
Dr. Manoj S, M08551, Dr. Sheera K R, Dr. Unnikrishnan Nair R
Abstract
PURPOSE:
To evaluate the 6month and 1year efficacy of modified combination therapy protocol for Polypoidal Choroidal Vasculopathy (PCV).
DESIGN:
Retrospective study
METHODS:
We retrospectively reviewed 25 eyes of 24 patients who were diagnosed as PCV on ICG angiography and received a modified combination treatment strategy; intravitreal Anti VEGF injections initially followed by standard PDT. Mean changes in the best-corrected visual acuity, central retinal thickness between baseline, month 6 and Month 12 and number of additional treatments were analysed and compared with known data on early PDT combination therapy and other relevant studies.
RESULTS:
Mean baseline vision improved from 0.40±0.32 to 0.17±0.21 logMAR units and 0.12±0.19 logMAR units respectively at 6months and 12 months post PDT.Mean visual acuity gain was 0.24±0.27 logMAR units and 0.28±o.28 logMAR units at 6months an 12 months respectively. The Mean CFTimproved from346.64±130.67µ to 196.68±52.98µ and 191.52±41.47µ at 6 months and 12 months post PDT respectively . Mean CFT gain was 149.96±140.01µ and 155.12±133.43µ at 6months and 12 months respectively.Mean number of injections required to dry the fovea before PDT were 2.05. Mean number of additional injections required was 0.6 and 0.71 at 6months and 1year respectively.Out of 25 eyes 40% required additional antiVEGF treatment with ranibizumab injection at 6 months and 48% at the end of one year. Number of patients requiring additional PDT was 0% at 6months and 4% at 1 year.
CONCLUSION:
Deferred PDT combined with antiVEGF therapy in PCV eyes shows good visual and anatomical improvements at 6 months and 12 months. Delayed PDT combination leads to significantly fewer additional treatments and less complications.
Modified Combination Therapy Strategy For Polypoidal Choroidal Vasculopathy.
AIM OF THE STUDY: To evaluate the 6months and 1year efficacy of modifiedcombination therapy protocol for Polypoidalchoroidalvasculopathy (PCV).
MATERIALS AND METHODS:
We retrospectively reviewed data of 25 eyes of 24 patients who were diagnosed asPCV on Indocyanine green angiography(ICG) and underwent modified combination treatment protocol. Modified combination therapy protocol is defined as those patients who received anti vascular endothelial growth factor(anti VEGF) therapy initially and followed by PDT at a later date . Our study included both treatment naïve and previously treated patient. The latter group had a minimum gap of 6 months from the previous treatment,which was IntravitrealRanibizumab. The inclusion criteria are as follows: (a) confirmed diagnosis of PCV, that is, presence of early subretinal focal ICGA hyperfluorescence (appearing within the first 6 minutes after injection of indocyanine green) and in addition, at least one of the following angiographic or clinical criteria: (i) association with a BVN, (ii) presence of pulsatile polyp, (iii) nodular appearance when viewed stereoscopically, (iv) presence of hypofluorescent halo (in first 6 minutes), (v) orange subretinal nodules in stereoscopic color fundus photograph (polyp corresponding to ICGA lesions), or (vi) associationwith subretinal hemorrhage or exudation (b) follow up period should be greater than or equal to 1 year. Patients were excluded if there were other intraocular conditions like cataract, glaucoma or any other condition affecting vision. Patients who have not completed the mandatory atleast 9 visits out of the 12 visits were also excluded from the study. Eyes that underwent the EVEREST guidelines of primary combination therapy and where the diagnosis was not clear were also not analysed in this study.
