

Dr Rashmi Kumari (K12746 )
![]()
![]()
Abstract
Aim:To comparatively evaluate the surgical outcomeof external dacryocystorhinostomy with two different flap techniques (H /double vs U/single) with respect to surgical time.
Study design -Prospective randomized comparative clinical study
Material and method – 96 patients ofprimary NLD block were selected. 47underwent the conventional DCR by ‘H ‘Shaped flap and 49 by ‘U’Shaped flap with suspension to the orbicularis .Success rate was evaluated bylacrimal patency to irrigation and surgical time was calculated from skin incision to skin suturing. Statistical analysis was done by Chi-square test, T-test and Fisher’s exact test.
Results-Success rate in groups A and B was 93.62% and 95.91% respectively. Surgical time difference between the groups was statistically significant with t =7.2031, p= 0.01(<0.05) while difference in complication rate was not significant (X2 test=0.733 p=0.391).
Conclusion -External dacryocystorhinostomy with H flap has no added advantage over the U flap while the later technique is much easier and less time consuming with comparable success rate.
Key words: External DCR,flap techniques,patency,complication
Introduction;
Nasolacrimal duct (NLD) obstruction, primary or secondary, is one of the important causes of epiphora.[1] Most common cause of primaryNLD block is chronic dacryocystitis .It causes troublesome symptoms like watering and discharge sometimes severe enough to cause social stigma. Medical management gives only temporary relief and the treatment of choice is surgery. The operative approach to the sac may be external or endoscopic. In 1904 Toti first described the external approach and West described the endonasal approach in 1911.[2] The latter approach fell out of favour because of difficult visualization and endonasal access to the lacrimal sac. However, with the newer, rigid telescopes, these difficulties have been overcome resulting in a resurgence of the endoscopic technique. Need of specialised training and very expensive instruments has kept endonasal DCR at backfoot in developing countries where external dacryocystorhinostomy (DCR) still remains the gold standard surgical treatment for epiphora due to NLD block.The aims and objectives of DCR are two folds- to eliminate fluid and mucusretention within the lacrimal sac and to establish a low-resistancedrainage pathway between the conjunctival tear sac and the nasalcavity, by conversion of the lacrimal sac into part of the lateral nasalwall .The procedure is a highly successfulin managing epiphora due to nasolacrimal ductobstruction.[3] The reported success rate varies between 85% to 99%.[4,5]However, surgical procedure is not technically easy and requiresconsiderable experience as well as operative time. The tedious andtime taking nature of this procedure discourages even the trainedsurgeons from doing DCR especially when the operative load ofcataract is high. This need urges for some modification in theconventional technique which could make it simpler, less traumaticand less time taking without compromising the success rate. The aim ofthis study is to evaluate and compare the outcomes of theconventional external DCR with suturing posterior and anteriormucosal flaps (H shaped) and the modified technique of creating andsuturing anterior flaps (Ushaped) only with respect to operative time,intraoperative complications and success rate.
Material and Methods:
A Prospective randomized comparative clinical study was undertaken atIndira Gandhi Institute of Medical sciences, Patna for one year duration,from June 13 to July14. After taking approval from the ethical committee of theinstitution, 96 patients, more than 20 years of age,with primary acquired NLD obstruction with orwithout mucocele were selected to undergoexternal DCR .Patients with secondary nasolacrimal ductobstruction,failed DCR,canalicular and punctal occlusion, lowereyelid deformity (entropion, ectropion or lid laxity),nasal mucosalpathology (atrophic rhinitis, lupus etc.),bleeding diathesis wereexcluded from the study. All the selected cases underwent thoroughanterior segment examination of each eye, with special emphasis on examination of lacrimal drainage system [puncta, swelling,tenderness, fistula, regurgitation on pressure over lacrimal sac(ROPLAS)] and eye lids. Fundus examination was performed for botheyes in every case. Lacrimal irrigation was done in all cases alongwith primary and secondary Jones dye test. ENT consultation to ruleout gross nasal mucosal pathologies and physician checkup for surgical fitness was obtained in all patients. The cases were randomly divided into two groups by a computer generated system , A & B with 47 and 49 patients respectively. Surgery was done under local anaesthesia. A curvilinear skin incision of 8-10 mm, corresponding to the anterior lacrimal crest was given, care being taken to avoid trauma to the angular vein. After bluntdissection of orbicularis and exposure of lacrimal sac, a 10 x 12 mmdiameter bony window was created taking care to preserve the nasalmucous membrane intact. It is necessary to remove the anterior lacrimal crest down to the entrance of the nasolacrimal duct. The landmarks of bony ostium were anteriorly up to 5 mm from theanterior lacrimal crest, posteriorly up to posterior lacrimal crest, superiorly up to the level of medial palpeberal ligament and inferiorly up to the beginning of nasolacrimal duct. The margins of osteotomy were made smooth. In group A a ‘H’shaped incision was made through the medial wall of the sac so as to form anterior and posterior flaps of the lacrimal sac. The nasal mucosa was incised in similar fashion along the upper and then the lower limit of the oval opening in its full diameter. In this manner two flaps of nasal mucous membrane were formed which were fashioned further by excising the extra edges. Both anterior and posterior flaps were sutured to their counter flaps with 6-0 vicryl. In group B, an U shaped incision was made in the nasal mucosa and the sac to create only a single flap with excision of the remaining tissue which were later anastomosed witheach other and then suspended to the orbicularis muscle to preventsagging. The surgical wound was closed in layers.Orbicularis musclewas closed with 3-4 interrupted 6/0vicryl sutures and the skin incision by interrupted 6/0 silk sutures and a firm pressure dressing was done after antibiotic ointment application. Postoperatively all patients were given oral and local antibiotics and nasal decongestants for one week. Follow-up examination was scheduled on the 1st, 7th postoperative day and thereafter 1st, 3rd and 6th months from the day of surgery. Skin sutures were removed on day-7 postoperatively. At each followup visit cases were examined for any complications such as wound gap, infection, granuloma formation, discharge, epistaxis etc. The surgical success was defined by anatomical patency of lacrimal drainage system on irrigation at final follow-up. Blocked syringing was considered as surgical failure. Statistical analysis was done using chi square test and Fisher’s exact test.
