
Dr. Puneeth Isloor, I16596, Dr. Shrinivas M Joshi, Dr. Apoorva A G, Dr. Guruprasad Ayachit
Abstract
Purpose – To evaluate the demographics of Paediatric Rhegmatogenous Retinal detachments.and to analyse the visual outcomes and retinal re-attachment rates.
Methods – It was a retrospective study of 93 patients ≤18 yrs, who underwent Retinal detachment surgery over a period of two years (January 2014-August 2016) in a South Indian population of children. Demographic data, cause of RD,type of RD,status of macula, location of breaks, PVR grade& type, number of surgeries,type of surgery, retinectomy and its site ,tamponading agents used, retinal re-attachment , post-operative visual acuity,post –operative status on follow up for more than one month after surgery were noted.
Results -The demographic details are as follows – The .Male:Female ratio was 3.6:1 .Idiopathic (38.7%), Closed globe injury(25.8%)&myopia(22.6%)were the commonest causes. Commonest location of break was inferior(38%).46.2% had no PVR,33.3% grade C PVR with subretinal type(26.9%) being commonest. 27.9% had segmental buckle,75.3% had vitrectomy. Re-attachment was seen in 80.6% eyes. 42.9% of subjects with grade D PVR, 10.7% grade C,20% grade B did not have reattachment. Highest reattachment was seen among subjects with idiopathic RD (37.9%) followed by Closed Globe injury(24.2%)and Myopic RD(24.2%).There was no significant association between PVR grade and reattachment. Eyes with inferior retinectomy done for anterior PVR showed lower reattachment rates (p- 0.008).
Conclusion -Pediatric RD poses distinct challenges in terms of causation, higher rates of PVR & lower success rates.
Key words :Paediatric Retinal Detachment,PVR, Retinal re-attachment
Introduction
Paediatric rhegmatogenous Retinal detachments(RD) vary in presentation as compared to Adult retinal detachments. Most studies till date in pediatric RD have been conducted with small sample size. Most of the studies are descriptive studies .Statistical analysis of the outcomes are present in few studies conducted in the pediatric population. This study aims to add to the existing literature on Paediatric Retinal detachments in a South Indian population of children presenting to at a high volume centre .
Materials and methods
Objectives of the study
To study the demographics of paediatric retinal detachments and its various causes.
To compare visual outcomes and retinal re-attachement with PVR changes
Materials and methods
It was a retrospective study of 93 children aged less than 18 years who underwent Retinal detachment surgery from January ,2014 to August ,2016 at our institute. The charts of these patients were reviewed. All the surgeries had been performed by the same team of surgeons. Scleral buckling and Pars plana vitrectomy were the two main surgical procedures carried out for repair.Scleral buckling was performed with MIRA #277/279 with #240 band. .Pars Plana vitrectomy was done using 25 Gauge vitrectomy .Retinectomies had been done in cases with anterior PVR. Gas or silicon oil were used as tamponading agents. Demographic data, cause of RD,type of RD,status of macula, location of breaks, PVR grade& type, number of surgeries,type of surgery, retinectomy and its site ,tamponading agents used, retinal re-attachment , post-operative visual acuity,post –operative status on follow up for more than one month after surgery were noted. Retinal Re-attachment was considered when the retina was found to be attached for atleast one month following removal of silicon oil or after one month of gas injection at the time of surgery. PVR was graded as Grade A,B,C and D . The type of PVR was also noted. The demographics were listed .The associations were tested using Chi-square test.
Results
Demographics
In the study Majority of subjects were in the age group 11 to 15 years(46.2%),
Majority were males(78.5%) .M:F ratio was 3.6:1
Majority were phakic at presentation(64.5%)
Cause of R.D(Table 1)
Idiopathic (38.7%), Closed globe injury(25.8%)&myopia(22.6%)were the top 3 commonest causes. The most common location of the break was inferior retina(38%). Macula off RD was seen in ( 93.5%) . Rhegmatogenous RD was the commonest type of RD seen in 93.5%(
PVR grade and type(Table 2)
46.2% had no PVR,33.3% grade C PVR with subretinal type(26.9%) being the commonest
Type of surgery and tamponading agent
27.9% had segmental buckle,36.36% had belt buckle ,20% underwent Belt buckle with vitrectomy and 75.3% underwent vitrectomy.