Treatment protocol of our study– After the diagnosis of PCV, patients wereinitially given intravitrealranibizumab injections at monthly intervals until the fovea was dry of fluid. Dry fovea was defined as absence or decrease of subretinal fluid(SRF) to less than 100 microns at the fovea.Presence of cystoid macular edema(CME) persisting in the absence of SRF was not considered as active, provided there was no increase in CME compared to the last visit. These eyes were followed by combination therapy of standard fluencePDT and intravitrealRanibizumab. Standard PDT was given as intravenous injection of verteporfin6 mg/m2 with laser irradiation at 689-nm wave length and 600 mW/cm2 irradiance for 83 seconds. 24 hrs later intravitrealRanibizumab was given in the same eye. Best corrected visual acuity(BCVA) and Central foveal thickness(CFT) were measured at baseline and at each follow-up visit. FA/ICG angiography was done at 3 monthly intervals if poor responder to treatment. BCVA was measured using Snellen’s visual acuity chart and converted to logMAR and ETDRS letters for convenience purpose. Conversion to ETDRS letters was done using formula 85+50×log(snellen fraction) as defined by Gregori NZet al (1).Patients were retreated with intravitrealRanibizumab injections on pro re natabasis. Retreatment criteria are (1) decrease in visual acuity by one line on snellen’schart (2) presence of subretinal fluid on OCT (3)appearance of new subretinal hemorrhage or exudation close to fovea.Retreatment with PDT was done only if the disease is persistantwith no response to additional anti-VEGF therapy and is based on the presence of active polyp or Branching Vascular Networkon ICG withsubretinal fluid.
STATISTICAL ANALYSIS:
The aim of this study is to calculate differences in the change in BCVA and CFT at 6months and 12 months in patients who underwent the treatment protocol.Data analysis was performed using SPSS version 17.0. Quantitative variables were expressed in mean and standard deviation. Qualitative variables were expressed in frequency distribution. Group comparison of quantitative variables wereanalysed using independent sample t-test and that of qualitative variables were analysed using Chi- square test.Receiver operating characteristic (ROC) curve was plotted to find the optimum cut off point of the independent variable to predict the best outcome and the Area Under Curve(AUC) with 95% CI was calculated. A’p’ value of 0.05 or less was taken as significant.
RESULTS:
A total of 25 eyes of 24 patients were included in the study. Baseline characteristics of the patients are shown below.
Table 1. Baseline features of the study population
| BASELINE FEATURES | |
| Eyes | 25 |
| Age | 70.29±5.89 |
| Sex | M- 11 (44%)
F- 14 (56%) |
| Visual acuity
-LOGMAR -ETDRS |
0.40±0.32 64.9±16.1 letters |
| Central foveal thickness(µm) | 346.6±130.67 µm |
Changes in BCVA
The mean visual acuities at Baseline, Month 6and Month 12 were 0.40 ± 0.32, 0.17 ± 0.21 and 0.12±0.19 LogMARrespectively. The mean ETDRS letter scores at baseline, Month 6 and Month 12 were 64.9 ± 16.1, 76.7±10.8 and 79.0±9.8 respectively. BCVA level improvement was significant from baseline to 6month&12month and also maintained through month 6 to month 12.
Table 2: Changes In Visual Acuity In ETDRS Letters
Conversion formula = 85+50 × log (snellen fraction)
|
N |
Visual acuity in ETDRS | Paired comparison | Paired Differences | Paired t test | ||||
| mean | sd | Mean | sd | t | p | |||
| Baseline | 25 | 64.91 | 16.11 | Baseline to 6 months | 11.75 | 13.68 | 4.296 | <0.001 |
| After 6 months | 25 | 76.66 | 10.75 | 6 months to last follow up | 2.34 | 3.25 | 3.610 | .001 |
| At last follow-up | 25 | 79.01 | 9.78 | Baseline to last follow up | 14.10 | 14.09 | 5.004 | <0.001 |
Changes in Central Foveal Thickness:
The mean central foveal thickness (CFT) was 346.64±130.67,196.68±52.98 and 191.52±41.47 microns respectively at Baseline, Month 6 and Month 12 .CFT decreased significantly at Month 6 and maintained through Month12.However even though there was numerically an improvement between 6 months and 12 months, it was not statistically significant.
