
Dr. Rushita R Kamdar, R15509, Dr. Vineet Joshi, Dr. Neeraj Shah, Dr. Jagadeesh Kumar Reddy K
Abstract:
Purpose: To eliminate PCO formation by using a hydrophobic acrylic foldable ring.
Methods: A prospective, non-randomized case series of 30 patients with senile cataract who underwent phacoemulsification.The ring is inserted into the bag after IOL implantation and fits under the anterior capsular margin, pushing the IOL posteriorly. This brings the IOL optic in close apposition with the posterior capsule, eliminating space for the proliferation of lens epithelial cells to form PCO. Follow up was at 1,6,24,52 weeks with visual acuity, IOP, anterior and posterior segment examination.
Results: Postoperative BCVA of all patients was 20/30 or better. No evidence of PCO was noted in any patient until last follow up.
Conclusion: This ring may provide an ideal one stop solution for cataract surgery in community ophthalmology by eliminating the costs, complications associated with interventions for PCO and the need to revisit the hospital. Long term follow up is needed to validate this device.
Introduction :
India is home to 1/4th of the worlds blind population. Cataract is the biggest cause of curable blindness in India as well as the world. Modern surgical technique and advances in intraocular lenses has given us the capability to deliver dramatic results. Now with new technology and equipment, an intraocular lens (IOL) has the potential to improve a patient’s acuity and refine the refractive error to a given target.
But, posterior capsule opacification (PCO) is one such impediment that withholds cataract surgery from reaching its zenith. PCO is the most frequent postoperative complication associated with decreased vision after intraocular lens (IOL) implantation. The incidence was reported to be 20.1% a mean of 3 years after surgery in the literature published between 1990 and 1998.[1]Risk factors precipitating PCO development are young age , incomplete cortical removal, material and design of IOL.[1]
Due to the presence of a potential space ( depicted by arrow in Figure 1) between the IOL and the posterior capsule, the lens epithelial cells from the equator may migrate posteriorly and proliferate onto the the posterior capsule within the visual axis.( Figure 1)
Figure1 : Diagrammatic representation of IOL within capsular bag and migration of lens epithelial cells.
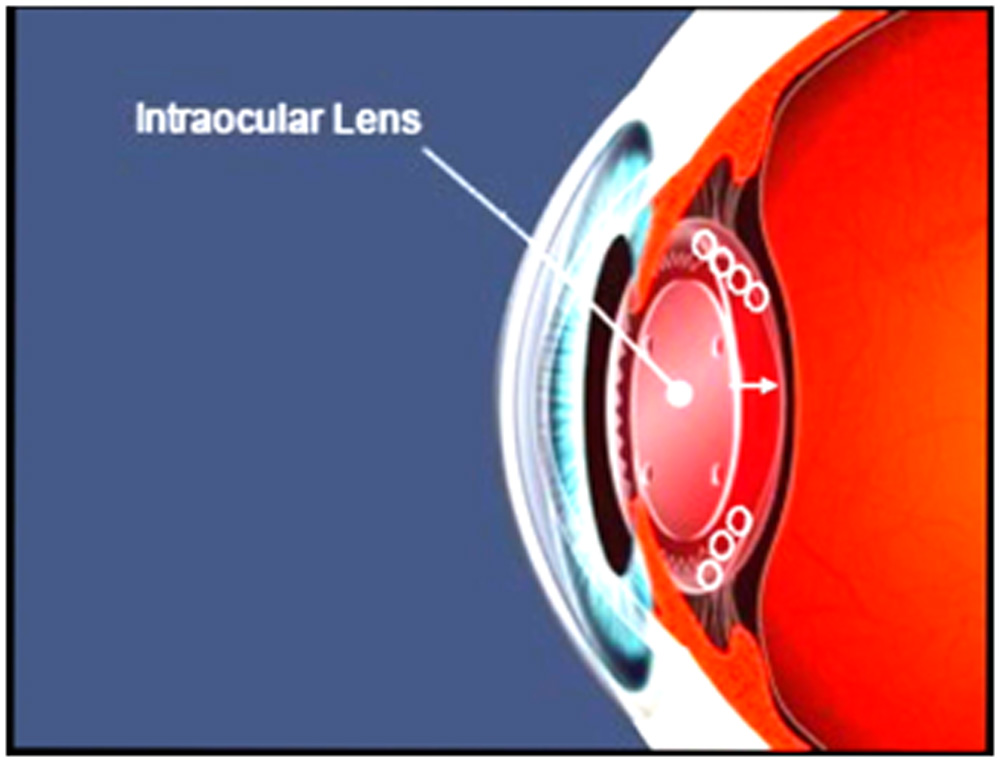
The natural course would be to do a Nd-YAG / Surgical Capsulotomy to clear off the opacity from the visual axis. But YAG Capsulotomy may pose a risk in high myopes, those with a retinal detachment, and those with Diabetes Mellitus. At times, it could result in IOP spike and Cystoid Macular edema and rarely, IOL dislocation.