Silicon oil was the most commonly used tamponading agent
Surgical outcomes(Table 3)
Re-attachment was seen in 80.6% eyes .
Majority had poor visual outcomes with vision of PL to 1/60 in 41.9%.
Interestingly , 84.9% of the patients did not end up with Phthisis Bulbi
Effect of grade of PVR on Retinal reattachment(Table 4)
There was no significant association between PVR grade and reattachment
50% of subjects with Grade 4 PVR did not have reattachment, 9.7% of Grade 3, 20% of Grade 1 did not have reattachment.
Effect of grade of PVR on visual outcomes
There was no significant association between PVR grade and Visual outcomes. Although subjects with Lower PVR grade had better visual outcomes. (χ 2 = 7.37, df = 8, p = 0.497)
Effect of number of resurgery on final vision outcome
There was no significant association between Number of Resurgeries and Visual outcomes despite the observation that the patients who underwent lesser number of res-surgeries had better visual outcomes (χ 2 = 11.53, df = 12, p = 0.484)
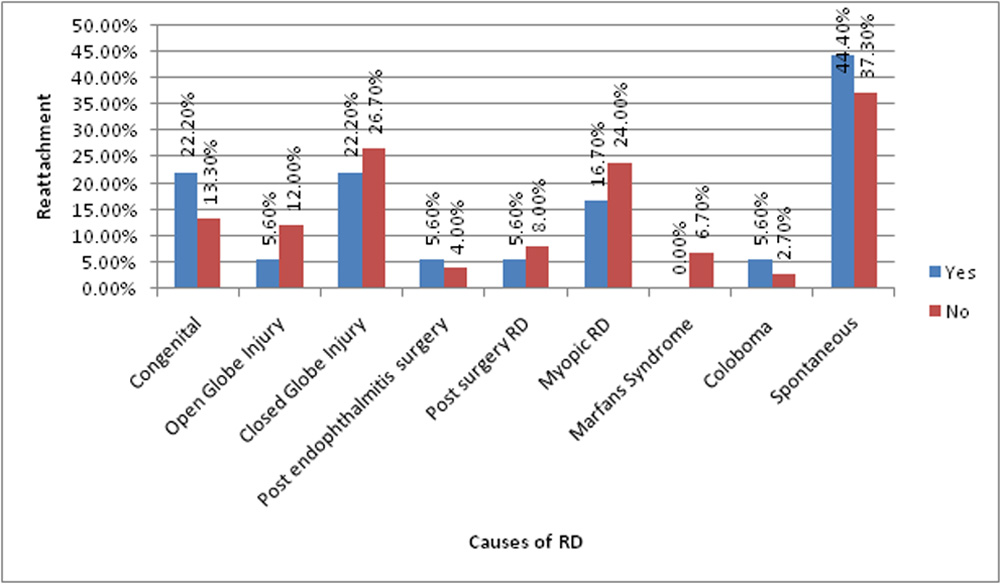
Effect of cause of retinal detachment on retinal re-attachment (Graph 1) Highest percentage of reattachment was seen among subjects with Idiopathic cause(44.4%) followed by Closed Globe injury(22%) . Least re-attachment was seen in Open globe injury (5.6%)
Reasons for Detached retina post RD surgery(Table 5)
Among subjects with no reattachment 33.3% of subjects had undergone Inferior retinectomy. However other factors were not statistically significant reasons for a detached retina.
