
Dr. Amita Nair, A20149, Dr. Dubey Nidhi, Dr. Minija C K
Introduction:
Sarcoidosis is a chronic autoimmune multisystemic granulomatous disorder1 and ocular involvement manifests in 25%–60% of sarcoidosis patients.2 The First International Workshop on Ocular Sarcoidosis (FIWOS) recommended four levels of certainty for diagnosis of ocular sarcoidosis.3,4 There has never been a major role of ophthalmological imaging tools in the diagnosis of ocular sarcoidosis.
Studies have analysed OCT (optical coherence tomography)-derived choroidal images in birdshot chorioretinopathy,5 idiopathic panuveitis,6 punctate inner choroidopathy,7,8 and Vogt–Koyanagi–Harada disease (VKH).9
We have use Swept source-OCT(SS-OCT) to quantitatively assess the choroid possibly to understand more about the pathology of ocular sarcoidosis.
Materials and Method:
Data collection:
Clinical and imaging data from patients with granulomatous uveitis were collected retrospectively from patients attending uveitis clinics from September 2016 to May 2017. Approval for data collection and analysis was obtained from the institute’s research and ethics committee and adhered to the tenets set forth in the Declaration of Helsinki.
Patients included in this study had the following assessments: physical examination for features of systemic inflammatory or autoimmune disease; complete ophthalmic examination including best corrected visual acuity (BCVA), disease activity and duration of disease and treatment; a standard laboratory work-up for panuveitis, including full blood count with differential analysis, angiotensin converting enzyme, C-reactive protein, erythrocyte sedimentation rate,liver and kidney function tests, VDRL, and Mantoux test and/or quantiFERON TB-Gold test; chest Xray. Anterior chamber activity was graded by measuring the number of cells and intensity of flare. Posterior segment activity was based on the clinician’s impression of significant vitritis, vasculitis, chorioretinitis, and papillitis. Cases of intermediate uveitis, posterior uveitis, and panuveitis were recorded as per clinical observation.
Diagnostic and inclusion criteria:
The First International Workshop on Ocular Sarcoidosis (FIWOS) recommended four levels of certainty for diagnosis in patients in whom other possible causes of uveitis had been excluded5:(1) biopsy-supported diagnosis with a compatible uveitis was labelled as definite ocular sarcoidosis; (2) if biopsy was not done but the chest X-ray was positive showing bihilar lymphadenopathy associated with a compatible uveitis, the condition was labelled as presumed ocular sarcoidosis; (3) if biopsy was not done and the chest X-ray did not show bihilar lymphadenopathy but there were three of the classic intraocular signs and two positive laboratory tests, the condition was labelled as probable ocular sarcoidosis; and (4) if lung biopsy was done and the result was negative but at least four classic intraocular signs and two positive laboratory investigations were present, the condition was labelled as possible ocular sarcoidosis. Only patients with definite, presumed or probable sarcoidosis were included in this study. Patients with myopia or hypermetropia greater than 6 dioptres were excluded from the study to avoid the influence of axial length on choroidal parameters.
Image acquisition:
Each patient was scanned using Topcon DRI OCT Triton Swept Source OCT using 1050 nm wavelength light wherein, a macular centered scan was performed on both eyes, and consisted of twelve OCT radial scans obtained in a radial pattern with a diameter of 12 mm.
Quantitative analysis of OCT images:
All OCT image sets acquired using the Swept source OCT contained 12 radial scans distributed in a radial pattern overlying the area covered by the nine subfields of the Early Treatment Diabetic Retinopathy Study (ETDRS) grid. For each OCT image set, the inner and outer boundaries of both the retina and the choroid were manually segmented.
The choroid was defined as the space between the outer border of the retinal pigment epithelium and choroidoscleral junction. The choroid was further subdivided into Haller’s large vessel and Sattler’s medium vessel layers. On OCT, the walls of blood vessels appear hyperreflective, and their lumens appear hyporeflective. Haller’s large vessel layer was defined as the outer choroid, consisting of large hypointense spaces representing large vascular luminal spaces.10 Sattler’s medium vessel layer consisted of small- to medium-sized hypointense spaces, surrounded by hyperintense stroma, giving a mottled appearance on scans. Sattler’s layer included the choriocapillaries, which is not easily distinguishable from the Sattler’s layer.11,12
The foveal central subfield choroidal thickness parameters were measured automatically by the software within the OCT machine. The segmentation of the Haller’s and the Sattler’s layer was done manually by double blinding while the the thickness was measured using the software.
The foveal central subfield (FCS) corresponds to the ETDRS central subfield (area 1) shown in Fig 1.