Mechanical, physical, and immunological methods have been developed to prevent PCO by removing or killing lens epithelial cells (LECs); however no method proved satisfactorily practical, effective, and safe as a routine clinical procedure.[ ] The world is now moving from knee jerk reactive medicine to preventive medicine. We, describe our initial results of a hydrophobic acrylic PCO preventing ring implanted after IOL insertion into the capsular bag.
Material and methods:
Ours is a prospective, non-randomized clinical case series carried out at a tertiary eye hospital in South India. Ethics Committee approval was obtained. Informed consent was obtained from all patients enrolled between June 2015 till June 2016. The study cohort comprised presbyopic ametropic patients in the age group 40-65 years with cataract. 30 eyes of 23 patients were enrolled in this study. They underwent standard phacoemulsification with implantation of a foldable acrylic Intraocular lens over which the PCO prevention ring was implanted into the capsular bag. Eight patients had bilateral implantation of the ring. Patients were enrolled after careful selection and screening. Exclusion criteria were a history of glaucoma, retinal detachment, corneal disease, corneal surgery, ocular inflammation, neuroophthalmic disease, macular degeneration or retinopathy, keratometric cylinder greater than 1.00 diopter (D) and senile miotic pupils, patients with traumatic mydriasis or iris coloboma. All patients had a preoperative examination that included autorefraction, tonometry, uncorrected and corrected distance visual acuity (UDVA, CDVA), near visual acuity, biometry (IOL Master 500, Carl Zeiss Meditec AG), subjective and cycloplegic refractions, slit-lamp evaluation and dilated fundus evaluation. Visual acuity was measured at distance and near vision with a Snellen visual acuity chart and converted to logMAR scores. Axial length (AL), anterior chamber depth (ACD), and keratometry values from the IOL Master were used for IOL power calculation. All eyes were targeted for -0.50 D Myopia to compensate for the posterior IOL displacement. UDVA and CDVA, AR, Acceptance, uncorrected near visual acuity and distance-corrected near visual acuity (UNVA and CNVA), were evaluated at 1 week, 1 month, 6 months and 10 months later. Spectacle independence for the operated eye and patient satisfaction was also analyzed.The IOL implanted was a single piece hydrophobic acrylic foldable 13 mm lens with an optic of 6mm.
Ring :- This PCO preventing ring is made up of a foldable hydrophobic acrylic material with an outer diameter of 9 mm , inner diameter of 6.5 mm and thickness of 0.40 mm. It can be implanted via a standard 2.4 mm incision used during phacoemulsification using a conventional IOL cartridge and injector and positioned over the Intraocular lens within the capsular bag.It is then dialed into position under the capsular margin using a Sinskey’s hook. The ring snugly fits into the periphery irrespective of the size and shape of the anterior capsulorhexis. It also strengthens the capsular bag, thereby providing excellent IOL centration within the bag whatsoever the material/ design of IOL. It also safeguards against lens tilting. It must be implanted over the IOL in order to push the lens posteriorly causing the optic of the lens to come in contact with the posterior capsule thus eliminating any space for the lens epithelial cells to proliferate. This posterior displacement of the lens must be accounted for while selecting the IOL power to counter the induced hyperopia due to the small posterior shift.
