
Dr. Khurshed M Bharucha, B05942, Dr.
Rahul Deshpande, Dr. Shilpa Joshi, Dr. (col) Madan Deshpande
Abstract:
Purpose: To study surgical induced change in Posterior corneal curvature (PCC) due to various types of incisions in phacoemulsification surgery
Methods: A prospective observational study of 100 subjects aged 30-80 yrs undergoing phacoemulsification surgery. The subjects were randomly assigned to undergo phacoemulsification surgery with any one of the four types of incisions i.e. superior clear corneal (SCC), temporal clear corneal (TCC), On-axis clear corneal (OACC) and superior sclera-corneal incision (SCI). All clear corneal incisions were made by standard 2.8mm keratome in a triplanar technique. Sclerocorneal incision was taken 1mm behind limbus in a triplanar fashion.The subjects underwent corneal evaluation by Scheimpflug imaging (Pentacam HR) preoperatively and 1 week postop. Surgical induced change in PCC was analysed statistically for the four incision groups.
Results: SCC incision caused the maximal Posterior Surgical induced Astigmatism (PSIA) mean value of 0.43D. OACC and SCI incisions resulted in minimal PSIA (mean value -0.17 and 0.18D).The difference between both OACC and SCI groups v/s SCC incision was statistically significant (p-values 0.015 and 0.002). TCC incision also caused less PSIA as compared to SCC incision but was not statistically significant .
Conclusion: In view of the increasing importance of posterior corneal curvature, we evaluated PSIA for various incisions. However small the implications on surgical outcomes, this aspect need further evaluation for a complete assessment. We found OACC and SCI incisions to induce minimal PSIA as compared to SCC and TCC. This aspect will need further evaluation to be incorporated into Toric IOL power calculations.
Keywords: posterior corneal curvature, surgical induced astigmatism, phacoemulsification, Scheimpflug
Introduction: Posterior corneal curvature (PCC) had been one of the parameters of the eye that till recently was not possible to measure. Now with the advent of newer technologies like Scheimpflug and OCT devices this lacuna in our knowledge has been filled.
The posterior surface of cornea though being steeper than the anterior contributes about less than 1/10th the effect of the anterior curvature toward the total corneal refractive power. This is because of the difference of refractive index of cornea(1.376) vs aqueous(1.336) is just 0.04; whereas the refractive index at the air-corneal interface changes by 0.376. This results in significant refraction of rays at the anterior surface vis a vis the posterior.(1)
In the era before these devices calculations of corneal refractive power were based on certain assumptions. It was assumed that the curvature of the posterior cornea and anterior corneal surface were in a constant ratio. An artificial index was used to convert anterior keratometry to total corneal power. This gave higher reading of total corneal power by upto 1D.(1)
In view of the inability to measure posterior curvature Dr Douglas Koch and team proposed the Baylor’s nomogram for toric iol calculations. They presumed a WTR astigmatism of posterior curvature and made corrections to the anterior corneal power to evauate the total corneal power.(2)
Now with the availability of devices it is possible to measure the posterior corneal curvature and its nuances. We studied one such aspect in the form of changes in posterior corneal curvature changes as a result of various incisions for phacoemulsification.
Methods: This prospective observational study was carried out at a tertiary eye care institute after approval by institutional ethics committee.
We enrolled patients undergoing phacoemulsification cataract surgery at this institute. Informed consent was taken from the patients for participation in the study.
We recruited 100 eyes of 100 patients for the study over the study period of one year. Patients were randomly assigned to undergo phacoemulsification with one of the following incisions namely: On-Axis Clear Corneal Incision (OACC), Superior Clear Corneal Incision (SCC), Temporal Clear Corneal Incision (TCC) and Sclero Corneal incision (SCI) placed at 12 o’clock.
The subject underwent a detailed pre-operative assessment- history, general and systemic examination, best corrected visual acuity (BCVA) by LogMAR chart, refraction by auto refractometer, slit lamp biomicroscopy, detailed fundus examination by 90 D lens, and routine preoperative investigations which includes keratometry, axial length and IOL power calculation by optical biometer IOL Master( Carl Zeiss Meditec AG, Germany), measurement of anterior corneal curvature, posterior corneal curvature, total corneal astigmatism, anterior chamber depth and pachymetry by rotating Scheimpflug camera (Pentacam; Oculus, Wetzlar, Germany).
Patients with previous ocular surgery, trauma, corneal disease and history of wearing contact lens were excluded from the study.
Preoperative marking of the Axis was done on slit lamp by Nuijts-Lane Pre-op Reference Marker with Bubble. The subjects underwent a standard phacoemulsification procedure with the randomly assigned type of main incision, SCC, TCC, OACC or SCI. All clear corneal incisions were made by standard 2.8mm keratome in a triplanar technique. Sclerocorneal incision was taken 1mm behind limbus in a triplanar fashion. . Two 1mm sideports were created at 60degrees left and 90 degrees right of the main incision for irrigation and aspiration.A well centred capsulorrhexis was aimed for and phacoemulsification was done in stop and chop or direct chop method by two designated surgeons. Two 1mm side ports were created at 60degrees left and 90 degrees right of the incision for irrigation and aspiration. A non-toric foldable acrylic IOL was implanted in the bag.
