
Dr. Shilpi Narnaware, N17511, Dr. Prashant Keshao
Bawankule
Pseudophakic Retinal Detachments: Success after PPV without Belt buckle with ILM peel
Title / Purpose: To compare primary success rate of PPV with or without ILM Peel in pseudophakic RRD
Methods: A retrospective observational study was conducted on 111 eyes of 111 pseudophakic RD patients undergone PPV with/without ILM peel. Eyes were grouped into A) PPV with no ILM peel B) PPV with ILM peel. Primary success rates were obtained & compared statistically for significance of difference across groups using Pearsons chi-square test. Exclusion criteria included previous RD surgery.
Results :Primary success with no peel was 88.2% (45/51) & with ILM peel was 96.7% ( 58/60). The difference in primary success across the groups was statistically significant with p value of 0.009
Conclusion :Primary anatomic success rate of PPV with ILM peel is significantly higher.
INTRODUCTION :
Although all retinal detachments have the potential to threaten vision and cause permanent loss of sight, pseudophakic detachments have some unique characteristics. Because affected eyes often are older, the vitreous tends to be more syneretic and fluid, which leads to faster accumulation of subretinal fluid and quicker progression of detachments.
Moreover, the fundus view is often impaired by anterior or posterior capsular opacification, reflections / optical aberrations from intraocular lens, or poor mydriasis leading to poor detection of retinal tears which are often smaller and multiple.
To date high-level evidence is lacking regarding the question whether an encircling band in addition to vitrectomy in the treatment of pseudophakic retinal detachment (PRD) improves outcome. While several retrospective or non-randomised studies reported almost complete success of combined surgery[1 ,2] other studies found no benefit of an additional encircling band compared with vitrectomy alone.[3–5] An ancillary analysis of the randomised SPR study (Scleral buckling versus primary vitrectomy in rhegmatogenous retinal detachment study) which compared vitrectomy and scleral buckling in the treatment of patients with retinal detachment of medium complexity showed that in pseudophakic patients treated with vitrectomy the use of an additional buckle resulted in a significantly lower redetachment rate of 11.4% vs 40.9% in patients who were treated by vitrectomy alone.[6] In contrast an analysis of survey data on 4179 patients with retinal detachments showed a slightly higher failure rate for combined surgery versus vitrectomy alone,[7] though selection bias, for example, due to favouring an additional buckle in difficult situations, cannot be ruled out.
Traction has 3 components : 1) Antero-posterior 2) Circumferential 3) Tangential.
Vitrectomy relieves antero-Posterior and circumferential traction. Encircling band & base excision relieve the circumferential traction. Membrane Peeling relieves the tangential traction on the surface of Retina.
ILM as a cause of tangential traction is well established and is responsible for development of macular hole. Peeling of ILM leads to relief of this traction and thereby increases rate closure of full thickness macular hole [9].
ILM as a cause / role of tangential traction in retinal detachment & PVR and its relief by peeling internal limiting membrane during vitrectomy has not been addressed in any previous study.
Methods
Study design
A retrospective observational study was conducted on 111 eyes of 111 patients with primary pseudophakicRRD’s during January 2012 – February 2016 at SarakshiNetralaya, Nagpur, Maharashtra, India. Eyes were grouped into 1) PPV with no ILM peel 2) PPV with macular &peri-papillary peel. For the purpose of the study, only patients undergoing vitrectomy in cases of primary RRD were selected. Patients with subtotal or total RRD with a giant retinal tear, retinal dialysis, multiple retinal breaks, posterior breaks, RRD with vitreous hemorrhage and retinal detachments with preoperative PVR (all grades), were included in the study. PVR stage was graded according to the updated classification of Retina Society Terminology Committee (1991) [10]
Excluded from the study were patients with history of trauma, combined detachments, history of any previous retinal surgery & patients with incomplete follow-up period.