Surgical Technique :- The surgeries were performed by a single surgeon. The pupils were dilated with Tropicamide + Phenylephrine and Cyclopentolate. Proparacaine (0.5%) and Lignocaine jelly (4%) was applied. Lens extraction was performed using a standard phacoemulsification technique through a 2.8mm incision. All incisions were made on the steepest corneal meridian to neutralize corneal astigmatism. After phacoemulsification, the foldable Intraocular lens was inserted through a 2.8mm corneal incision using the injector into the capsular bag ensuring adequate centration followed by implantation of the ring over the lens within the capsular bag . Post operatively, patients were asked to instill Gatifloxacin (0.3%) with Loteprednoletabonate (0.5%) tapered over a month along with Nepafenac (0.03%) for 60 days.
Results:
In all, 30 eyes of 23 patients underwent PCO ring implantation over the IOL. The mean follow up of these patients was recorded as 15.5 months (13 -18 months). The mean patient age was calculated to be 55 years (46-64 years). 16 were males and 14 were females. Postoperatively, all patients had a well centred IOL within the capsular bag with a normal Anterior Chamber. Figure 2,3depicts post-operative anterior segment photograph of an eye in which this PCO ring was implanted over the IOL
Figure 2 &3 : Post operative slit lamp images
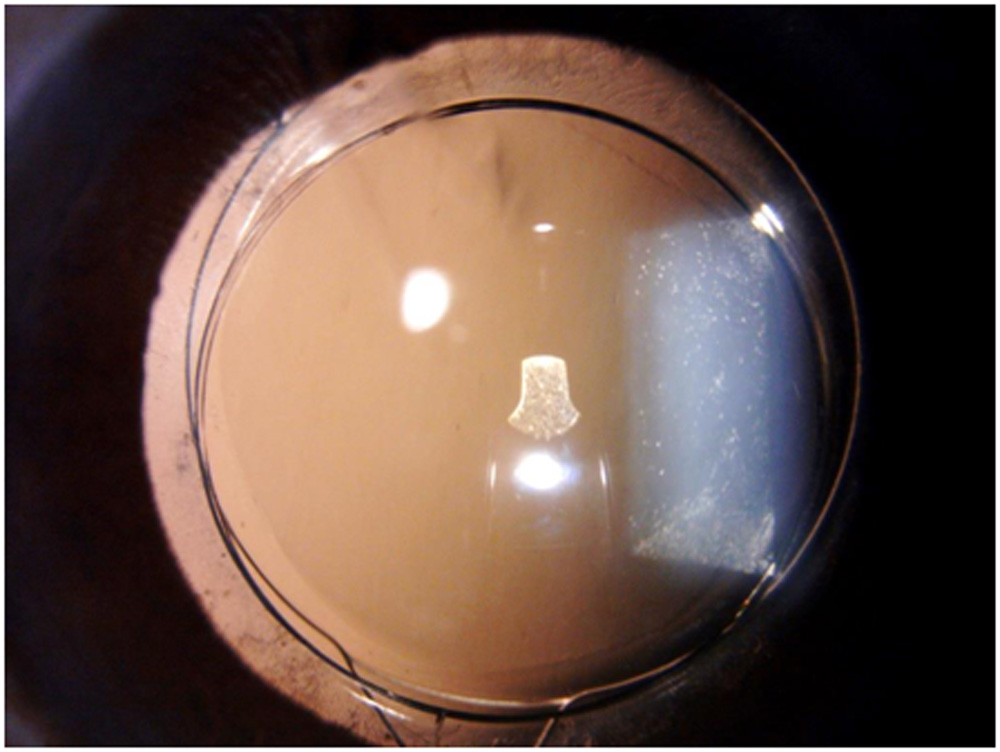
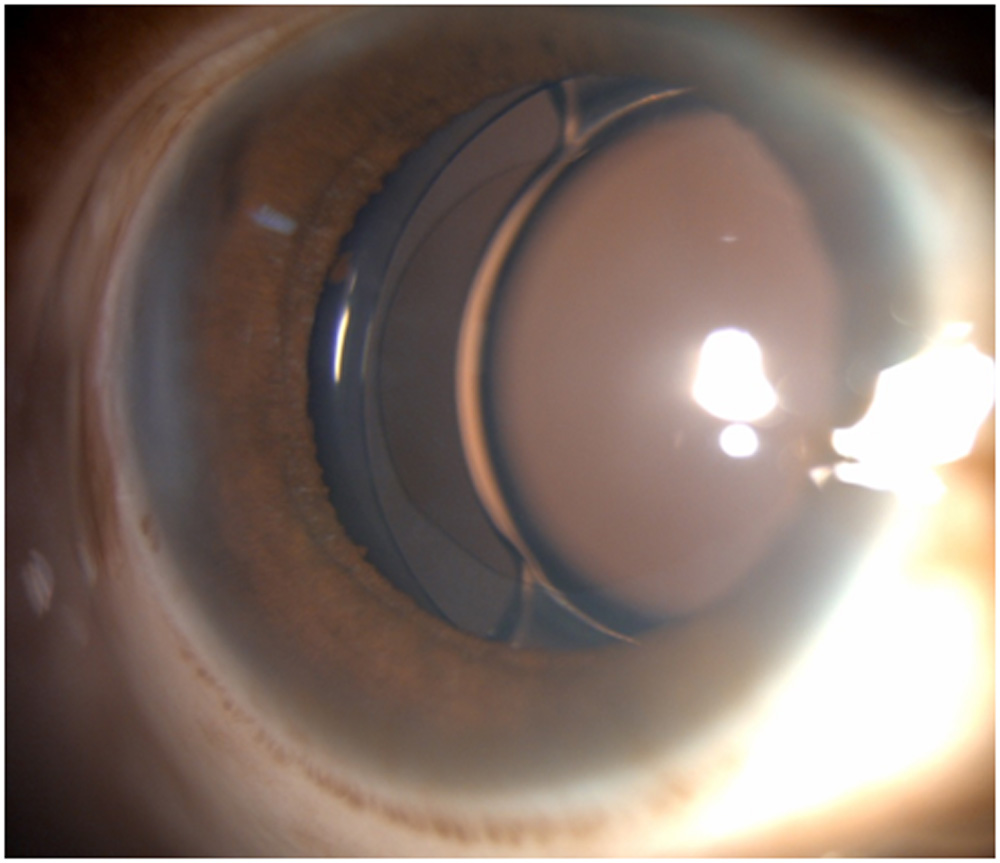
Post operative slitlamp observation indicated a perfect shrink wrap sealing of the anterior and posterior capsule with the 360 degree square profile of the ring.Good centration of IOL is achieved in all 30 eyes irrespective of the anterior capsulorhexis size and shape.PCO ring achieves good centration of the implanted IOL’s optic with any size of the capsular bag irrespective of the IOL’s haptic design.
IOL power calculation done with SRK T formula was accurate upto ±0.30 D ( Mean).Hence it was essential to account for the posterior shift of IOL while calculating the IOL power.
No posterior capsular folds were noted in any of the eyes implanted with this ring.No Lens Epithelial cell outgrowth was noted in any eye with a ring during the postoperative period.
All 30 eyes (100%) had BCVA for distance 20/20 and near vision with distance correction N6 which was well maintained till their last follow up.(Figure 3)UCVA of 27 eyes (90%) is 20/30 or better, and remaining 3 eyes is 20/40. (Figure 4)
All the patients were highly satisfied with their subjective visual quality.