The subjects underwent corneal evaluation by Scheimpflug imaging (Pentacam HR) preoperatively and 1 week postop.
Results:
Posterior corneal parameter of flatK and steepK (magnitude and axis) were measured preoperatively and 1 week post operatively. The posterior surgical induced astigmatism (PSIA) was calculated using an online calculator for each case. The mean PSIA for each type of incision was calculated.
We found that the PSIA induced in Superior clear corneal incision was the largest (Mean PSIA – 0.43 ±0.32D). Mean PSIA of On-Axis incision (OACC) and sclerocorneal incision (SCI) were the least at 0.17 ±0.12D and 0.18 ±0.13D respectively. The temporal incision (TCC) was somewhere inbetween with an induced PSIA of 0.28 ±0.21D. (Figure 1)(Table 1)
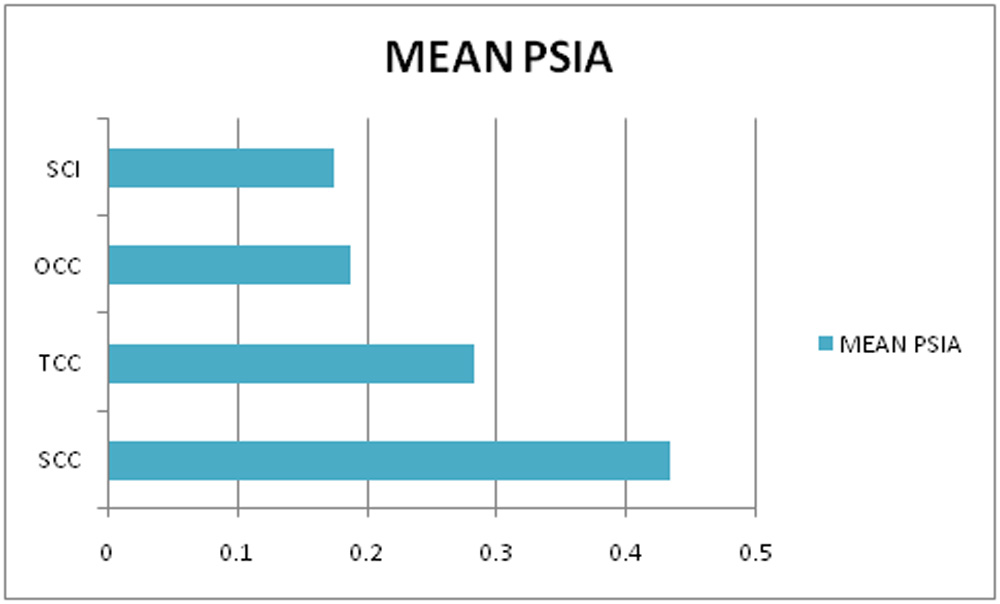
Figure 1: Mean PSIA induce by various incisions
| Type of incision | Magnitude | Test | P value | Interpretation |
| On Axis | 0.17+0.13 | Kruskal-Wallis Test | 0.002 | The magnitude of astigmatism between the groups was significantly different. |
Table 1:Comparison of Posterior SIA Magnitude
Surgical induced change in PCC was analysed statistically for the four incision groups. The difference in PSIA induced by superior incisions (SCC) vs OACC and SCI was statistically significant (P-value 0.015 and 0.002).Temporal incisions(TCC) showed a PSIA lesser than Superior incisions(SCC) but was not statistically significant (P-value 0.255).(Table 2)
| Incision 1 | Incision 2 | P value | Interpretation |
| On Axis=0.17+0.13 | SCI=0.18+0.12
SUP=0.43+0.33 TCC=0.27+0.22 |
0.74
0.015 0.12 |
The magnitude of astigmatism with SCI and TCC incision was comparable with that of On Axis incision while that with SUP incision was significantly more. |
| SCI=0.18+0.12 | SUP=0.43+0.33
TCC=0.27+0.22 |
0.002
0.06 |
The magnitude of astigmatism wit TCC incision was comparable with that of SCI incision while that with SUP incision was significantly more. |
| SUP=0.43+0.33 | TCC=0.27+0.22 | 0.255 | The magnitude of astigmatism with TCC incision was comparable with that of SUP incision. |
Table 2: PSIA -Pairwise comparisons of incision types
We also evaluated the pre-existing type of astigmatism predominant on the posterior surface of cornea. We found that 63.48% subjects had WTR, 14.78% ATR and 21.73% oblique posterior astigmatism.(Figure 2)
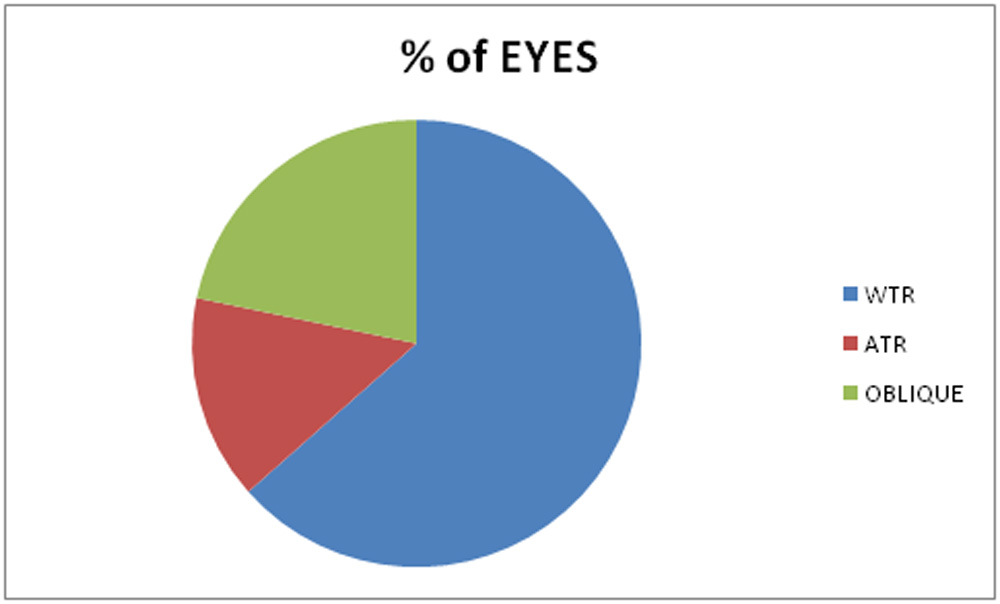
Figure 2: Types of pre-existing Posterior corneal astigmatism
Discussion:
Posterior corneal curvature has been till recently difficult to measure. An arbitrary constant ratio between Anterior and Posterior curvatures was assumed after evaluating demographic data.
This ratio was used by most instruments to assess total corneal power and incorporate it in various formulae for calculating IOL power. This method was prone to error and unsatisfactory results.
Koch D et al proposed the Baylor nomogram to compensate for the posterior corneal astigmatism in Toric IOL power calculations. They suggested subtracting 0.5D from with the rule(WTR) astigmatism and add 0.3D for against the rule(ATR)astigmatism to cater for the posterior corneal astigmatism.