Table 3: Changes in the CFT
|
N |
CFT | Paired comparison | Paired Differences | Paired t test | ||||
| mean | sd | Mean | sd | t | p | |||
| Baseline | 25 | 346.64 | 130.67 | Baseline VS 6 months | 149.96 | 140.01 | 5.355 | <0.001 |
| After 6 months | 25 | 196.68 | 52.98 | 6 months VS last follow up | 5.16 | 34.34 | .751 | .460 |
| At last followup | 25 | 191.52 | 41.47 | Baseline VS last follow up | 155.12 | 133.43 | 5.813 | <0.001 |
ADDITIONAL TREATMENTS:
The average number of injections received before PDT was 2.12. The Average timing of PDT was 4.64 months. This means that it takes on an average of 4-5 months for the fovea to be reasonably dry before PDT is done. Out of 25 eyes 40% required additional anti-VEGFtreatment with ranibizumab injection at 6 months and 48% at the end of one year.Only one patient(4%) required additional PDT retreatment at the end of one year. Mean number of retreatment with anti VEGF injections at Month 6 and Month 12 are 0.6 and 0.71 respectively after PDT session.
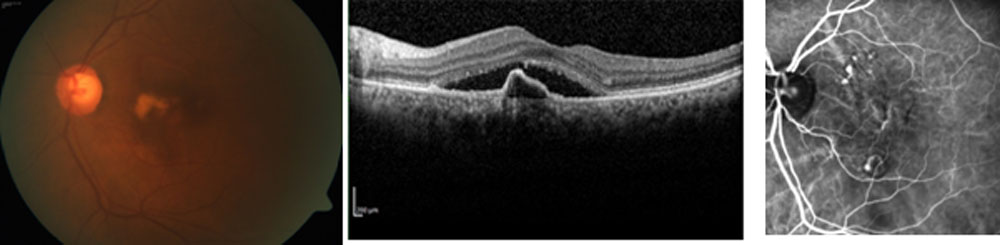
Image 1: Baseline fundus picture, OCT and ICG.
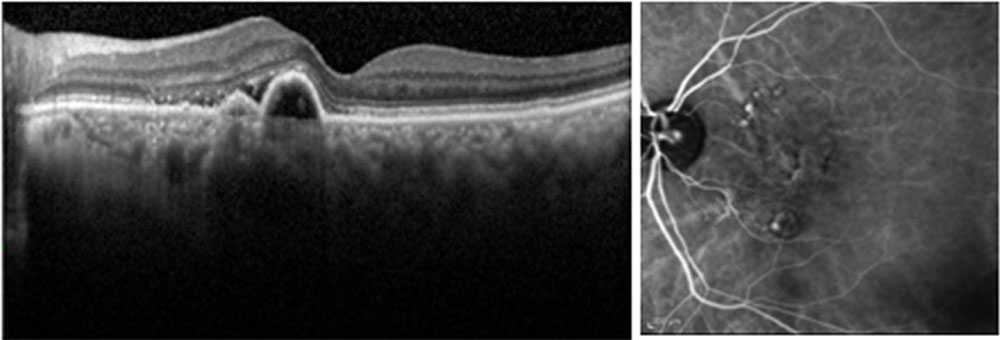
Image 2: OCT and ICG after Anti-VEGF injections
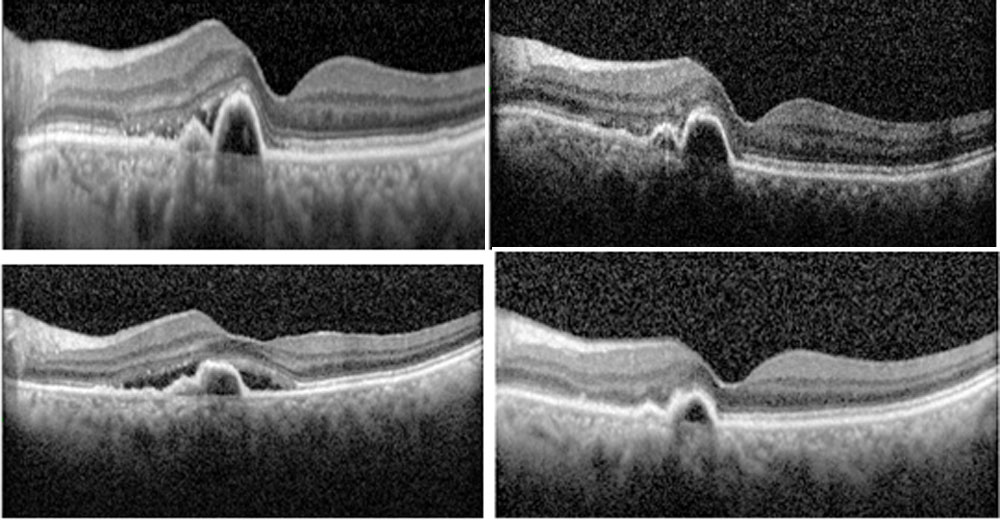
Image 3: Post PDT pictures