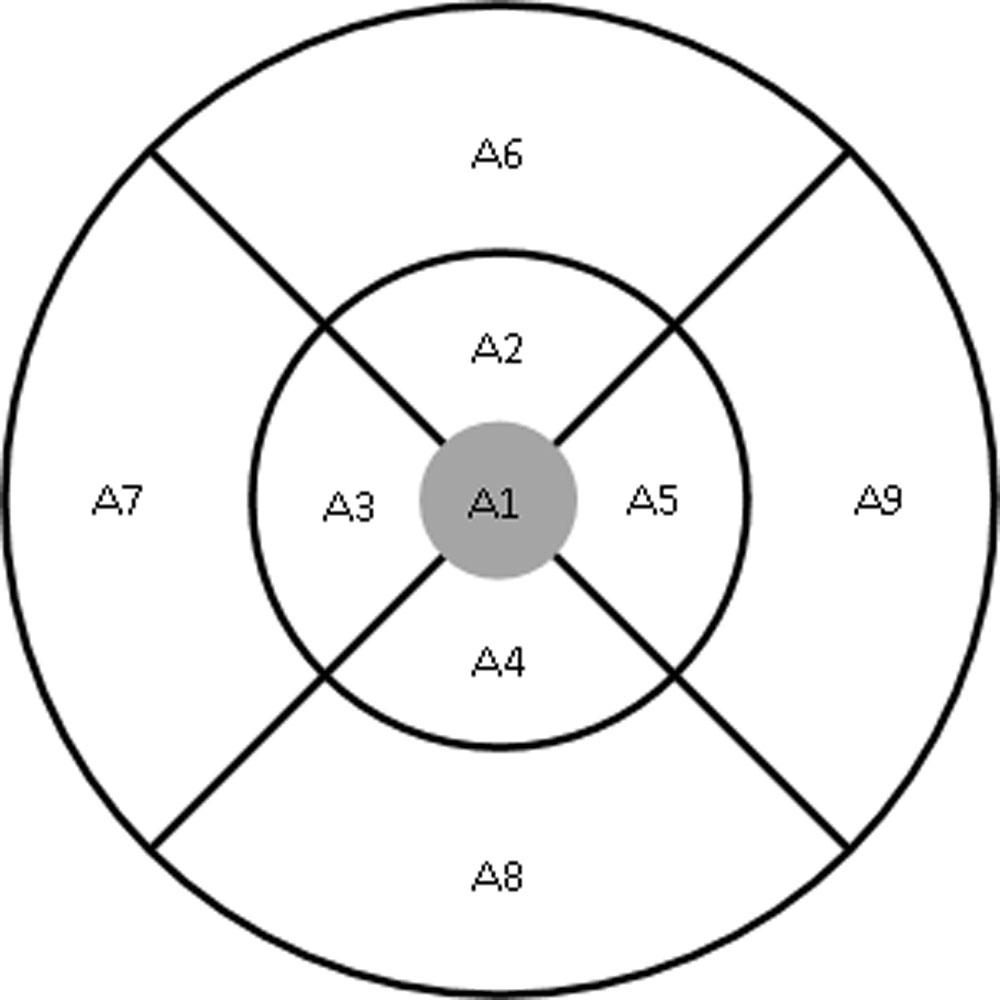
Fig 1: The ETDRS plot of macular topography with nine section represented in alphanumeric form in which A1 (shaded) defines the foveal central subfield (FCS).
Statistical analysis:
The statistical analyses were performed by STATA 11.2 (College Station TX USA). Shapiro wilk test has been used to check the normality, Students t-test were applied to find the significance difference between the total choroid thickness, Sattler’s layer, Haller’s layer and Sattler’s layer to Haller’s layer ratio of the groups (affected eye and normal eyes). The same parameters were compared between affected eye of patients with acute uveitis and chronic uveitis. These were expressed as mean and standard deviation.
Owing to multiple statistical comparisons, we applied a Sidak correction to adjust P-values to a more stringent value of P≤0.004 to allow for an experimental wide type 1 error of 10%. Less stringent P<0.05 were also presented.
Result:
14 patients diagnosed as sarcoidosis related granulomatous uveitis were retrospectively included into the case group. 14 healthy patients were included into control group.
Baseline characteristics
The median age of patients diagnosed with sarcoidosis was 40.71 ± 12.07 years (range =23–64), compared with patients in control group was 35.93 ± 9.62 years (range =23–57). However, this did not reach statistical significance (p= 0.257). There was also no significant difference between gender between groups (p=1.0).
Among the 14 patients diagnosed with sarcoidosis uveitis, 7 (50%) patients had unilateral uveitis and 7 (50%) patients had bilateral uveitis. As per FIWOS recommendation for diagnosis for sarcoidosis, 3 cases (21.43%) were definite sarcoidosis, 5 cases (35.71%) were presumed sarcoidosis and 6 cases (42.86%) were probable sarcoidosis. 4 (28.57%) cases presented as anterior uveitis, 4 (28.57%) as intermediate uveitis, 3 (21.43%) as posterior uveitis and 3 (21.43%) as panuveitis. Out of the 7 patients, 2 (14.29%) patients responded to topical steroid, 11(78.57%) patients required oral steroid and 1(7.14%) patient required immunosuppressant therapy.