Now with the availability of devices such as slit scanning videokeratoscope, Scheimpflug imaging and AS-OCT, which directly measure the posterior corneal surface parameters we are better informed to make more accurate calculations. Considering not only the anterior but also the posterior corneal curvature when planning refractive cataract surgery could lead to a more predictable result.
We studied the surgical induced change in posterior corneal curvature due to various types of surgical incisions in phacoemulsification. As far as we are aware from literature, there has been no such evaluation studying PSIA after phacoemulsification done earlier.
Sano M et al evaluated the influence of posterior corneal astigmatism on postoperative refractive astigmatism after phacoemulsification. They concluded that if we consider actual posterior corneal curvature measurements for IOL calculations, postoperative refractive astigmatism may be reduced.(4)
Many studies have evaluated SIA of the anterior surface and its impact on postoperative astigmatism. Hashemi H et al studied the impact of location of incision in cataract surgery on induced astigmatism. They found that the temporal incision was associated with least astigmatism and on-axis incisions were associated with good results in correcting pre-existing astigmatism.(5)
Rho CR et al evaluated surgically induced astigmatism (SIA) when the clear corneal incision is located on the preoperative steep meridian of the corneal astigmatism in phacoemulsification. They advocated placing the corneal incision on the steep meridian in eyes with corneal astigmatism higher than 0.50 D. (6)
With the availability of newer devices it may be of some value to study the various nuances of the posterior corneal curvature, a small part of which we have tried to study in this paper.
References:
- Koch DD. The Enigmatic Cornea and Intraocular Lens Calculations: The LXXIII Edward Jackson Memorial Lecture.Am J Ophthalmol. 2016 Nov;171:xv-xxx.
- Koch DD, Ali SF, Weikert MP, Shirayama M, Jenkins R, Wang L. Contribution of posterior corneal astigmatism to total corneal astigmatism. Journal of Cataract & Refractive Surgery. 2012;38:2080-7.
- Koch DD, Jenkins RB, Weikert MP, Yeu E, Wang L. Correcting astigmatism with toric intraocular lenses: effect of posterior corneal astigmatism. J Cataract Refract Surg. 2013 Dec;39(12):1803-9
- Sano M, Hiraoka T, Ueno Y, Itagaki H, Ogami T, Oshika T. Influence of posterior corneal astigmatism on postoperative refractive astigmatism in pseudophakic eyes after cataract surgery. BMC Ophthalmology. 2016;16:212.
- Hashemi H, Khabazkhoob M, Soroush S, Shariati R, Miraftab M, Yekta A. The location of incision in cataract surgery and its impact on induced astigmatism. Curr Opin Ophthalmol. 2016 Jan;27(1):58-64
- Rho CR, Joo CK. Effects of steep meridian incision on corneal astigmatism in phacoemulsification cataract surgery. J Cataract Refract Surg. 2012 Apr; 38(4):666-71
Leave a Comment