
![]()
Dr. Deepak Megur, M08810, Dr. Bharathi Megur
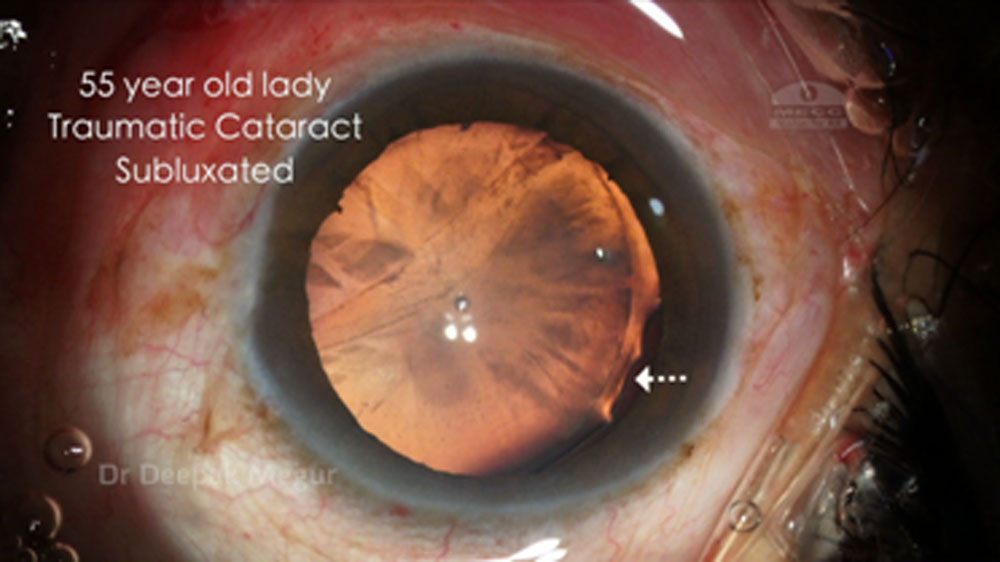
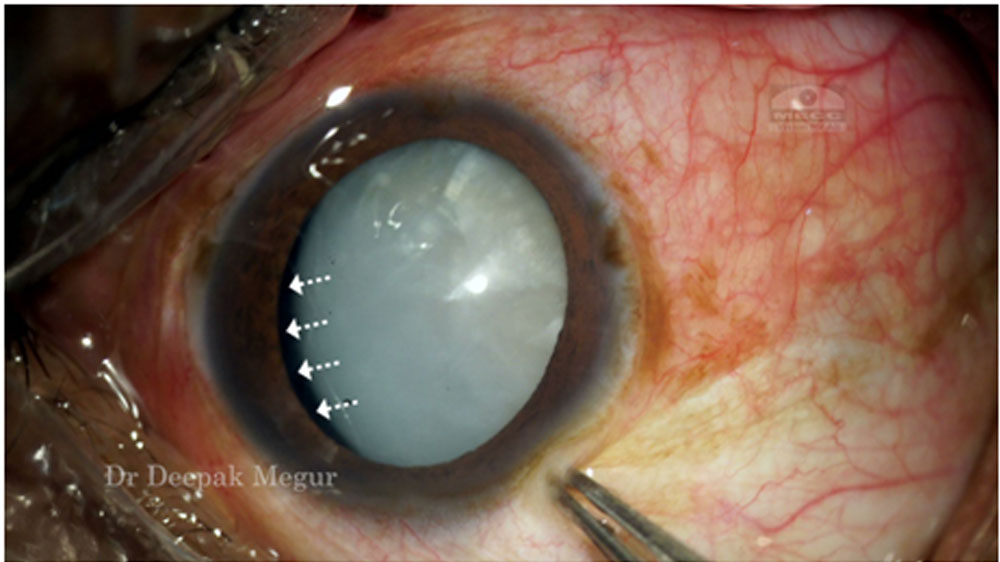
Introduction: Zonular weakness is a commonly encountered entity by the cataract surgeon. Trauma, pseudoexfoliation, inherited connective tissue disorders are some of the common causes for zonular weakness. Performing cataract surgery in eyes with zonular weakness is challenging for the cataract surgeon. The goals while performing surgery in such eyes is to ensure the stability of the capsular bag during cataract removal and placement of a posterior chamber intra ocular lens. Capsule tension rings , segments are standard tools to stabilize the bag. Traditionally the intraocular lens is placed in the bag after the capsular bag is stabilized with Capsular tension rings. However complications associated with this technique are 1) late onset spontaneous dislocation of the capsular bag complex 2) Pseudo phakodonesis 3) Capsular phimosis.