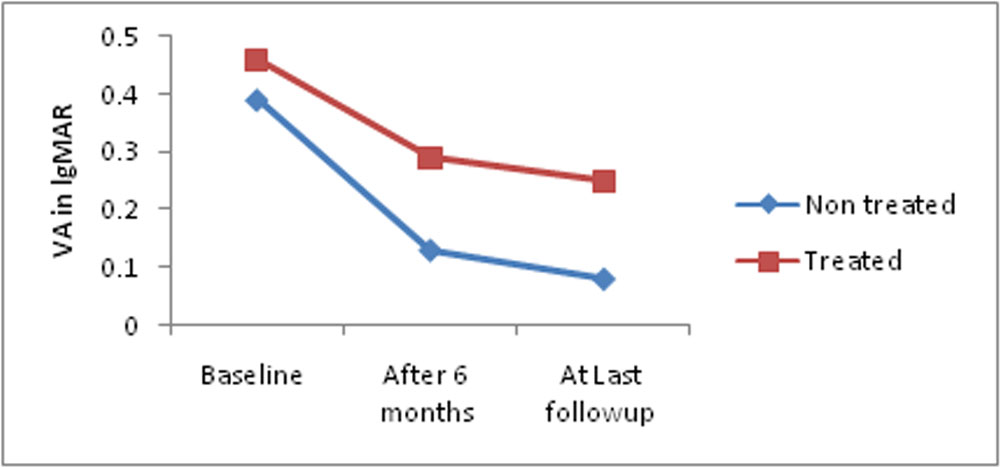
We have also analysedthe differences in outcome between treatment naïve and previously treated patients.There are no significant differences between treatment groups suggesting that previous anti VEGF therapy did not have any added benefit nor it is detrimental towards a poor outcome. Curiously the previous treated group had a poorer baseline vision and poorer outcome at 6 months and 12 months compared to treatment naïve eyes though not statistically significant.
Figure 1:Differences In Mean Visual Acuity Between Treatment Naïve And Treated Groups:
DIFFERENCES IN MEAN CFT BETWEEN TREATMENT NAÏVE AND TREATED GROUPS:
The mean CFT at baseline, 6months and last follow-up are 363.42µ, 191.74µ, 194.11µ respectively in the treatment naïve group and it is 293.50µ, 212.33µ, 183.33µ respectively in the previously treated group. Mean CFT gain from baseline to 6 months is 171.68±130.40µ and 81.17±159.39µ between treatment naïve and previously treated groups respectively.CFT gain from baseline to last follow-up is 169.32±124.56µ and 110.17±162.51µ in treatment naïve and previously treated groups respectively .Though statistically not significant, mean CFT gains were better in the treatment naïve group.