The patients were grouped into the affected group which included affected eyes of the 14 patients diagnosed with sarcoidosis uveitis i.e. 21 eyes in the affected group which was further divided into 7 (33.33%) eyes with acute uveitis and 14 (66.67%) eyes with chronic uveitis. 28 eyes of 14 healthy patients were grouped into normal group.
Effects of sarcoidosis associated uveitis on choroidal morphology
Haller’s layer was found to be significantly thinner in affected eyes diagnosed with sacroid related uveitis (180.57 ± 46.78 µm) when compared with eyes in normal group (212.04 ± 33.15 µm) (p=0.008) at FCS choroidal parameter analysis. The comparison of ratio of Sattler’s layer to Haller’s layer among the eyes of the affected (0.67 ± 0.18) and control group (0.50 ± 0.09) was found to be statistically significant (p<0.001). However, the total choroidal thickness was thinner in the affected eyes (297.29 ± 69.37 µm) when compared to control eyes (317 ± 44.06 µm) but did not reach significance (p=0.231) while the Sattler’s layer was found to be thicker in the affected eyes (116.71 ± 31.94 µm) but not statistically different in comparison to the control eyes (104.96 ± 18.11µm) (p= 0.109).
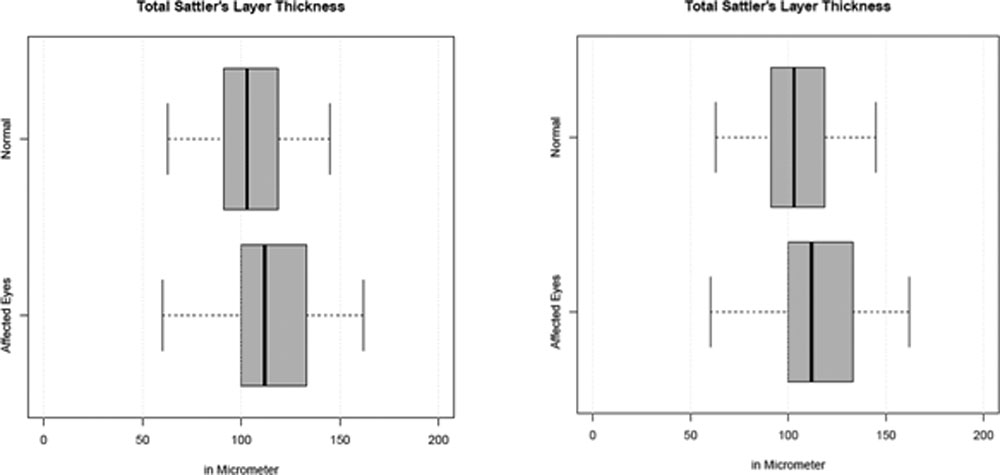
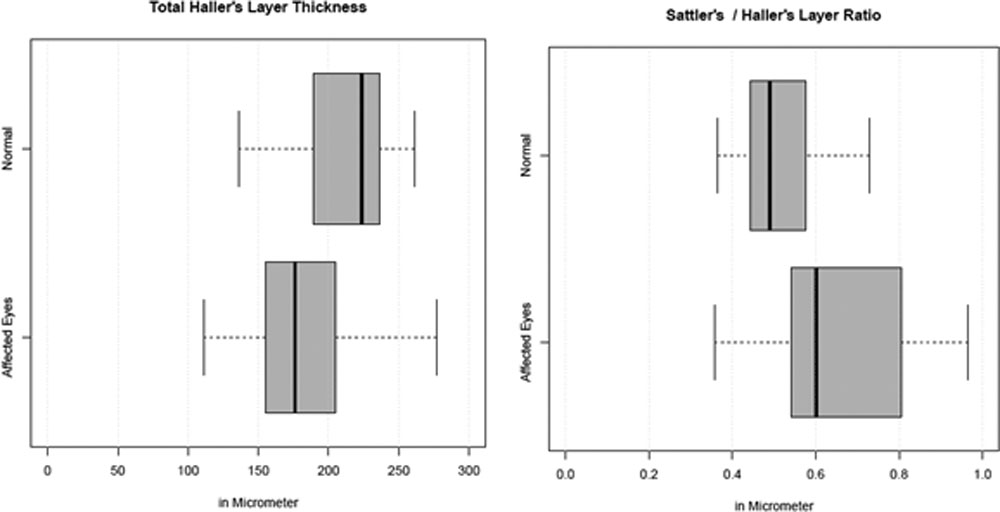
Fig 2: Box plot of the thickness of various choroidal parameters at the foveal central subfield (FCS) in the affected eyes diagnosed with sarcoid related uveitis and normal healthy eyes. In the box plot,the median is represented by the solid line within the box. Quartiles 1 and 3 are delineated by the borders of the box. The whiskers extend from quartile 1 to the minimum value and from quartile 3 to the maximum value. (A) the total choroidal thickness was not significantly thinner in the affected eyes when compared to normal eyes (p=0.231).(B) the Sattler’s layer was thicker in the affected eyes but
Effect of number of duration of uveitis on choroidal morphology
The choroidal thickness of affected eyes of patients who had acute uveitis (344.29 ± 73.83 µm) was compared to affected eyes of patients who had chronic uveitis (273.79 ± 55.73 µm) at FCS. It was found that the choroidal thickness at FCS was statistically different between affected eyes of patients who had acute uveitis and affected eyes of patients who had chronic uveitis (p=0.024). There was no significant difference when affected eyes of patients who had acute uveitis were compared to eyes of normal patients (p=0.213) at FCS but there was significant difference when affected eyes of patients who had chronic uveitis were compared to the eyes of normal patients (p=0.009).