Surgical procedure
In all cases, 23 Gauge PPV with Alcon constellation was performed using a noncontact wide-angle viewing system (Oculus BIOM). After receiving informed consent, surgery was performed mostly under local anaesthesia. Trocars were placed in a way that allows peripheral vitrectomy to be performed without touching the lens, and also switching between the 3 entry sites, if necessary. Core vitrectomy was followed by PVD induction. Membranes were peeled. Base excision was done in all cases. No cases received encircling / sclera buckle. The first group did not undergo ILM Peel. In group 2, ILM was stained with brilliant blue dye. ILM was peeled at macular and peri-papillary area ILM was peeled (Diagram 1). PFCL was used to flatten the retina & then PFCL –air exchange was done. Endolaser photocoagulation using curved probe& was applied around the retinal tear & 360° to the vitreous base. All patients received SO (1000 Centistokes) tamponade at the end of the surgery. Patients were examined postoperatively and followed for at least 6 months after Silicone Oil Removal.
Diagram 1
Statistical methods:
The data on factors like demography, duration of event, lens status, location of break and the exposed choroidal area were obtained on patients undergoing PPV. The patients were observed for a period of one year and the primary, secondary and final success were recorded.
Primary success was considered in cases where retina remained attached at 6 months after removal of silicone oil.
Secondary success was defined as retina remained attached after the last procedure.
Final success is the cumulative of primary and secondary success.
The probability of final success was obtained using following expressions:
P (Final success) = 1 – P (Failure at 2nd surgery)
= 1 – [P (Failure at 1st surgery) * P (Failure at 2nd surgery/Failure at 1st surgery)]
Let n1 be the initial number of patients who underwent surgery for 1st time, and r1 be the number of success in first attempt (primary success). Let n2 be the number of patients undergoing surgery for second time due to recurrence, and r2 be the number of successes in the second attempt. Then the probability of success at second attempt is given by:
…(*)
If c1 is number of censored cases after 1st surgery, then n2 is defined as:
n2 = n1 – r1 – c1
Further, recurrence rates were obtained graphically for each factor according to respective levels and procedures using Kaplan-Meier plots. The statistical significance of difference across the three procedures was determined using log-rank test. All the analyses were performed using SPSS ver 20.0 (IBM Corp) and statistical significance was evaluated at 5% level.
RESULTS :
| Procedure | Primary success | p-value |
| With peel (60) | 58 (96.67%) | 0.009 |
| Without peel (51) | 45 (88.23%) | |
| Total (111) | 103 (92.79%) |
The data on 111 eyes of 111 pseudophakic patients who undergone PPV with and without ILM peel was obtained and analyzed for the success rates. Out of 111 eyes, 60 had PPV with ILM peel, while 51 had PPV without ILM peel. Primary success was obtained for eyes in both the groups. It was defined as patients not showing retinal detachment within first 6 months after silicone oil removal. In the ILM peel category, there were 58 eyes with primary success, giving a success rate of 96.7%, while in the without ILM peel category, there were 45 eyes with primary success, giving a success rate of 88.2% , p-value = 0.009. In other words, the primary success was higher in with peel category as compared to without peel.