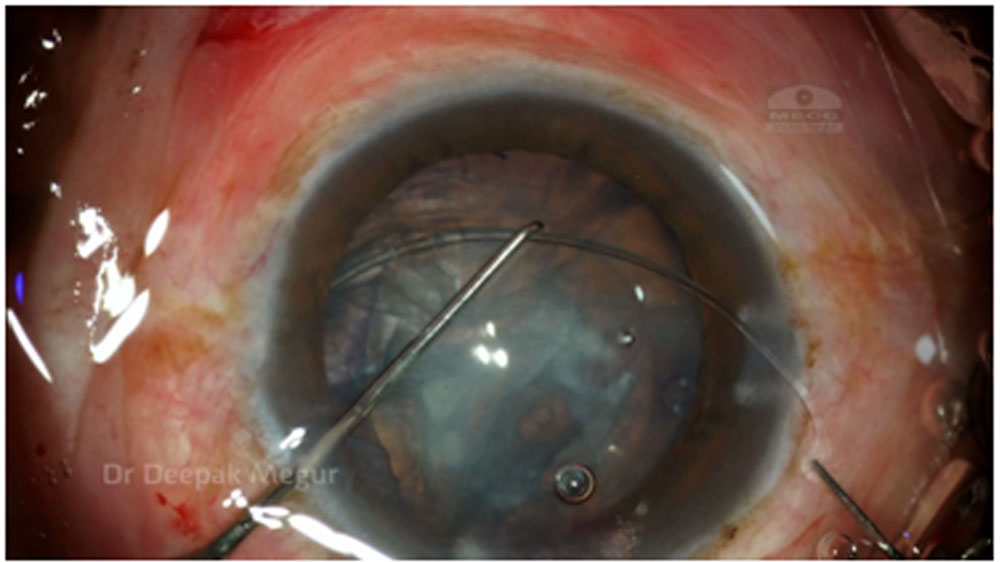
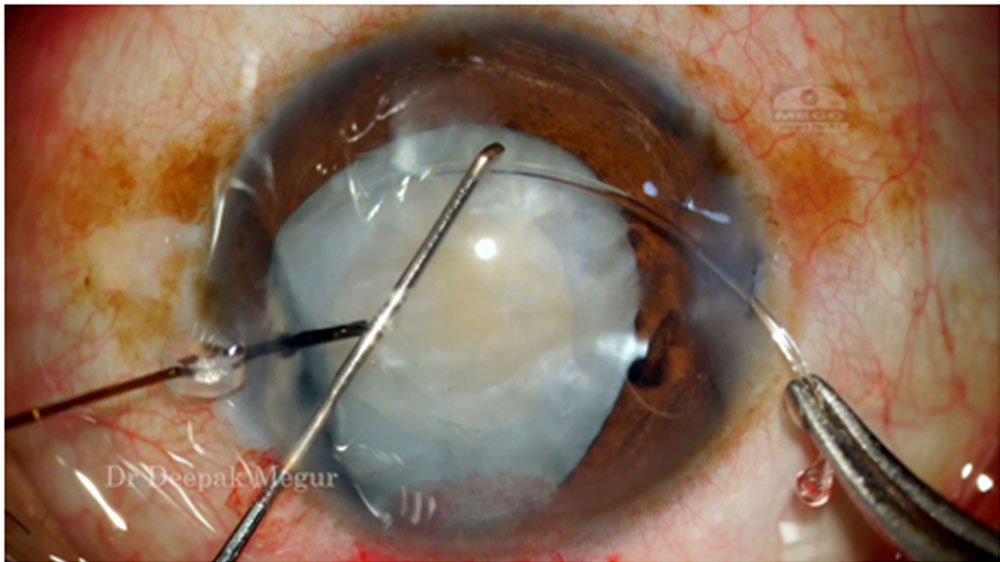
To address these issues, we propose the “ IOL Trap” technique where in after placing the Capsule Tension Ring ( CTR) in the bag, a multipiece hydrophobic IOL is placed intentionally in the sulcus with optic being captured in the capsulorhexis. We used this technique in eyes having subluxated cataract with localized zonular dehiscence of less than 3 clock hours, and in eyes with pseudoexfoliation with weak zonules.