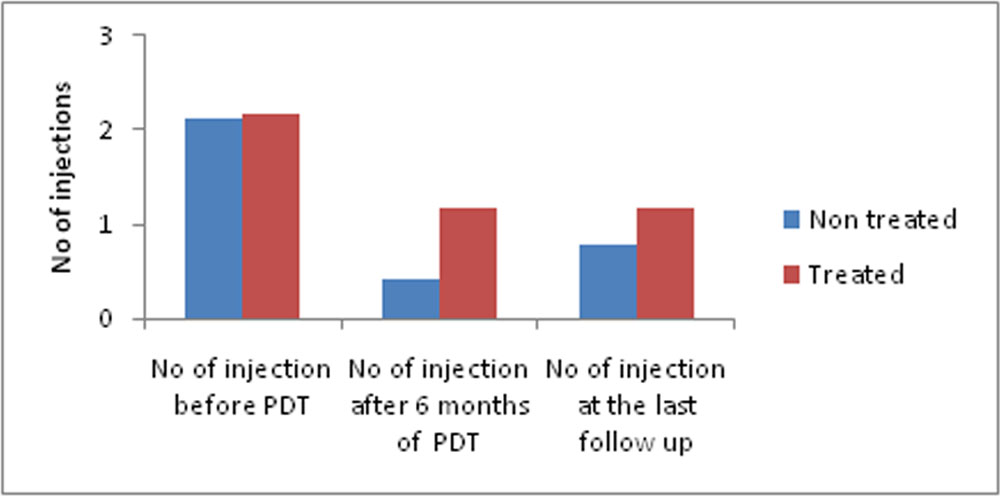
DIFFERENCES IN THE NUMBER OF INJECTIONS BETWEEN TREATMENT NAÏVE AND TREATED GROUPS:
There is no significant difference in the number of injections required to dry the fovea before PDT between the two groups. But the number of injections required post PDT is slightly higher in the previously treated group.
Figure 2: Differences In The Number Of Injections Between Treatment Naïve And Treated Groups
We used Receiver Operating Characteristic (ROC) curve and Chi square test for determining optimumcutoff point for predicting good functionaland anatomical outcome values.
A Base line log MAR visual acuity of <0.57(approximately corresponding to 6/24)was associated with a sensitivity of 94.7 % , aspecificity of 83.3 % , and an area under an ROC curve (AUROC) of 0.807with 95% CI 0.527 – 1.000 fordetermining good outcome at the last follow up (p<0.001). It means if the visual acuity value is better than 6/24 at baseline, there is a significant chance of obtaining good vision at the last follow-up.
Table 5 : Baseline Visual Acuity As Predictor For Good Visual Outcome
| Baseline visual acuity(logMAR) | Outcome | Total | χ2 | Df | p | ||||
| Good | Poor | ||||||||
| N | % | N | % | N | % | ||||
| <0.57 | 18 | 94.7 | 1 | 16.7 | 19 | 76.0 | 15.237
|
1
|
<0.001
|
| >0.57 | 1 | 5.3 | 5 | 83.3 | 6 | 24.0 | |||
| Total | 19 | 100.0 | 6 | 100.0 | 25 | 100.0 | |||
When Baseline visual acuity used as a predictor for determining optimum anatomical outcome(CFT) at the last follow-up, the ‘p’ value was not significant. Baseline Visual acuity of <0 .45 logMAR was associated with a sensitivity of 53.8 % , a specificity of 41.7% , and an area under ROC curve (AUROC) of only 0.558 with 95% CI 0.314 – 0.801 for determining CFT <184 at the last follow up. (p=0.821)
Similarly baseline CFTwhen used to predict the optimum anatomical and functional outcomes, ‘p’ values were not significant. A Baseline CFT of < 439µ was associated with a sensitivity of 84.2 % , aspecificity of 50.0 % , and an area under an ROC curve (AUROC) of only 0.544with 95% CI 0.225 – 0.863 for determining good anatomical outcome at the last follow up(p=0.087). A Baseline CFT< 340µ is associated with a sensitivity of 53.8 %,specificity of 50.0 % , and an Area under ROC curve of only 0.510with 95% CI 0.273 – 0.746 for determining goodvisual outcome at the last follow up(p=0.848). So baseline CFT in the present study cannot be used to predict visual and anatomical outcomes.