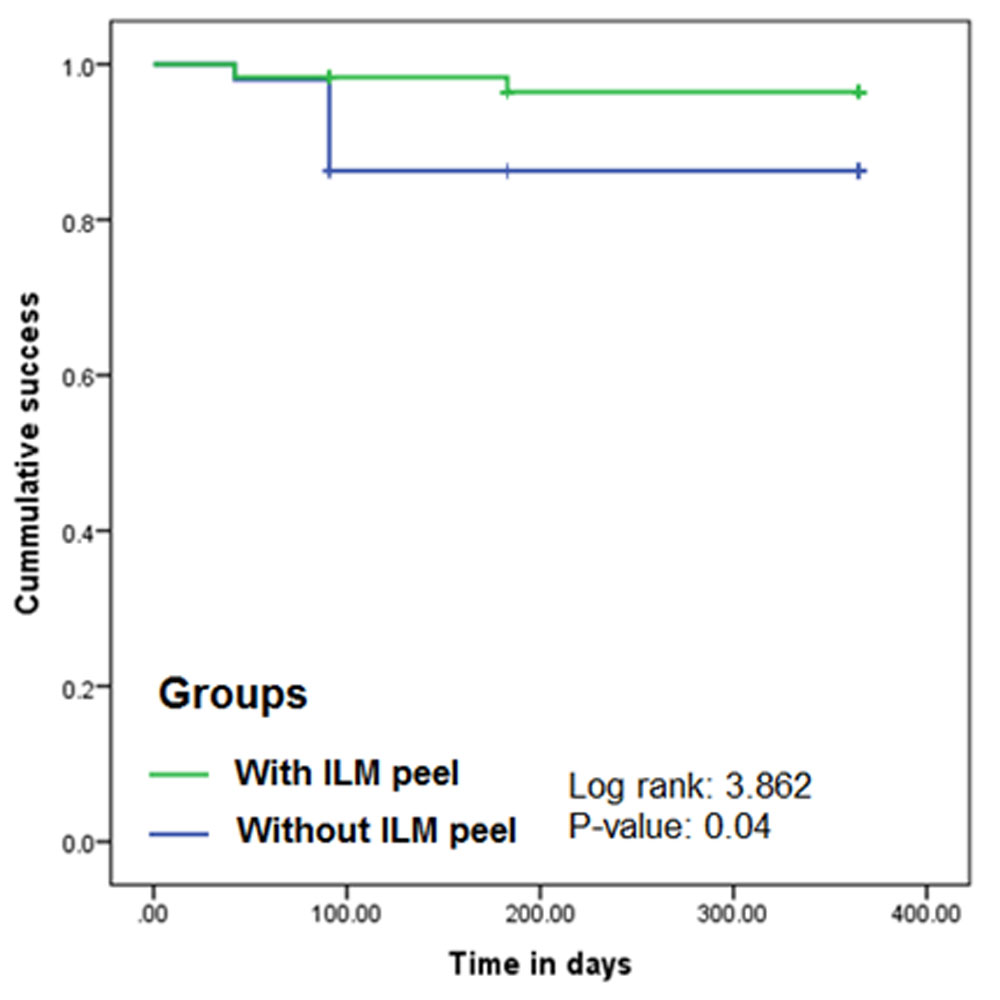
The statistical significance of difference in the treatment effect was determined using the non-parametric Kaplan-Meier analysis. The equality of survival distribution was evaluated using Log-rank test. The test resulted into a Chi-square value of 3.862 (DF=1) with a p-value of 0.04. This indicated that the difference in the survival distribution of PPV with and without ILM peel was statistically significant. The visualization of the same is given through KM plot in Figure 1. It is evident from the figure that the success rate steps down faster with time in without peel category as compared to with peel category; and this step down is statistically significant.
Discussion
Goal of RD surgery in general is to close the retinal breaks and release vitro retinal traction. The best method to treat a RD is one which is relatively safe and controlled, involves minimal manipulation and minimal intra and post-operative complications [11]. Scleral buckling (SB) procedures may pose a problem because of poor visualization due to poor mydriasis, cortical remnants, capsular opacification, glare or pitting from the intra ocular lens implant, corneal opacification, or vitreous opacities may make identification difficult, especially because anterior breaks more commonly occur inpseudophakic and aphakic RDs[12]. In pseudophakic eyes results varied from 82% to 95% as reported by Ho and Tolentino and Johnston et al.
These problems are not encountered in PPV. A better access to the vitreous base in pseudophakic eyes, allows for a better completion of the recommended complete shaving of the vitreous base compared to phakic eyes. The advances in vitreoretinal instrumentation and wide angle viewing systems along with better understanding has improved surgical success rates. A few retinal surgeons expect additional buckling procedures with PPV to provide enhanced support of the vitreous base and better visualisation of the periphery. On the other hand, the additional scleral buckle implies increased invasiveness and operation time, it affects the postoperative refraction and the blood circulation of the eye[8] and may entail specific complications such as buckle migration and infection. The longer duration of surgery may explain a higher stress on the corneal epithelium, risk of perforating the sclera during the fixation of the encircling band and increased incidence of myopia with additional encircling buckle.