Discussion
In our study it was found that the number of Paediatric RD is more common in male children. However this could be because of the fact that closed globe injuries form the second largest cause of RD in our study . Macula off RD was seen in most patients(93.5%) This could be because of the fact that children with RD with macula on do not have visual complaints or are unable to explain the visual symptoms if any. Idiopathic (38.7%), Closed globe injury(25.8%)&myopia(22.6%)were the top 3 commonest causes. A large number of patients had RD after closed globe injury (25.8%)compared to open globe injury(10.8%) In Idiopathic cases , trauma could be a cause as children usually do not come up with a history of blunt trauma until skillfully elicited or observed . 46.2% had no PVR,33.3% grade C PVR with subretinal type(26.9%) being the commonest. There was no significant association between PVR grade and re-attachment in our study .although 50% of subjects with Grade 4 PVR did not have re-attachment ,while only 9.7% of Grade 3 and 20% of Grade 1 did not have reattachment. Although subjects with Lower PVR grade had better visual outcomes, it was not found to be statistically significant. Probably this could be due to the fact that majority of the RD s were macula- off at presentation, which is a known prognostic indicator of visual recovery post RD surgery,[[i],[ii]]
Re-attachment was seen in 80.6% eyes . Highest percentage of reattachment was seen among subjects with Idiopathic causes (44.4%) followed by Closed Globe injury(22%) .Least re-attachment was seen in Open globe injury (5.6%). In the study there was no significant association between Number of Resurgeries and Visual outcomes. Majority had poor visual outcomes with vision of PL to 1/60 in 41.9%.Interestingly , 84.9% of the patients did not end up with Phthisis Bulbi, despite the fact that a significant number of patients had RD post- trauma. In our study ,it has been seen that among subjects with poor retinal re-attachment,33.3% of subjects had undergone Inferior retinectomy which was done for anterior PVR .
The incidence of retinal detachment from all causes in many studies was found to be similar between males and females,[[iii] [iv] [v] [vi] [vii]]. In our study , males were found to be predominantly affected and this could be because of the fact that closed globe injuries form the second largest cause of RD in our study . A large number of patients had RD after closed globe injury (25.8%)compared to open globe injury(10.8%) which is in agreement with other studies,[[viii] [ix] [x] [xi]]. Many reports have listed myopia as one of the most common causes of pediatric RD, and its frequency has ranged from 28% to 42.4%,[[xii] [xiii]].This is in contrast to the findings in our study. Congenital anomaly has been thought to be a major characteristic feature in pediatric RRD. Reported frequency ranged from 17% to 56%.[[xiv]] .This again disagrees with the findings in our study.
One of the important causes of failure in retinal detachment surgery is proliferative vitreo retinopathy(PVR)[[xv]]. Children present late and have increased intra-ocular cellular activity,both of which result in advanced PVR being a common presentation in them. In a study conducted on Indian population by Wadhwa et al, [xii ].44.78% had advanced PVR.Anterior PVR was found to have a poor visual outcomes. There was no significant association between PVR grade and reattachment in our study . Also ,there was no effect of PVR on the visual outcomes. Anterior PVR is known to have poor prognosis,[[xvi]] and retinectomies are done in patients with Anterior PVR . In our study ,it has been seen that among subjects with no reattachment ,33.3% of subjects had undergone Inferior retinectomy done for anterior PVR . This suggests that inferior retinectomy could possibly make no difference in improving outcomes in patients with Anterior PVR which by itself is a poor prognostic factor as per other studies.
In a study conducted by Wang et al,[[xvii]] on paediatric RD in east Asians ,myopia was the most common cause(38%) ,again in contrast to our study.80% of the RD were macula off at presentation which agrees with our study. The anatomic success rate in the patients was 84.5%.In our study , the re-attachment was seen in 80.6% of eyes which agrees with the above study.PVR changes were not correlated with retinal re-attachement in the above study .
In a study conducted by Weinberg et al, Retinal reattachment was achieved in 79% of eyes and poor prognosis were seen in pre operative vision of unmeasurable or light perception (P = 0.0001), macula-off retinal detachment (P = 0.01), the presence of proliferative vitreoretinopathy grade C or worse (P = 0.02).In our study , the incidence of retinal re-attachement is similar and though the reattachment rates were lower with higher grades of PVR , it was not found to be statistically significant.
Conclusions
Paediatric Retinal detachments prove to be challenging right from the time of presentation as most of them tend to present as Macula off detachments which have poor surgical outcomes. Idiopathic causes and Closed globe injury were the leading causes of paediatric rhegmatogenous RD .One limitation is that trauma could be a cause of idiopathic RD as children usually do not give history of trauma unless skillfully elicited. Though the incidence of re-attachment was higher in patients with higher grades of PVR ,it was not found to be statistically significant in our study . The visual outcomes were poor in general . Inferior retinectomy done for anterior PVR was associated to be a statistically significant cause of non re-attachment post RD surgery,which is probably due to the fact that anterior PVR by itself is associated with poor prognosis . More studies are needed to analyse the various outcomes and compare them .