Results:
Epiphora with or without discharge was the most common presenting complaint. Chronic dacryocystitis accounted for 89% cases ,chronic dacryocystitis with mucocele for 7.5% and3.5% were diagnosed as encysted mucocele(Table 1)
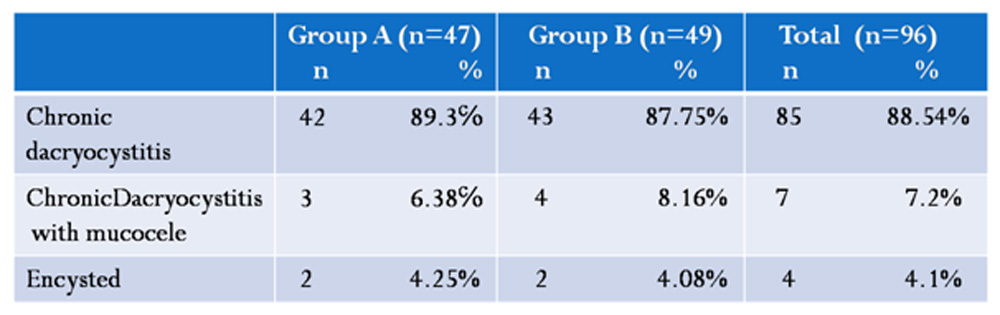
Table 1 Lacrimal system drainage disorders by Groups
In Group A mean age of the patient was 37.13 (±11.52) years with a range of (21- 60).In Group B, mean age of the patient was 37.37(±9.57) years with a range of (23 – 61) years. The age difference between the groups was not significant (t test= 0.111, p = 0.918) .
(Fig. 1).
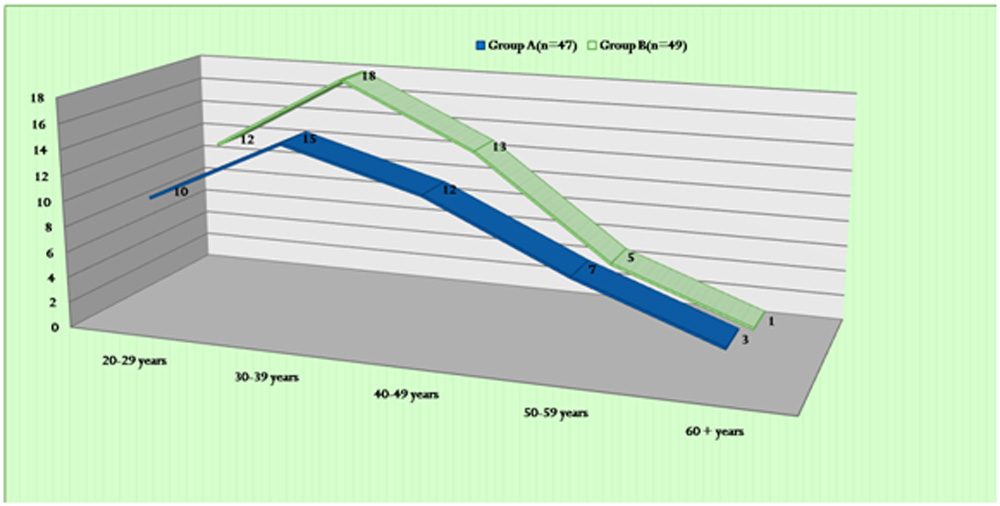
Fig.1 Age distribution, t test= 0.111, p = 0.918
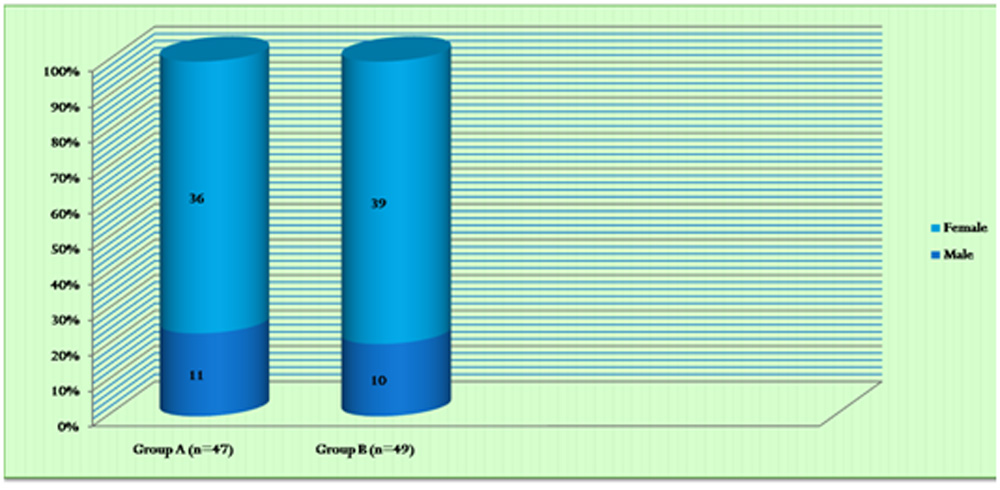
Fig. 2;Gender distribution.Both groups have similar gender distribution without significant difference (X² test=0.126; p=0.722)
By gender, themajority of treated patients 75 (78.12%) female, and 21 (21.87%) weremale. In the group A, 36(76.59%) patients were female and 11(23.40%) were male;while in the group B, 39 (79.59%) patients werefemale and 10 (20.40%) were male. Both groups have similar gender distribution without any statistically significant difference (X test=0,113; p=0,736) . (Fig.2)