ADVERSE EFFECTS:In our study 2 patients(8%) had RPE rip and one patient amongst them developed mild vitreous hemorrhage. No systemic adverse effects have been noted.
DISCUSSION:
The term “idiopathic polypoidalchoroidalvasculopathy” (IPCV) was coined by Yannuzzi et al to describe a disease of the choroidal circulation characterized by branching choroidal vessels with polyp-like terminal aneurysmal dilations, and recognized as a clinical entity separate from age-related macular degeneration(2).. PCV is defined as the presence of single or multiple focal areas of hyperfluorescence arising from the choroidal circulation within the first 6 minutes after injection of indocyanine green, with or without an associated branching vascular network (BVN)(3). The presence of orange-red subretinal nodules with corresponding ICG hyperfluorescence is pathognomonic of PCV. Identification of a BVN is not an absolute requirementfor a diagnosis of PCV especially those with small lesions of shortduration, in whom this feature is not demonstrated.
Photodynamic therapy resolves polypoidal lesions with subsequent resolution of accompanying fluid, whereas anti-VEGF agents rapidly absorb fluid and improve vision(4-6). Photodynamic therapy-monotherapy causes subretinal hemorrhage, pigment epithelial tear, atrophy of retinal pigment epithelium, and choriocapillaris in the exposure area in addition to a possible VEGF surge, and those may cause the limited visual improvement after PDT(5,6). Many studies reported the effectivenessof anti-VEGF therapy alone for treating PCV on the BCVA basis(7,9), but has less ability to resolve the polypoidal lesions, which leads to early recurrence of fluid(4,8).Thus, combining verteporfin with its angioocclusive effects and ranibizumab with its antiangiogenic and antipermeability effects may lead to synergistic treatment effects in PCV.
EVEREST study(10) assessed the effects of PDT combined with ranibizumab or alone versus ranibizumabmonotherapy in patients with symptomatic macular PCV.Combination therapy involved PDT initially along with intravitreal ranibizumab within 24hours of PDT followed by two consecutive monthly ranibizumab injections. Thereafter injections were given on pro re nata (PRN) basis.PDT combined with ranibizumab 0.5 mg or alone was superior to ranibizumabmonotherapy in achieving complete regression of polyps in this 6-month study in patients with symptomatic macular PCV.
In this present study our aim was to give the intravitreal injections initially till the fovea is dry followed by PDT. Retreatment with injections were done on PRN basis.When we compared our 6months data with EVEREST data,mean age is slightly higher and there is female preponderance in this study. Mean visual acuity and mean CFT are comparable in the studies . Average number of retreatments are less in present study.
Table 6: Comparison Table Between Our Study And EVEREST Study
| EVEREST STUDY (COMBINATION THERAPY GROUP) N=19 | PRESENT STUDY (6 MONTH DATA)
N= 25 |
|
| AGE | 63.8±8.30 | 70.25 |
| SEX | M- 11 (57.9)
F -8 (42.1) |
M- 11 (44)
F- 14 (56) |
| BCVA
(mean no. of letters gain in ETDRS chart) |
10.9±10.9 letters
|
11.75±13.68
|
| Mean decrease in CRT(µ) | 145.6±119.0 | 149.96±140.01 |
| PDT month | 0 | 4.64 |
| Average Retreatment injections number | 1.1
|
0.6 |
| No. of patients retreated with injections | 55.6% | 40% |
| No. of patients retreated with PDT | 44.4% | 4% |
| Ocular adverse effects | 26.3% | 8% |
| Non ocular adverse effects | 31.6% | 0% |
FUJISAN study(11) compared the 1-year results of initial or deferred photodynamic therapy combined with intravitreal ranibizumab for eyes with polypoidal choroidal vasculopathy. Both initial and deferred PDT combined with IVR to treat polypoidal choroidal vasculopathy show the similar visual and anatomical improvements at 12months.Delayed PDT group received intravitreal ranibizumab injections once monthy for 3 consecutive months followed by PDT. Retreatment was given with injections or PDT according to the disease activity. Mean visual acuity improvement, mean CFT gain are slightly higher and additional number of retreatments required are also less in the present study when compared to Fujisan study.