The Sattler’s layer at FCS in the affected eyes of patients who had acute uveitis (129.14 ± 20.38 µm) when compared to eyes of normal patients (104.96 ± 18.11µm) at FCS was significantly thicker (p=0.004). However, the Haller’s layer thickness at FCS was comparable in the affected eyes of patients who had acute uveitis (215.83 ± 56.07 µm) and eyes of normal patients (212.04 ± 33.15 µm) (p=0.849). Comparison of the ratio of the Sattler’s layer to Haller’s layer in the affected eyes of patients who had acute uveitis (0.62 ± 0.05) and eyes of normal patients (0.50 ± 0.09) was found to be statistically significant (p=0.006).
On analysis, statistically thinner Haller’s layer at FCS was observed in the affected eyes of patients who had chronic uveitis (163.29 ± 30.84 µm) when compared to eyes of normal patients (212.04 ± 33.15 µm) (p<0.001). There was thicker Sattler’s layer in the affected eyes of patients who had chronic uveitis (110.50 ± 25.40 µm) compared to eyes of normal patient (104.96 ± 18.11µm) but was not significant (p=0.504). The ratio of the Sattler’s layer to Haller’s layer in the affected eyes of patients who had chronic uveitis (0.68 ± 0.20) and eyes of normal patients (0.50 ± 0.09 µm) was significantly different (p<0.001).
Affected eyes of patients who had chronic uveitis (163.29 ± 30.84 µm) were observed to have statistically thinner Haller’s layer at FCS compared with affected eyes of patients who had acute uveitis (215.83 ± 56.07 µm) (p=0.012) while no difference was observed in the Sattler’s layer between the two groups (110.50 ± 25.40 µm and 129.14 ± 20.38 µm respectively) (p=0.215). The ratio of the Sattler’s layer to Haller’s layer in the affected eyes of patients who had chronic uveitis (0.68 ± 0.20) was not different compared to affected eyes of patients who had acute uveitis (0.62 ± 0.05) (p=0.599).
