
Dr. Suchismita Satpathy, S20256, Dr. Diptimayee Nayak, Dr. Nikita Dash, Dr. Sumita Mohapatra
INTRODUCTION:
Traumatic Optic Neuritis is defined as sudden loss of vision after Road Traffic Accident (will further be cited as RTA throughout the text) without an evidence of any external eye injury or ophthalmoscopic examination. Optic nerve is vulnerable to trauma in either way whether direct or indirect concussive force which causes functional impairment. Trauma affecting head or orbital region causes insult to optic nerve. There are two types of optic nerve injury, Direct and Indirect. Direct injuries occur by penetrating trauma like mid-facial fracture or orbital fracture. The types of direct injury to optic nerve are, Optic nerve avulsion, Optic nerve transection, Optic nerve sheath haemorrhage, Orbital haemorrhage, and Orbital emphysema.
Indirect optic nerve injuries are more common. The force impacted on head or orbital region may transmit to optic nerve. Hippocrates had known this condition that blow to forehead or eyebrow causes vision loss. Optic nerve involvement on close head injuries ranges from 0.5% to 5%. The site of impact that cause vision loss is forehead greater than supraorbital ridge is greater than temporal region.
Ocular examination is initially normal with a few exception of relative or absolute afferent pupillary defect. A wide range of visual field impairment and optic atrophy may develop in future.
Optic nerve avulsion:
Vision loss is severe and immediate. On fundoscopy, no optic disc is seen, ring haemorrhage is seen. Nerve tear at lamina cribrosa that is evident by Ultrasonography and that occurs due to rotation of eyeball or due to raised intraocular pressure. Treatment is not possible.
Optic nerve transection:
It occurs due to orbital fractures. Vision deteriorates upto no light perception. Radiological imaging may show bony fragments. Treatment is not effective.
Optic nerve sheath haemorrhage:
It is difficult to diagnose but vision loss is reversible.
Orbital haemorrhage:
It may be diffused or localized to orbit. Ophthalmoplegia and Proptosis may be found at the time of presentation. By raising the head end of the patient or giving tablet Diamox can be helpful the intraocular pressure.
AIM:
To study the factors that hamper the visual outcome in traumatic optic neuritis.
MATERIALS AND METHODS:
It is a prospective study including 20 patients having traumatic optic neuritis following RTA and admitted to Regional Institute of Ophthalmology, SCB MEDICAL COLLEGE CUTTACK, between June 2016 to April 2017. Among the total patients, 12 were from urban areas and 8 were from rural areas. Their age group was between 27 years to 43 years. During history taking it was found that 11 patients were bike riders, 2 were car drivers, 3 were bi-cycle riders, 4 were by-standers. Most of the patients were healthy. Few patients had some systemic illness were excluded from this study. After detail history the signs and symptoms were evaluated and the patients those were fit according to the inclusion criteria were subjected to further examinations such as Visual Acuity recorded by Snellen’s Chart taken initially, then after 48 hours of steroid therapy and finally at the last follow-up. Then swinging flash light test was done to know the presence of Relative Afferent Pupillary Defect (RAPD). Intraocular Pressure (IOP) was recorded. Fundoscopic examination was done through Direct Ophthalmoscope and Indirect Ophthalmoscope. Finally, all the patients were sent for CT scan and MRI to know the extent of injury. Patients were treated with Intravenous Methyl Prednisolone 30 mg/kg bodyweight as loading dose, then 5mg/kg bodyweight for the next 48 hours and then with tapering dose of oral steroid.
RESULT:
Out of 22 eyes of 20 patients, most of the eyes had poor vision at the time of presentation in a range of Hand movement to Perception of light. Periorbital edema was present in case of 15 patients due to blunt trauma or orbital fracture. 12 patients had subconjunctival haemorrhage, 8 patients had RAPD, 4 patients had orbital fracture, 8 patients shown optic nerve compression on CT scan or MRI. One group of patients were managed with Intravenous Methylpredisolone 30 mg/kg bodyweight loading dose then 5 mg/kg bodyweight for next 48 hours followed by tapering oral steroids(40mg 10mg).