AIM: To analyze outcomes of placing a multi-piece hydrophobic IOL in sulcus with optic capture along with a CTR in the bag in eyes with weak zonules.
Material & Methods:
This was a prospective non comparitive study performed at secondary eye care facility, between January 2012 to December 2016. The eyes included in the study had zonular weakness secondary to trauma or pseudoexfoliation. Eyes with traumatic subluxated cataracts with localized zonular dehiscence of less than 3 clock hours and eyes with pseudoexfoliation were include. Eyes which had gross subluxation more than 3 clock hours and also eyes with severe generalized weakness were not included in the study.A single surgeon performed all the surgeries using a standardized protocol. The surgeries were performed under posterior subtenon’s anesthesia. After performing a Central Curvilinear Capsulorhexis (CCC) , Phacoemulsification of the nucleus was done through a 2.8 mm clear corneal incision, followed by ( in few cases preceded by) implantation of the CTR in the bag and then amultipiece hydrophobic IOL is placed in the sulcus. After removing the OVD behind the IOL the optic of theIOL is nudged posteriorly to ensure optic capture in the CCC. After removing the OVD in the anterior chamber the incisions are hydrated to ensure water tight closure. The post operative evaluation was done on the 1st day, 1 st week, 3 weeks, 6 weeks, then every 6 months for the next 4 years. Eyes with a minimum follow up of 18 months onlywere included in the study. The postoperative evaluation included Uncorrected & Corrected Visual Acuity, Intra Ocular Pressure, Dilated retinal evaluation, OCT Macula. Slit lamp photographs & HD videos with pre & post dilatation were taken to document centration of the IOL, pseudophakodonesisand capsular phimosis. The Outcome measures studied were IOL centration, capsular bag stability, pseudophakodonesis.
Results:
28 eyes with zonular weakness were included in the study. 20 eyes had traumatic subluxated cataracts with localized zonular dehiscence of less than 3 clock hours and the remaining 8 eyes were of pseudo exfoliation with moderate generalized zonular weakness. 15 eyes belonged to men & 13 eyes were of women. Mean age in this group was 61.17 years. 3 eyes required anterior vitrectomy to tackle the prolapsed vitreous secondary to traumatic zonulardehiscence. No other intra –operative complication noted. The mean follow up was of 23.10 months, minimum follow up was of 18 months, and the longest follow up was 38 months. Best corrected vision of 6 /12 or better was achieved in 25 out of the 28 eyes. 3 eyes with BCVA of less than 6/12 were because of epiretinal membrane in 1 eye, macular scar in 1 eye and corneal scar in 1 eye.
Good IOL centration was noted in 26 of the 28 eyes during the entire course of the follow up. 2 eyes had minimal IOL decentration owing to inadequate optic capture in the CCC because of a larger CCC & an eccentric CCC. 2 cases revealed mild anterior capsular phimosis at 12 months but none required any intervention during the follow up period. Mild pseudo-phakodonesis was noted in 16 eyes and moderate phakodonesis was noted in 6 eyes, but none of the patients found it to be bothering enough.
Conclusion: The IOL Trap technique consisting of placing the CTR in the capsular bag followed by intentionally placing the Multipiece Hydrophobic IOL in the sulcus with optic capture in the CCC seems to be an excellent option when dealing with eyes having subluxated cataracts with localized zonular dehiscence and eyes with pseudoexfoliation with zonular weakness. In our study period there was no evidence of late onset dislocation of the IOL bag complex, the IOLs continued to be well centered, and pseudophakodonesis was also minimal.