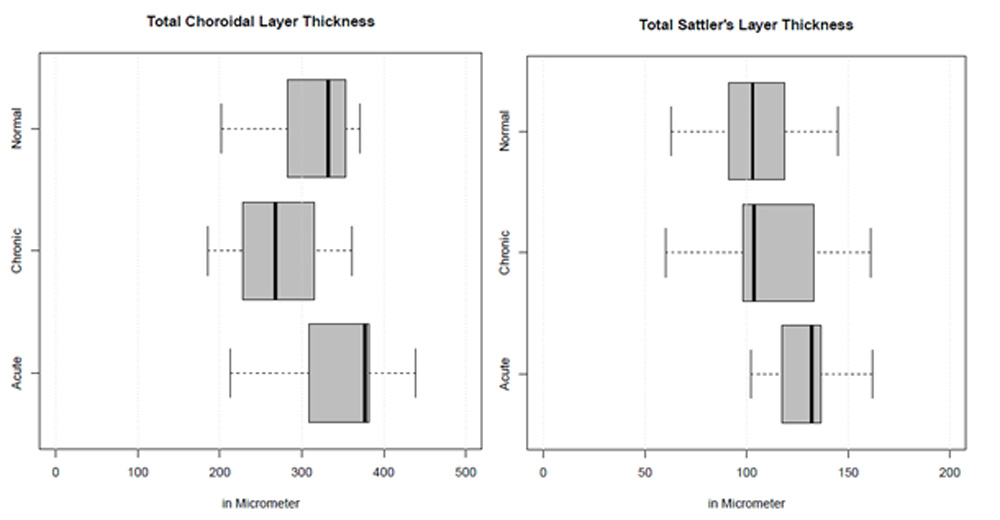
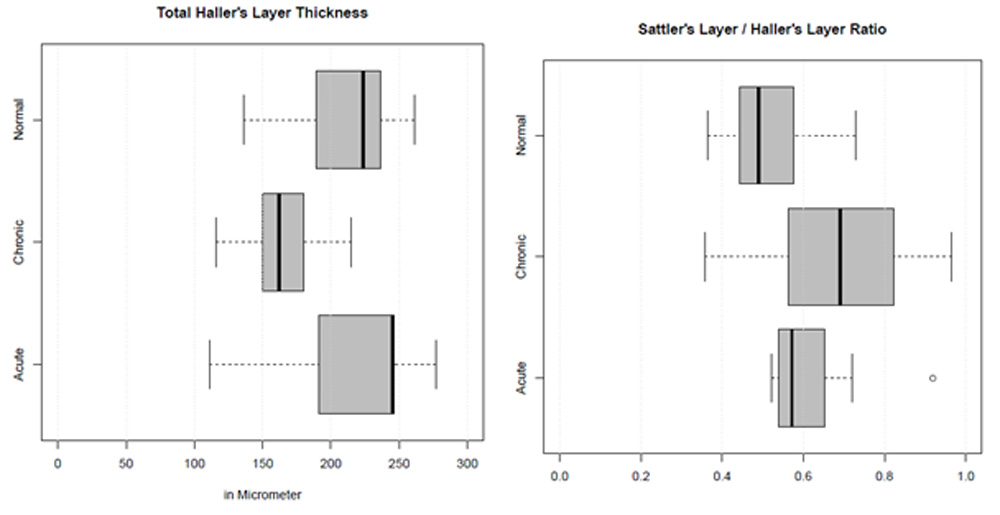
Fig 3: Box plot of the thickness of various choroidal parameters in the affected eyes with acute sarcoid related uveitis, affected eyes with chronic sarcoid related uveitis and normal healthy eyes. (A) Compares the total choroidal thickness among groups. Total choroidal thickness was statistically decreased in affected eyes with chronic uveitis in comparion to affected eyes with acute uveitis (p=0.024) and normal eyes (p=0.009). (B) Compares the Sattler’s layer thickness among groups. The Sattler’s layer thickness in acute uveitis affected eyes was significant increased compared to normal eyes (p=0.004). (C) Compares the the Haller’s layer thickness among groups. The Haller’s layer thickness was significantly thinner in the affected eyes with chronic uveitis compared to affected eyes with acute uveitis (p=0.012) and normal eyes (p<0.001). (D) Compares the ratio of Sattler’s layer to Haller’s layer among groups. Ratio of Sattler’s layer to Haller’s layer was significantly different to acute uveitis affected eyes (p=0.006) and chronic uveitis affected eyes (p<0.001).
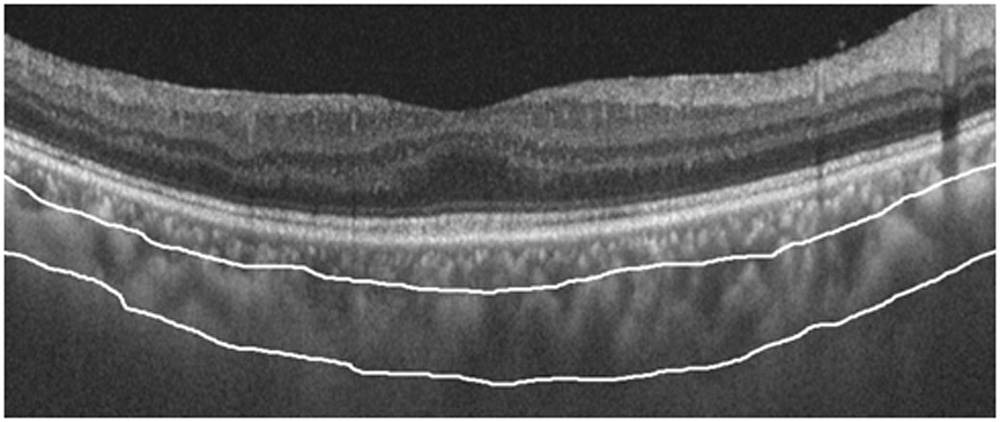
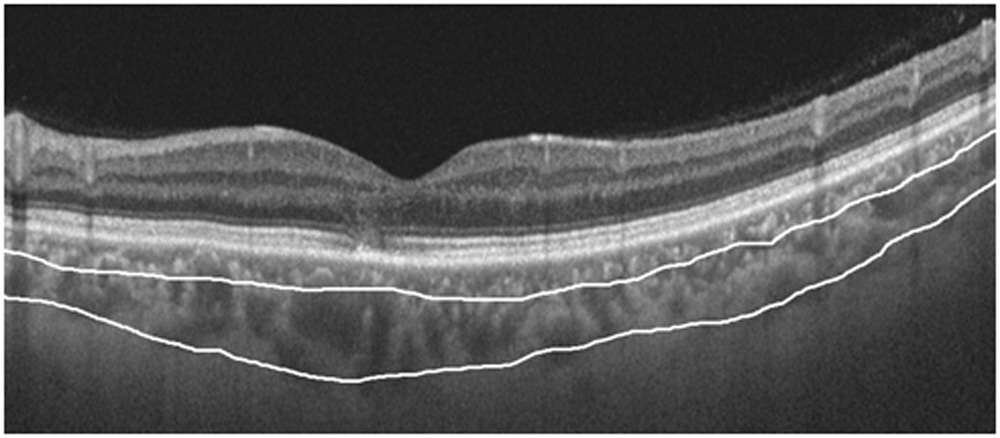
Fig 4: Swept Source OCT image of the choroid with manual segmentation in (A) affected eye with acute sarcoid related uveitis, (B) affected eye with chronic sarcoid related uveitis.