References
[i] David V Weinberg,Alice TLyon,Mark JGreenwald,Marilyn B Mets.Rhegmatogenous retinal detachments in children: Risk factors and surgical outcomes.Ophthalmology.2003,110(9):1708-1713
[iii] Hudson JR. Retinal detachment in children. Trans Ophthalmol Soc UK 1965;85:79–91.
[iv] Tassman W. Retinal detachment in children. Trans Am Acad Ophthalmol Otolaryngol 1967;71:455–460.
[v] Winslow RL, Tassman W. Juvenile rhegmatogenous retinal detachment. Ophthalmology 1978;85:607–618.
[vi] Hilton GF, Norton EWD. Juvenile retinal detachment. Mod Probl Ophthalmol 1969;8:325–341.
[vii] Arensten JJ, Welch RB. Retinal detachment in the young individual: a survey of 100 cases seen at the Wilmer Institute.J Pediatr Ophthalmol 1965;11:198–202
[viii] Stralman E, Elman M, Daub E, Baker S. Causes of pediatric eye
injuries. A population based study. Arch Ophthalmol 1990;108:603-6.
.[ix] Hudson JR. Retinal detachment in children. Trans Ophthalmol Soc UK 1965;85:79-91
[x] . Nagpal M, Nagpal K, Rishi P, Nagpal PN. Juvenile rhegmatogenous retinal detachment. Indian J Ophthalmol 2004;52:297-302.
[xi] Sarrazin L, Averbukh E, Halpert M, Hemo I, Rumelt S. Traumatic pediatric retinal detachment: A comparison between open and closed globe injuries. Am J Ophthalmol 2004;137:1042-9
[xii] Butler TK, Kiel AW, Orr GM. Anatomical and visual outcomes of retinal detachment surgery in children. Br J Ophthalmol .2001;85:1437–9.
[xiii] Fivgas GD, Capone A Jr. Pediatric rhegmatogenous retinal detachment. Retina .2001;21:101-6.
[xiv] Akabane N, Yamamoto S, Tsukahara I, Ishida M, et al. Surgical outcomes in juvenile retinal detachment. Jpn J Ophthalmol 2001;45:409-11.
[xv] Neeraj Wadhwa, Pradeep Venkatesh, Raju ,Sampangi,Satpal Garg. Rhegmatogenous retinal detachments in children in India: Clinical characteristics, risk factors, and surgical outcomes .Journal of AAPOS.2016,12:551-554
[xvi] Diddie KR, Azen SP, Freeman HM, et al. Anterior proliferative vitreoretinopathy in the silicone study. Silicone Study Report Number 10. Ophthalmology .1996;103:1092-9.