No tilting/ decentration of the lens was noted in any case.
Two eyes implanted with this ring showed an intense inflammatory reaction in the immediate post operative period. This was taken care of by stepping up the topical steroids to an hourly frequency till it abated. An unknown antigen antibody reaction to the hydrophobic material of the ring was suspected.
Discussion:
In our small series of 30 eyes , PCO was not observed in any of the eyes for a maximum follow up of 18 months. The mechanism of preventing the occurrence of PCO by thisdevice is postulated to be due to these two reasons. Firstly, with the ring present in the periphery , it prevents the migration of the lens epithelial cells onto the posterior capsule, hence prevents the nidus for opacity to develop. Secondly, the ring positioned over the IOL , pushes the IOL further posteriorly within the capsular bag so as to develop complete contact between IOL optic and posterior capsule, thus eliminating any space for the proliferation of lens epithelial cells.
This ring also strengthened the capsular bag thereby providing excellent centration of the IOL in the bag. Due to its scaffold- like effect this square edged ring also prevents the tilting of the IOL with capsular bag contraction. This is of special advantage with premium multifocal lenses.
Cortical cleaving hydrodissection has been an important basic step in PCO prevention by eliminating any nidus for development of opacity.[2] Another important step is lens haptic fixation in the bag. This has been age old teaching, the importance of which must be emphasized.
The future is now a PCO preventive device. Its 360 degree square edged profile of the ring ensured facilitated the creation of a sharp equatorial bend in the capsule. This hindered lens epithelial cell migration.
Nishi et al in an experimental study have found that the capsular bending ring , which is a modified capsular tension ring with a sharp edge, significantly inhibited lens epithelial cell migration onto the posterior capsule , preventing PCO.[3]
The ring’s 0.4mmwidth and its strategic placement led to a stretching effect on the capsule that prevented the anterior capsule from coming into contact with the IOL. As a result, LEC(Lens epithelial cell) outgrowth was prevented and the LECs under the anterior capsule were not induced to undergo fibrous pseudometaplasia.Anterior Capsule fibrosis and subsequent shrinkage was thus prevented.
Nishi and coauthors also support the concept that a discontinuous bend induces contact inhibition of migrating LEC’s and reduce PCO. However, their design was of an open ring with an eyelet.[4]
The common capsule tension ring is also an effective and safe for the reduction of the incidence of posterior capsule opacification as reported by Kim et al.[5]
Insertion of the ring did not prolong surgical time or complicate the surgery. It did not involve any major economical issues also. Hence it seems to be a cost effective device to combat PCO, but long term studies are yet to be done to confirm its validity.
Conclusion: The PCO ring prevents or delays PCO formation by eliminating the space between the IOL and posterior capsule. The PCO ring offers the perfect solution, in preventing PCO and achieving excellent IOL positioning in cataract surgery.
References:
- Schaumberg DA, Dana M, Christen WG, Glynn RJ. A systematic overview of the incidence of posterior capsule opacification. Ophthalmology 1998; 105:1213–1221
- Fine IH. Cortical cleaving hydrodissection. J Cataract Refract Surg 1992; 18:508–512)
- Nishi O, Nishi K, Mano C, et al. The inhibition of lens epithelial cell migration by a discontinuous capsular bend created by a band-shaped circular loop or a capsule-bending ring.Ophthalmic Surg Lasers 1998; 29:119–125.
- Nishi.O,Nishi K, Menapace R, AkuraJ.Capsular bending ring to prevent Posterior capsular opacification : 2 year follow up J Cataract Refract Surg 2001; 27:1359–1365
- Kim JH,Kim H, JooC.The Effect of capsular tension ring on posterior capsular opacity in cataract surgery. Korean J OphthalmolVol. 19:23-28, 2005
Leave a Comment