DISCUSSION:
In this retrospective study, a detailed analysis about the choroidal parameters obtained by OCT images was done in eyes of patients affected by sarcoidosis. We compared the OCT- derived choroidal parameters with the age and gender matched controls. The effects of acute and chronic uveitis on the choroidal parameters were also taken into consideration.
Choroidal thickness at the posterior pole, based on histopathological studies, was reported as 220 μm in earlier studies.13 However, there can a false thinner valuation because the fixation techniques can cause tissue shrinkage and thereby, underestimating the true thickness of the choroid. OCT-derived normative values of choroidal thickness have been derived in various population and ranges from 262 to 332 μm.14-19 In our study, the total choroidal thickness was 317 ± 44.06 µm at FCS which is within the normal range according to previous study.
Total choroidal thickness had decreases in the affected eyes of the patients with sacroidosis associated uveitis when compared to the eyes of normal healthy patients. Previous study on idiopathic panuveitis cases stated decreased choroidal thickness in the affected eyes of patients.6 However, all their patients had clinically inactive disease at the time of data acquisition. The mean subfoveal choroidal thickness in 16 eyes of active VKH was thicker on presentation which decreased on starting of corticosteroid treatment.9 Similarly, EDI study on Behcet uveitis found increased subfoveal choroidal thickness in active compared to quiescent uveitis but was thicker in comparison to normal population even in quiescent uveitis.20 Haller’s layer was significantly thinner in the eyes of patients diagnosed with sarcoidosis as compared to eyes of normal patients while Sattler’s appeared to be thicker but not statistically significant. H Mehta et al21 in their study found Sattler’s medium vessel layer on average contributed 48.3% of the total macular choroidal thickness in sarcoid uveitis. A previously published study on healthy subjects reported that Sattler’s layer contributed ~ 20–30% of the macular choroidal thickness22. In our study, 39.25% of the total choroidal thickness was contributed by Sattler’s layer.
Haller’s layer was observed to thinner in the affected eyes of patients who had chronic uveitis compared to eyes of normal patients. On the other hand, Sattler’s layer was observed to thicker in affected eyes of patients who had acute uveitis compared to eyes of normal patient. Previous studies have also noted that Sattler’s later to be thicker in the sarcoidosis associated uveitis affected eyes.24 However, in our study, Sattler’s layer appeared to thicker in affected eyes of patients who had acute uveitis as well as affected eyes of patients who had chronic uveitis as compared to eyes of normal patients but reached significant difference only when compared with affected eyes of patients who had acute uveitis. A clinicopathological study of a patient with sarcoid posterior uveitis done by Gass and Olson23 in 1976, found that lesions labelled as ‘focal choroiditis’ were actually below the retinal pigment epithelium and not within the choroid. Other studies too had supporting findings, observing that in sarcoid-associated uveitis, superficial choroidal involvement were more frequently involved with sparing of the deeper layers24,25. We can hypothesis that, initially in the acute phase of inflammation, sarcoidosis has a primary effect only on the superficial vascular layer of choroid i.e. the Sattler’s layer and the choroicapillaries sparing the Haller’s layer. A possible explanation for thickening of the Sattler’s layer is that in the presence of inflammation, the mediators such as prostaglandins are released locally causes blood vessels to dilate.26 This does not occur in the vessels of the retinal blood flow is auto regulated while there is no such auto regulatory mechanism in choroid is present.27 Another hypothesis for thickening of the choroid could be caused by a non-necrotizing granulomatous inflammation with infiltration of lymphocytes, epithelioid and giant cells, especially in the choroidal stroma. Similar feature was stated by Inomata H and Rao NA28 in acute stage of VKH. On the contrary, long standing inflammation or repeated episode of inflammations, affects the Haller’s layer thereby causing thinning of the choroid. H Mehta21 et al too mentioned that occurrence of choroidal inflammation over extended periods ultimately leads to generalized choroidal atrophy and thinning. Similar study on idiopathic panuveitis also observed thinning of the Haller’s layer of choroid irrespective of the duration of uveitis.6 Rao29 has described the pathology of VKH as, infiltration of inflammatory cells in the acute phase leads to choroidal stromal oedema, which, in turn, compresses the vessels in choroidal stroma and, consequently, decreases choroidal blood flow. Choroidal ischaemia and hypoperfusion in uveitis has also been hypothesized by an ICGA based study.30 Based of these earlier studies, we can hypothesize that the thinner Haller’s layer observed in the eyes with chronic uveitis would be based on the choroidal ischaemia and hypoperfusion.
The ratio of Sattler’s layer to Haller’s layer ratio in affected eyes with acute uveitis as well as in affected eyes with chronic uveitis was observed to be comparable with each other but significantly different from the normal population. Thus, there is a necessity for a larger cohort study to understand the role of choroidal parameters for diagnosis of ocular sarcoidosis.