[xvii] Nan-Kai Wang, Chen-Hsin Tsai, Yen-Po Chen, Ling Yeung, Wei-Chi Wu, Tun-Lu Chen, Ken-Kuo Lin, Chi-Chun Lai.Pediatric Rhegmatogenous Retinal Detachment in East Asians. Ophthalmology. 2005;112:1891–1896
Table 1 -Cause of R.D
| Count | % | |
| Congenital causes | 14 | 15.1% |
| Open globe injury | 10 | 10.8% |
| Closed Globe injury | 24 | 25.8% |
| Post Endophthalmitis surgery | 4 | 4.3% |
| Post RD surgery | 7 | 7.5% |
| Myopic RD | 21 | 22.6% |
| Marfan’s syndrome | 5 | 5.4% |
| Coloboma | 3 | 3.2% |
| Idiopathic | 36 | 38.7% |
Table 2 -PVR grade and type
| Count | % | ||
| PVR Grade | 0 | 43 | 46.2% |
| A | 5 | 5.4% | |
| B | 4 | 4.3% | |
| C | 31 | 33.3% | |
| D | 10 | 10.8% | |
Table 3– surgical outcomes
| Count | |||
| Post Op Vision | PL to 1/60 | 39 | 41.9% |
| 2/60 to 6/60 | 32 | 34.4% | |
| 6/60 to 6/18 | 22 | 23.7% | |
| Reattachment | No | 18 | 19.4% |
| Yes | 75 | 80.6% | |
| Cornea | Hazy cornea/ BSK | 9 | 9.7% |
| Clear cornea | 84 | 90.3% | |
| Intra ocular lens | 14 | 15.1% | |
| Phthisis Bulbi | 5 | 5.4% | |
| Trabeculectomy done for glaucoma | 4 | 4.3% | |
Table 4 -Effect of grade of PVR on Retinal reattachment
| PVR Grade | |||||||||||
| 0 | A | B | C | D | |||||||
| Count | % | Count | % | Count | % | Count | % | Count | % | ||
| Reattachment | No | 9 | 20.9% | 1 | 20.0% | 0 | 0.0% | 3 | 9.7% | 5 | 50.0% |
| Yes | 34 | 79.1% | 4 | 80.0% | 4 | 100.0% | 28 | 90.3% | 5 | 50.0% | |
χ 2 = 8.906, df = 4, p = 0.063
Table 5– Reasons for detached retina post RD surgery
| Re-attachment
present |
P Value | |||
| Count | % | |||
| Open Globe injury
|
9 | 12.0% | 0.428 | |
| Closed globe injury | 20 | 26.7% | 0.699 | |
| Number of Resurgery | 0 | 48 | 64.0% | 0.818 |
| 1 | 18 | 24.0% | ||
| 2 | 8 | 10.7% | ||
| 3 | 1 | 1.3% | ||
| Nasal retinectomy | 8 | 10.7% | 0.510 | |
| Temporal retinectomy | 7 | 9.3% | 0.608 | |
| Inferior retinectomy | 8 | 10.7% | 0.016* | |
| Superior retinectomy | 4 | 5.3% | 0.317 | |
| PVR Grade | 0 | 34 | 45.3% | 0.063 |
| 1 | 4 | 5.3% | ||
| 2 | 4 | 5.3% | ||
| 3 | 28 | 37.3% | ||
| 4 | 5 | 6.7% | ||
Effect of cause of retinal detachment on retinal re-attachment (Graph 1)
[1] David V Weinberg,Alice TLyon,Mark JGreenwald,Marilyn B Mets.Rhegmatogenous retinal detachments in children: Risk factors and surgical outcomes.Ophthalmology.2003,110(9):1708-1713
[1] Hudson JR. Retinal detachment in children. Trans Ophthalmol Soc UK 1965;85:79–91.
[1] Tassman W. Retinal detachment in children. Trans Am Acad Ophthalmol Otolaryngol 1967;71:455–460.
[1] Winslow RL, Tassman W. Juvenile rhegmatogenous retinal detachment. Ophthalmology 1978;85:607–618.
[1] Hilton GF, Norton EWD. Juvenile retinal detachment. Mod Probl Ophthalmol 1969;8:325–341.
[1] Arensten JJ, Welch RB. Retinal detachment in the young individual: a survey of 100 cases seen at the Wilmer Institute.J Pediatr Ophthalmol 1965;11:198–202
[1] Stralman E, Elman M, Daub E, Baker S. Causes of pediatric eye
injuries. A population based study. Arch Ophthalmol 1990;108:603-6.
.[1] Hudson JR. Retinal detachment in children. Trans Ophthalmol Soc UK 1965;85:79-91
[1] . Nagpal M, Nagpal K, Rishi P, Nagpal PN. Juvenile rhegmatogenous retinal detachment. Indian J Ophthalmol 2004;52:297-302.
[1] Sarrazin L, Averbukh E, Halpert M, Hemo I, Rumelt S. Traumatic pediatric retinal detachment: A comparison between open and closed globe injuries. Am J Ophthalmol 2004;137:1042-9
[1] Butler TK, Kiel AW, Orr GM. Anatomical and visual outcomes of retinal detachment surgery in children. Br J Ophthalmol .2001;85:1437–9.
[1] Fivgas GD, Capone A Jr. Pediatric rhegmatogenous retinal detachment. Retina .2001;21:101-6.