Second group of patients were managed conservatively due to some reasons like severe head injuries, uncontrolled diabetes mellitus. Patients treated with Intravenous steroids followed by tapering dose of oral steroids had a better outcome in absence of any orbital fracture or RAPD or with periorbital edema.
ANALYTICAL TABLE:
| VISION | SIGNS AND SYMPTOMS | NUMBER OF PATIENTS |
| NO PERCEPTION OF LIGHT | PERIORBITAL EDEMA , RAPD,
ORBITAL FRACTURE |
3 |
| PERCEPTION OF LIGHT | PERIORBITAL EDEMA
ORBITAL FRACTURE |
3 |
| HAND MOVEMENT | MILDSUBCONJUNCTIVAL HAEMORRHAGE,
RAPD |
2 |
| CF-6/60 | MILD PERIORBITAL EDEMA,
SUBCONJUNCTIVAL HAEMORRHAGE
|
5 |
| 6/60 -6/18 | MILD PERIORBITAL EDEMA,
SUBCONJUNCTIVAL HAEMORRHAGE |
3 |
| 6/18 OR BETTER | 4 |
COLUMN CHART:
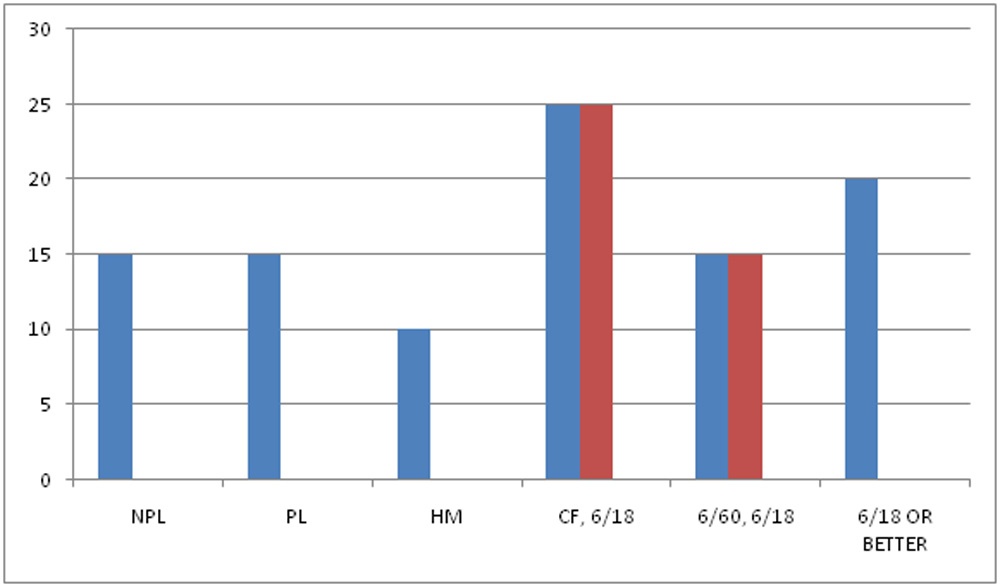
![]() VISION AT PRESENTATION
VISION AT PRESENTATION
![]() FINAL VISUAL OUTCOME
FINAL VISUAL OUTCOME
X-AXIS : VISION Y-AXIS: PERCENTAGE
Abbreviations :
NPL: NO PERCEPTION OF LIGHT PL: PERCEPTION OF LIGHT HM: HAND MOVEMENT
CF: COUNTING FINGER
DISCUSSION:
Traumatic optic neuropathy can cause optic nerve morbidity such as loss of vision, deficits in visual field, colour perception and an afferent pupillary defect. The diagnostic features of traumatic optic neuropathy are visual loss that occurs in the presence of a relative afferent pupillary defect without evidence of injury to the optic nerve or eye. The commonest site of indirect optic nerve injury is the optic canal. Chou had proposed that the damage of optic nerve at microscopic level, including contusion necrosis, nerve fibre tears and nerve infarction secondary to closed space edema, hemorrhage, thrombosis, vasospasm, impingement by bone spicules. All our patients with traumatic optic neuropathy were young male, mostly at age 27 to 43 years old which is consistent with other studies. Motor vehicle accidents were the main cause of traumatic optic neuropathy in our study, while blunt trauma had the second highest incidence rate and followed by fall. Similar findings were showed in Sadeghi-Tari study. We followed up the patients between 6 months to 3 years and all the patients reached the final vision at 6 months’ duration of follow-up as similar in other studies. In the present study, the morbidity associated with traumatic optic neuropathy was decreased visual acuity and relative afferent pupillary defect, which was elicited by swinging flashlight test. The ocular manifestations most commonly associated with optic nerve injury were periorbital hematoma and subconjunctival hemorrhage, with no immediate changes in the optic nerve. The ocular manifestations that were observed in our study are consistent with other studies. Most of the eyes with traumatic optic neuropathy were associated with periorbital hematoma and orbital walls and/or skull fractures. All patients with NPL had periorbital hematoma with subconjunctival hemorrhage.