To the author’s knowledge, this is the only SS-OCT study comparing the choroidal parameters in sarcoid related uveitis with normal population. This is probably the first study describing the effect of chronic uveitis and acute uveitis on choroidal parameters and its comparison with normal population. The main drawback of the study is its retrospective nature which is associated with inherent bias. Probably, a prospective study with a larger cohort would confirm our finding. The influence of the axial length on the choroidal thickness is well known.31-36 Though high refractive errors were excluded in our study, the cases and controls have to be comparable with respect to each other to avoid the confounding factor. In our study, manual segmentation of choroidal layers was done due to unavailability of software in current OCT machine. Future development of technology would help in more precise segmentation of the choroidal layers.
CONCLUSION:
We conclude that Sattler’s layer is the layer of choroid which primarily gets thickened in ocular sarcoidosis and eventually, in longer standing cases, Haller’s layer also gets thinned out. A larger prospective cohort study as well as histopathological evidences is required to establish the confirmation of the findings observed in our study. Such a study would pave the way for diagnosis of ocular sarcoidosis in a non invasive way and also be a stepping stone for understanding the pathogenesis of ocular sarcoidosis in future.
KEY WORDS: sarcoid, choroid, OCT, Sattler’s, Haller’s.
KEY MESSAGE: The inflammatory process occurring in the sarcoid uveitis can be assessed in a non invasive way using SS-OCT. Choroidal thickness are a guide to the changes occurring n the choroid during in the course of the disease, which can pave way in future for understanding the pathogenesis of ocular sarcoidosis.
References:
- Newman LS, Rose CS, Maier LA. Sarcoidosis. N Engl J Med 1997; 336:1223–34.
- Albert DM, Jakobiec FA, Hunter DG, et al. Ocular manifestations of sarcoidosis. In: Albert DM, Jakobiec FA, editors. Principles and practice of ophthalmology . Philadelphia:WB Saunders, 1994:p. 443–450.
- Herbort CP, Rao NA, Mochizuki M. International criteria for the diagnosis of ocular sarcoidosis: results of the first International Workshop On Ocular Sarcoidosis (IWOS) Ocul Immunol Inflamm. 2009;17:160–169.
- Takase H, Shimizu K, Yamada Y, Hanada A, Takahashi H, Mochizuki M. alidation of international criteria for the diagnosis of ocular sarcoidosis proposed by the first international workshop on ocular sarcoidosis. Jpn J Ophthalmol. 2010;54:529–536.
- Keane PA, Allie M, Turner SJ, Southworth HS, Sadda SR, Murray PI, et al. Characterization of birdshot chorioretinopathy using extramacular enhanced depth optical coherence tomography. JAMA Ophthalmol. 2013;131:341–350.
- Karampelas M, Sim DA, Keane PA, Zarranz-Ventura J, Patel PJ, Tufail A, et al. Choroidal assessment in idiopathic panuveitis using optical coherence tomography. Graefes Arch Clin Exp Ophthalmol. 2013;251:2029–2036.
- Zhang X, Zuo C, Li M, Chen H, Huang S, Wen F. Spectral-domain optical coherence tomographic findings at each stage of punctate inner choroidopathy. Ophthalmology. 2013;120:2678–2683.
- Zarranz-Ventura J, Sim DA, Keane PA, Patel PJ, Westcott MC, Lee RW, et al. Characterization of Punctate Inner Choroidopathy Using Enhanced Depth Imaging Optical Coherence Tomography. Ophthalmology. 2014;121:1790–1797.
- Nakayama M, Keino H, Okada AA, Watanabe T, Taki W, Inoue M, et al. Enhanced depth imaging optical coherence tomography of the choroid in Vogt-Koyanagi-Harada disease. Retina. 2012;32:2061–2069.
- Adhi M, Lau M, Liang MC, Waheed NK, Duker JS. Analysis of the thickness and vascular layers of the choroid in eyes with geographic atrophy using spectral-domain optical coherence tomography. Retina 2014; 34: 306–312.
- Sim DA, Keane PA, Mehta H, Fung S, Zarranz-Ventura J, Fruttiger M et al. Repeatability and reproducibility of choroidal vessel layer measurements in diabetic retinopathy using enhanced depth optical coherence tomography. Invest Ophthalmol Vis Sci 2013; 54: 2893–2901.
- Branchini LA, Adhi M, Regatieri CV, Nandakumar N, Liu JJ, Laver N et al. Analysis of choroidal morphologic features and vasculature in healthy eyes using spectral-domain optical coherence tomography. Ophthalmology 2013; 120: 1901–1908.