Table 7: Comparison Table Between Our Study And FUJISAN Study (Delayed PDT Group)
| FUJISAN STUDY (N=35) | PRESENT STUDY(1year) (N=25) | |
| AGE | 73.8 | 70.25 |
| MEAN IMPROVEMENT IN VISUAL ACUITY | 0.22logMAR
|
0.28±0.28 logMAR
|
| Mean CFT gain (µ) | 145.6±20.6 | 155.12±133.43 |
| Percentage of patients receiving additional treatments(Inj+PDT) | 82.9%
|
48%
|
| No. of injections after month3 | 3.8±2.3 | 1 |
| No. of patients who received additional PDT | 40%
|
4%
|
| Adverse events | 2.8% | 0% |
Combination therapy of PDT and anti-VEGF drugs provides the complementary effects of both treatments, but it remains unknown whether PDT should have been administered at the beginning of treatment or during follow-up of anti-VEGF therapy. From our study, we observed that drying the fovea before PDT will give better anatomical and visual outcomes.The number of additional retreatments required were also less. Small sample size and being a retrospective study are the major limitationsof this study.
CONCLUSION:Deferred PDT combined with antiVEGF therapy in PCV eyes show good visual and anatomical improvements at 12 months. Delayed PDT combination leads to significantly fewer additional treatments and less complications.
REFERENCES
1)Gregori NZ1, Feuer W, Rosenfeld PJ. Novel method for analyzing snellen visual acuity
measurements.Retina. 2010Jul-Aug;30(7):1046-50. doi: 10.1097/IAE.0b013e3181d87e04.
2)Yannuzzi LA, Sorenson J, Spaide RF, et al. Idiopathic polypoidalchoroidalvasculopathy (IPCV) Retina.1990;10:1–8.
3)Koh AH et al, Expert PCV panel Polypoidalchoroidalvasculopathy: evidence-based guidelines for clinical diagnosis andtreatment.
4)) Lai TY, Chan WM, Liu DT, et al. Intravitreal bevacizumab(Avastin) with or withoutphotodynamic therapy for the treatmentof polypoidal choroidal vasculopathy. Br JOphthalmol2008;92:661–666.
5)Gomi F, Tano Y. Polypoidalchoroidalvasculopathy and treatments.CurrOpinOphthalmol2008;19:208–212.
6) Nowak-Sliwinska P, van den Bergh H, Sickenberg M, Koh AH.Photodynamic therapy for polypoidalchoroidalvasculopathy. ProgRetin EyeRes 2013;37:182–199.
7) Mori R, Yuzawa M, Akaza E, Haruyama M. Treatment resultsat 1 year of ranibizumab therapy for polypoidalchoroidalvasculopathyin eyes with good visual acuity. Jpn J Ophthalmol2013;57:365–371.
8) Sakai T et al. Three-year visual outcomes of intravitreal ranibizumab with or withoutphotodynamic therapy for polypoidalchoroidalvasculopathy.ActaOphthalmol. 2016 May doi: 10.1111/aos.13130
9) Kang HM, Koh HJ. Long-term visual outcome and prognostic factors after intravitrealranibizumab injections for polypoidalchoroidalvasculopathy. Am J Ophthalmol2013;156:652–660.
10) Koh A et al. EVEREST study: efficacy and safety of verteporfin photodynamic therapy incombination with ranibizumab or alone versus ranibizumabmonotherapy in patients with symptomatic macular polypoidalchoroidalvasculopathy.Retina. 2012 Sep;32(8):1453-64.
11)Fumigomi, md, phd, Yuji oshima md etal. Initial versus delayedPhotodynamic therapyin combination with ranibizumabFor treatment of polypoidalchoroidalvasculopathy The Fujisan studyRETINA 0:1–8, 2015.
Leave a Comment