Various studies has shown superior success results of PPV alone in primary pseudophakic RRD .High rate of retinal reattachment with a single surgery was shown in the series of Brazitikos et al with a 94% success rate of primary PPV in uncomplicated cases. In complex cases 86.8% anatomical success rate was shown in study byTeke et al. Regler et al. reported an overall 79% final anatomic success rate of PPV for complex RRD ,while a 87.8% success rate was reported in complicated RRD cases by Ozdek et al.
No study addressed the effects of ILM peel in success rate of these RRD which removes tangential traction & might help in prevention of development of PVR & subsequent failure of surgery. In our study, we did not use belt buckle. In pseudophakics the primary success rate was 96.7% in peri -papillary + macular peel group which is significantly higher than No peel group i.e. 88.2%.
Conclusion:
The success of primary vitrectomy with & without belt buckle is established.
In our study primary vitrectomy without belt buckle & with ILM peel showed better success rate compared to previous studies.
The better success rate with addition of this step into surgical procedure probably helps by:
1) Relief of tangential traction 2) Ensures completion of PVD 3) No substrate for reproliferation at posterior pole
References :
- Desai UR, Strassman IB. Combined pars plana vitrectomy and scleral buckling for pseudophakic and aphakic retinal detachments in which a break is not seen preoperatively. Ophthalmic Surg Lasers 1997;28:718–22.
- Devenyi RG, deCarvalho Nakamura H. Combined scleral buckle and pars plana vitrectomy as a primary procedure for pseudophakic retinal detachments. Ophthalmic Surg Lasers 1999;30:615–18.
- Pournaras CJ, Kapetanios AD. Primary vitrectomy for pseudophakic retinal detachment: a prospective non-randomized study. Eur J Ophthalmol 2003;13:298–306.
- Stangos AN, Petropoulos IK, Brozou CG, et al. Pars-plana vitrectomy alone vs vitrectomy with scleral buckling for primary rhegmatogenouspseudophakic retinal detachment. Am J Ophthalmol 2004;138:952–8. doi:10.1016/j.ajo.2004.06.086
- Wickham L, Connor M, Aylward GW. Vitrectomy and gas for inferior break retinal detachments: are the results comparable to vitrectomy, gas, and scleral buckle? Br J Ophthalmol 2004;88:1376–9. doi:10.1136/bjo.2004.043687
- Heimann H, Bartz-Schmidt KU, Bornfeld N, et al. Scleral buckling versus primary vitrectomy in rhegmatogenous retinal detachment: a prospective randomized multicenter clinical study. Ophthalmology 2007;114:2142–54. doi:10.1016/j.ophtha.2007.09.013
- Adelman RA, Parnes AJ, Ducournau D, et al. Strategy for the management of uncomplicated retinal detachments: the European vitreo-retinal society retinal detachment study report 1. Ophthalmology 2013;120:1804–8. doi:10.1016/j.ophtha.2013.01.070
- Ogasawara H, Feke GT, Yoshida A, et al. Retinal blood flow alterations associated with scleral buckling and encircling procedures. Br J Ophthalmol 1992;76:275–9. doi:10.1136/bjo.76.5.275
- Lois N, Burr J, Norrie J et al. Full Thickness Macular Hole & Internal Limiting Membrane Peeling Study ( FILMS) group. Internal Limiting Membrane peeling versus no peeling for idiopathic full thickness macular hole: A pragmatic randomised controlled trial. IOVS 2011;52 (3); 1586-92.
- Machemer R, Aaberg TM, Freeman HM, Irvine AR, Lean JS, Michels RM. An updated classification of retinal detachment with proliferative vitreoretinopathy. Am J Ophthalmol. 1991;112:159–65. doi: 10.1016/S0002-9394(14)76695-4. [PubMed] [Cross Ref]
- Rehman N. Primary vitrectomy for uncomplicated aphakic and pseudophakic retinal detachment. Pak J Ophthalmol. 2000; 4: 16.
- Yoshida A, Ogasawasa H, Jalkh AE. Retinal detachment after cataract surgery. Predisposing factors. Ophthalmology 1992: 99: 453-9.
Leave a Comment