- Guyer DR, Schachat AP, Green WR (2006) The choroid: structural considerations. In: Ryan SJ (ed) Retina. Elsevier, Philadelphia, pp 33–42
- Margolis R, Spaide RF (2009) A pilot study of enhanced depth imaging optical coherence tomography of the choroid in normal eyes. Am J Ophthalmol 147:811–815
- Ikuno Y, Maruko I, Yasuno Y, Miura M, Sekiryu T, Nishida K, Iida T (2011) Reproducibility of retinal and choroidal thickness measurements in enhanced depth imaging and high-penetration optical coherence tomography. Investig Ophthalmol Vis Sci 52:5536–5540
- Rahman W, Chen FK, Yeoh J, Patel P, Tufail A, Da Cruz L (2011) Repeatability of manual subfoveal choroidal thickness measurements in healthy subjects using the technique of enhanced depth imaging optical coherence tomography. Investig Ophthalmol Vis Sci 52:2267–2271
- Yamashita T, Yamashita T, Shirasawa M, Arimura N, Terasaki H, Sakamoto T (2012) Repeatability and reproducibility of subfoveal choroidal thickness in normal eyes of Japanese using different SDOCT devices. Investig Ophthalmol Vis Sci 53:1102–1107
- Ding X, Li J, Zeng J, Ma W, Liu R, Li T, Yu S, Tang S (2011) Choroidal thickness in healthy Chinese subjects. Investig Ophthalmol Vis Sci 52:9555–9560
- Fujiwara A, Shiragami C, Shirakata Y, Manabe S, Izumibata S, Shiraga F (2012) Enhanced depth imaging spectral-domain optical coherence tomography of subfoveal choroidal thickness in normal Japanese eyes. Jpn J Ophthalmol 56:230–235
- Kim M, Kim H, Kwon HJ, Kim SS, Koh HJ, Lee SC. Choroidal thickness in Behcet’s uveitis: an enhanced depth imaging-optical coherence tomography and its association with angiographic changes. Invest Ophthalmol Vis Sci 2013;54: 6033–6039.
- Mehta H, Sim DA, Keane PA, Zarranz-Ventura J, Gallagher K, Egan CA, et al. Structural changes of the choroid in sarcoid- and tuberculosis-related granulomatous uveitis. Eye (Lond) 2015;29:1060-8
- Branchini LA, Adhi M, Regatieri CV, Nandakumar N, Liu JJ, Laver N et al. Analysis of choroidal morphologic features and vasculature in healthy eyes using spectral-domain optical coherence tomography. Ophthalmology 2013; 120:1901–1908.
- Gass JD, Olson CL. Sarcoidosis with optic nerve and retinal involvement. Arch Ophthalmol 1976; 94: 945–950.
- Campo RV, Aaberg TM. Choroidal granuloma in sarcoidosis. Am J Ophthalmol 1984; 97: 419–427.
- Spalton DJ, Sanders MD. Fundus changes in histologically confirmed sarcoidosis. Br J Ophthalmol 1981; 65: 348–358.
- Williams TJ. Oedema and vasodilatation in inflammation: the relevance of prostaglandins. Postgrad Med J 1977; 53: 660–662..
- Bill A, Sperber GO. Control of retinal and choroidal blood flow. Eye (Lond) 1990; 4(Pt 2): 319–325.
- Inomata H & Rao NA. Depigmented atrophic lesions in sunset glow fundi of Vogt–Koyanagi–Harada disease. Am J Ophthalmol131:607–614.
- Rao NA. Pathology of Vogt–Koyanagi–Harada disease. Int Ophthalmol27: 81–
- Howe L, Stanford M, Graham E, Marshall J (1998) Indocyanine green angiography in inflammatory eye disease. Eye (Lond) 12:761–767
- Margolis R, Spaide RF (2009) A pilot study of enhanced depth imaging optical coherence tomography of the choroid in normal eyes. Am J Ophthalmol 147:811–815
- Ikuno Y, Maruko I, Yasuno Y, Miura M, Sekiryu T, Nishida K, Iida T (2011) Reproducibility of retinal and choroidal thickness measurements in enhanced depth imaging and high-penetration optical coherence tomography. Investig Ophthalmol Vis Sci 52:5536– 5540
- Rahman W, Chen FK, Yeoh J, Patel P, Tufail A, Da Cruz L (2011) Repeatability of manual subfoveal choroidal thickness measurements in healthy subjects using the technique of enhanced depth imaging optical coherence tomography. Investig Ophthalmol Vis Sci 52:2267–2271
- Yamashita T, Yamashita T, Shirasawa M, Arimura N, Terasaki H, Sakamoto T (2012) Repeatability and reproducibility of subfoveal choroidal thickness in normal eyes of Japanese using different SDOCT devices. Investig Ophthalmol Vis Sci 53:1102–1107
- Ding X, Li J, Zeng J, Ma W, Liu R, Li T, Yu S, Tang S (2011) Choroidal thickness in healthy Chinese subjects. Investig Ophthalmol Vis Sci 52:9555–9560
- Fujiwara A, Shiragami C, Shirakata Y, Manabe S, Izumibata S, Shiraga F (2012) Enhanced depth imaging spectral-domain optical coherence tomography of subfoveal choroidal thickness in normal Japanese eyes. Jpn J Ophthalmol 56:230–235
Leave a Comment