NPL eyes were associated with orbital walls and skull fractures. These signs may indicate the increased morbidity to the optic nerve and strong relation to traumatic optic neuropathy in cases with or without evidence of optic nerve impingement or compression.
. The International Optic Nerve Trauma Study, which was undertaken to formulate an optimal management protocol, failed because of the limited number of eligible patients. The majority of published data do not clearly define the criteria of visual improvement; some studies defined improvement as an increase in 1 to 3 lines in visual acuity. Methylpredisolone therapy was advocated as the initial treatment of choice because of its neuroprotective mechanism. The exact mechanism of corticosteroids in reducing optic nerve injury is still unclear. Steroids may have the neuroprotective effects of decreasing the intraneural or extraneural edema and relieving compression of the nerve fibres. By reducing vasospasm steroids may also limit contusion necrosis of the nerve and block neuronal death in the setting of trauma is through inhibition of free radicals. The International Optic Nerve Trauma Study reported visual acuity improvement in 52% of patients treated with high dose steroids and 37% of patients treated with mega dose steroids in Sadeghi-Tari study after three months’ follow up. The visual improvement in patients treated with conservative management was not
significant ( =0.386). Those patients treated with intravenous corticosteroids alone showed no visual improvement statistically ( <0.05). There are a few limitations in our study also.
CONCLUSION:
The visual outcome in patients treated with intravenous and oral steroid is better in absence of orbital fracture and Relative Afferent Pupillary Defect.
REFERENCES:
1. Carta A, Ferrigno L, Salvo M, Bianchi-Marzoli S, Boschi A, Carta F. Visual prognosis after indirect traumatic optic neuropathy.2003;74:246-248
2.Kovacic M, Gracner T, Gracner B. Indirect Traumatic Optic Neuropathy-Two Case Reports. 2001;25:57-61
3 .Glaser JS. Traumatic optic neuropathy. In: Glaser L, Glaser JS. Neuro-ophthalmology, 3rd ed. Lippincott Williams and Wilkins 1999:186-188
4 .Beretska JS, Rizzo JF. Controversy in the management of traumatic optic neuropathy. 1994;34:87-96
5 .Liu GT, Volpe NJ, Galetta SL. Neuro-ophthalmology: Diagnosis and Management. Philadelphia: WB Saunders 2001:170-172
6 .Kline LB, Morawetz RB, Swaid NS. Indirect injury of the optic nerve. 1984; 14:756-764
7 .Nazir SA, Westfall CT, Chacko JG, Philips PH, Stack BC Jr. Visual recovery after direct traumatic optic neuropathy. 2010;31:193-194
8 .Kimberly Peele Cockerham. Traumatic optic neuropathy. Ophthalmic Care of the Combat Casualty 2003:395-403
9 .Sadeghi-Tari A, Lashay AR, Tabassi A. Visual outcome of traumatic optic neuropathy in patients treated with intravenous megadose of steroids. 2005;43(2):110-114
10.Li KK, Teknos TN, Lai A, Lauretano AM, Joseph MP. Traumatic optic neuropathy: result in 45 consecutive surgically treated patients. 1999;120(1): 5-11
11 .Steinsapir KD, Goldberg RA. Traumatic optic neuropathy.1994;38:487-518
12 .Chou PI, Sadun AA, Chen YC, Su WY, Lin SZ, Lee CC. Clinical experiences in the management of traumatic optic neuropathy.
Leave a Comment