Discussion:
Traditionally in the bag IOL placement along with CTR is the norm in eyes with zonular weakness. However long term stability of the IOL bag complex is becoming questionable as late disclocation of the IOL Bag complex is being reported. . This new approach of using a CTR in the bag, followed by placing the multi-piece acrylic Hydrophobic IOL haptic in sulcus with optic capture in CCC helps in better weight distribution around the IOL bag complex. The haptics in sulcus over a period of time may get adhered to the underlying uveal tissue by fibrosis and may exert a mild anterior pull on the IOL bag complex. Apart from this the trapping of the optic behind the CCC helps in excellent long term centration of the IOL. However it is critical to have a perfectly sized and perfectly centered CCC to achieve good optic capture. It is also important to note that this technique is not ideal in eyes with grossly subluxated cataracts, which will do better with scleral fixation of the bag

References:
1. Lorente, R., de Rojas, V., Vazquez de Parga, P., Moreno, C., Landaluce, M.L., Domínguez, R., and Lorente, B. Management of late spontaneous in-the-bag intraocular lens dislocation: retrospective analysis of 45 cases. J Cataract Refract Surg. 2010; 36: 1270–1282
View in Article | PubMed | Scopus (46)
2. Mönestam, E.I. Incidence of dislocation of intraocular lenses and pseudophakodonesis 10 years after cataract surgery. Ophthalmology. 2009; 116: 2315–2320
View in Article | PubMed | Scopus (48)
3. Chang, D.F. Prevention of bag-fixated IOL dislocation in pseudoexfoliation [letter]. Ophthalmology. 2002; 109: 1951–1952
View in Article | PubMed
4. Gimbel, H.V., Condon, G.P., Kohnen, T., Olson, R.J., and Halkiadakis, I. Late in-the-bag intraocular lens dislocation: incidence, prevention, and management. J Cataract Refract Surg. 2005; 31: 2193–2204
View in Article | PubMed | Scopus (129)
5. Assia, E.I., Apple, D.J., Morgan, R.C., Legler, U.F.C., and Brown, S.J. The relationship between the stretching capability of the anterior capsule and zonules. (Available at:) (Accessed January 2, 2013)Invest Ophthalmol Vis Sci. 1991; 32: 2835–2839
https://www.iovs.org/content/32/10/2835.full.pdf
View in Article | PubMed
6. Smith, S.G. and Lindstrom, R.L. Malpositioned posterior chamber lenses: etiology, prevention, and management. Am Intra-Ocular Implant Soc J. 1985; 11: 584–591
View in Article | PubMed | Scopus (41)
7. Mello, M.O. Jr., Scott, I.U., Smiddy, W.E., Flynn, H.W. Jr., and Feuer, W. Surgical management and outcomes of dislocated intraocular lenses. Ophthalmology. 2000; 107: 62–67
View in Article | PubMed | Scopus (61)
8. Jacob, S., Agarwal, A., Agarwal, A., Agarwal, S., Patel, N., and Lal, V. Efficacy of a capsular tension ring for phacoemulsification in eyes with zonular dialysis. J Cataract Refract Surg. 2003; 29: 315–321
View in Article | PubMed | Scopus (68)
9. Santoro, S., Sannace, C., Cascella, M.C., and Lavermicocca, N. Subluxated lens: phacoemulsification with iris hooks. J Cataract Refract Surg. 2003; 29: 2269–2273
View in Article | PubMed | Scopus (36)
10. Davison, J.A. Capsule contraction syndrome. J Cataract Refract Surg. 1993; 19: 582–589
View in Article | PubMed | Scopus (243)
11. Werner, L., Pandey, S.K., Escobar-Gomez, M., Visessook, N., Peng, Q., and Apple, D.J. Anterior capsule opacification; a histopathological study comparing different IOL styles. Ophthalmology. 2000; 107: 463–471
View in Article | PubMed | Scopus (127)
12. Gimbel, H.V. and Sun, R. Role of capsular tension rings in preventing capsule contraction [letter]. (reply by C Faschinger, M Eckhardt, 792)J Cataract Refract Surg. 2000; 26: 791–792
View in Article | PubMed | Scopus (14)
13. Nishi, O., Nishi, K., Menapace, R., and Akura, J. Capsular bending ring to prevent posterior capsule opacification: 2 year follow-up. J Cataract Refract Surg. 2001; 27: 1359–1365
View in Article | PubMed | Scopus (60)
14. Gimbel, H.V. and DeBroff, B.M. Intraocular lens optic capture. J Cataract Refract Surg. 2004; 30: 200–206
View in Article | PubMed | Scopus (58)
15. Intraocular lens optic capture in eyes with zonular weakness in cataract patients. KazımDevranoğlu, MD, AylinKılıç, MD’Correspondence information about the author MD AylinKılıçEmail the author MD AylinKılıç, AkifÖzdamar, MD, Ali KeremYurtsever, MPhil, JCRS May 2013Volume 39, Issue 5, Pages 669–672
Leave a Comment