[1] Akabane N, Yamamoto S, Tsukahara I, Ishida M, et al. Surgical outcomes in juvenile retinal detachment. Jpn J Ophthalmol 2001;45:409-11.
[1] Neeraj Wadhwa, Pradeep Venkatesh, Raju ,Sampangi,Satpal Garg. Rhegmatogenous retinal detachments in children in India: Clinical characteristics, risk factors, and surgical outcomes .Journal of AAPOS.2016,12:551-554
[1] Diddie KR, Azen SP, Freeman HM, et al. Anterior proliferative vitreoretinopathy in the silicone study. Silicone Study Report Number 10. Ophthalmology .1996;103:1092-9.
[1] Nan-Kai Wang, Chen-Hsin Tsai, Yen-Po Chen, Ling Yeung, Wei-Chi Wu, Tun-Lu Chen, Ken-Kuo Lin, Chi-Chun Lai.Pediatric Rhegmatogenous Retinal Detachment in East Asians. Ophthalmology. 2005;112:1891–1896
Table 1 -Cause of R.D
| Count | % | |
| Congenital causes | 14 | 15.1% |
| Open globe injury | 10 | 10.8% |
| Closed Globe injury | 24 | 25.8% |
| Post Endophthalmitis surgery | 4 | 4.3% |
| Post RD surgery | 7 | 7.5% |
| Myopic RD | 21 | 22.6% |
| Marfan’s syndrome | 5 | 5.4% |
| Coloboma | 3 | 3.2% |
| Idiopathic | 36 | 38.7% |
Table 2 -PVR grade and type
| Count | % | ||
| PVR Grade | 0 | 43 | 46.2% |
| A | 5 | 5.4% | |
| B | 4 | 4.3% | |
| C | 31 | 33.3% | |
| D | 10 | 10.8% | |
Table 3– surgical outcomes
| Count | |||
| Post Op Vision | PL to 1/60 | 39 | 41.9% |
| 2/60 to 6/60 | 32 | 34.4% | |
| 6/60 to 6/18 | 22 | 23.7% | |
| Reattachment | No | 18 | 19.4% |
| Yes | 75 | 80.6% | |
| Cornea | Hazy cornea/ BSK | 9 | 9.7% |
| Clear cornea | 84 | 90.3% | |
| Intra ocular lens | 14 | 15.1% | |
| Phthisis Bulbi | 5 | 5.4% | |
| Trabeculectomy done for glaucoma | 4 | 4.3% | |
Table 4 -Effect of grade of PVR on Retinal reattachment
| PVR Grade | |||||||||||
| 0 | A | B | C | D | |||||||
| Count | % | Count | % | Count | % | Count | % | Count | % | ||
| Reattachment | No | 9 | 20.9% | 1 | 20.0% | 0 | 0.0% | 3 | 9.7% | 5 | 50.0% |
| Yes | 34 | 79.1% | 4 | 80.0% | 4 | 100.0% | 28 | 90.3% | 5 | 50.0% | |
χ 2 = 8.906, df = 4, p = 0.063
Table 5– Reasons for detached retina post RD surgery
| Re-attachment
present |
P Value | |||
| Count | % | |||
| Open Globe injury
|
9 | 12.0% | 0.428 | |
| Closed globe injury | 20 | 26.7% | 0.699 | |
| Number of Resurgery | 0 | 48 | 64.0% | 0.818 |
| 1 | 18 | 24.0% | ||
| 2 | 8 | 10.7% | ||
| 3 | 1 | 1.3% | ||
| Nasal retinectomy | 8 | 10.7% | 0.510 | |
| Temporal retinectomy | 7 | 9.3% | 0.608 | |
| Inferior retinectomy | 8 | 10.7% | 0.016* | |
| Superior retinectomy | 4 | 5.3% | 0.317 | |
| PVR Grade | 0 | 34 | 45.3% | 0.063 |
| 1 | 4 | 5.3% | ||
| 2 | 4 | 5.3% | ||
| 3 | 28 | 37.3% | ||
| 4 | 5 | 6.7% | ||
Effect of cause of retinal detachment on retinal re-attachment (Graph 1)
Leave a Comment