tear evaporation and increased tear film Osmolarity leading to ocular surface changes, unstable tear film and blepharitis20.
Deficiencies in meibum may be responsible for the symptoms experienced in MGD blepharitis. Hyper keratinization related to MGD has been shown to play a role in decreased Meibomian gland secretions and obstruction.21 Similar sequela have shown a link between higher rates of tear evaporation and related secondary corneal surface damage associated with DES symptoms in blepharitis patients.20
Prolonged Meibomian gland obstruction leads to bacterial colonization. Eventually, inflammatory mediators are formed and released from lipolytic enzymes that are produced from bacteria such as Staphylococcus epidermidis, S. aureus, Propionibacterium acnes, and Cornebacterium22. Lipolytic enzymes released by bacteria cause highly irritating free fatty acids to breakdown the lipids in the tear film contributing to the loss of tear film integrity. (This loss of tear film stability allows for increased aqueous tear evaporation, leading to signs and symptoms of evaporative dry eye23
In our study 73% of posterior blepharitis had culture positive with the organisms of staph. Aureus and epidermidis. Association of Posterior blepharitis with dry eyes, madarosis and poliosis also noted in our study fig7. Another clinical feature observed with chronic posterior blepharitis was that marginal keratoconjunctivitis which was seen in 10% cases and they responded well to the low dose of steroid or subsided without treatment. Another study also reported the presence of keratoconjunctivitis in chronic blepharitis24.
Conclusion
Our study reported the strong association of posterior blepharitis with Meibomian gland dysfunction and Anterior Blepharitis with allergy. Meibography was more than a diagnostic tool, a self-explanatory and impressive in making the patient understand the condition which makes the treatment easier
References
- Nelson JD, Shimazaki J, Benitz-de-Castillo JM, et al. The international workshop on meibomian gland dysfunction: report of the definition and classification subcommittee. Invest Ophthalmol Vis Sci. 2011; 52:1930–1937.
- John T, Shah AA. Use of azithromycin ophthalmic solution in the treatment of chronic mixed anterior blepharitis. Ann Ophthalmol. 2008; 40:68-74.
- McCulley JP, Shine WE. Eyelid disorders: the meibomian gland, blepharitis, and contact lenses. Eye Contact Lens. 2003;29(suppl 1):S93-S95; discussion S115-18, S192-94
- McCulley JP, Shine WE. The lipid layer of tears: dependent on meibomian gland function. Exp Eye Res. 2004;3:361-65
- Raskin EM, Speaker MG, Laibson PR. Blepharitis. Infect Dis Clin North Am. 1992; 6:777-87).
- Rife L., Nii D., Luttrull J.K., Wilson L., Smith R.E. In vivo biomicroscopy and photography of meibomian glands in a rabbit model of meibomian gland dysfunction. Invest Ophthalmol Vis Sci. 1982; 22:660–677.)
- Jester J.V., Nicolaides N., Smith R.E. Meibomian gland studies: histologic and ultrastructural investigations. Invest Ophthalmol Vis Sci. 1981; 20:537–547. [PubMed]
- Lee S.H., Tseng S.C. Rose bengal staining and cytologic characteristics associated with lipid tear deficiency. Am J Ophthalmol. 1997; 124:736–750. [PubMed]
- Mathers W.D., Shields W.J., Sachdev M.S., Petroll W.M., Jester J.V. Meibomian gland dysfunction in chronic blepharitis. Cornea. 1991; 10:277–285.
- Srinivasan,K. Menzies,L. Sorbara,L. Jones Meibography of the upper lid Optician, (2011), pp. 12-14.
- Srinivasan,L. Sorbara,L. Jones,W. Sickenberger Imaging the structure of the meibomian glands Contact Lens Spectrum, (2011), pp. 52-53)
- Christopher M Putnam Diagnosis and management of Blepharitis: an optometrist’s perspective .clinical optometry2016; 8: 71-78.
- Jackson WB. Blepharitis: current strategies for diagnosis and management.Can J Ophthalmol. 2008; 43(2):170–179.
- . Raskin EM, Speaker MG, Laibson PR. Blepharitis. Infect Dis Clin North Am. 1992; 6(4):777–787.
- Jester JV, Nicolaides N, Smith RE. Meibomian gland studies: histologic and ultrastructural investigations. Invest Ophthalmol Vis Sci. 1981; 20:537–47.
- Hom MM, Martinson JR, Knapp LL, Paugh JR. Prevalence of Meibomian gland dysfunction. Optom Vis Sci. 1990; 67:710–2.
- Lemp MA, Nichols KK. Blepharitis in the United States, a survey-based perspective on prevalence and treatment. Ocul Surf. 2009; 2009(7):S1–S14.
- Ong BL. Relation between contact lens wear and Meibomian gland dysfunction. Optom Vis Sci. 1996; 73:208–10.
- Ong BL, Larke JR. Meibomian gland dysfunction: some clinical, biochemical and physical observations. Ophthalmic Physiol Opt. 1990; 10:144–8.
- Shimazaki J, Sakata M, Tsubota K. Ocular surface changes and discomfort in patients with meibomian gland dysfunction. Arch ophthalmol.1995;113:1266–70
- Obata H. Anatomy and histopathology of human meibomiangland.Cornea. 2002;21:S70–S74
- Dougherty JM, McCulley JP. Comparative bacteriology of chronic blepharitis. Br J Ophthalmol. 1984; 68(8):524–528.)
- Bron AJ, Tiffany JM. The contribution of meibomian disease to dry eye. Ocul Surf. 2004;2:149–165
- Huber-Spitzy V, Baumgartner I, Bohler-Sommeregger K, GrabnerG.Blepharitis – a diagnostic and therapeutic challenge: report on 407 consecutive cases. Graefes Arch ClinExpOphthalmol. 1991;229(3):244–247
- Lambert DW. Physiology of the tear film. In: Smolin G, Thoft RA, editors. The Cornea. 3rd ed. Noida, India: Lippincott Williams and Wilkins; 2001. p. 439.
Leave a Comment