Intraoperative haemorrhage was present in 5 cases (10.63%) in Group
A and 7cases (12.5%) in Group B (Table 2). Flap tear was present in 6cases(12.76%) in Group A and 4cases (8.16%) in Group B. The
difference in complications between the two groups was not statistically significant (X test=0.733 p=0.391).
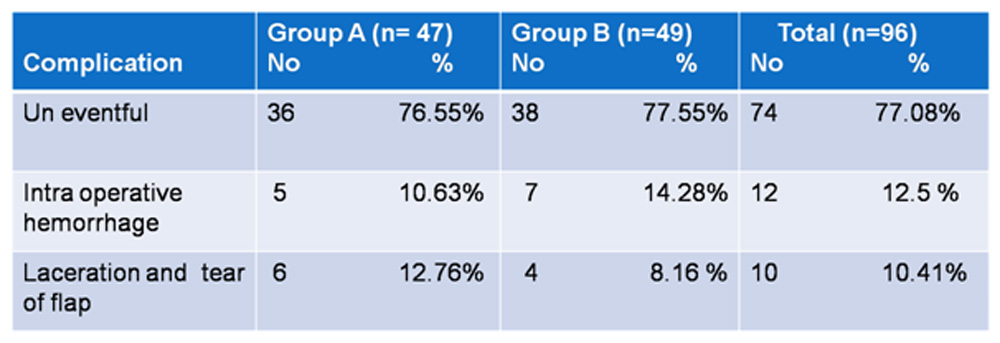
Table 2.Intraoperative complications in the two groups ,
(X test=0.733 p=0.391)
The overall rate of patency on lacrimal irrigationin external DCR was 94.79%. Of this success rate was 93.62% in group A and 95.91% in group B (Table 3). Recurrence of epiphora was present in 3 cases(6.38%) in Group A and 2 cases(4.08%) in Group B(Table 3).There was no statistically significant difference in success rate between the groups since the Fisher exact test statistic value was 0.674.
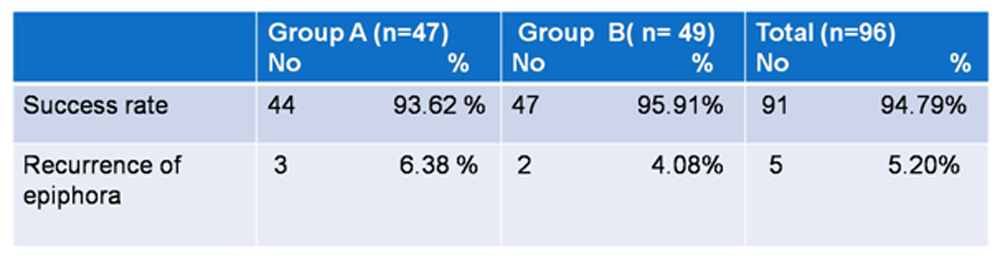
Table 3.Success rate in terms of patency and recurrence
Mean surgical time (calculated from skin incision to skin suture) in Group A was 52.14min and in Group B was 43.39 minutes. Average surgical time taken was 8.75 min less in single flap technique in comparison to double flap (t =7.2031, p= 0.01) which was statistically significant (Table 4). p=0.722).
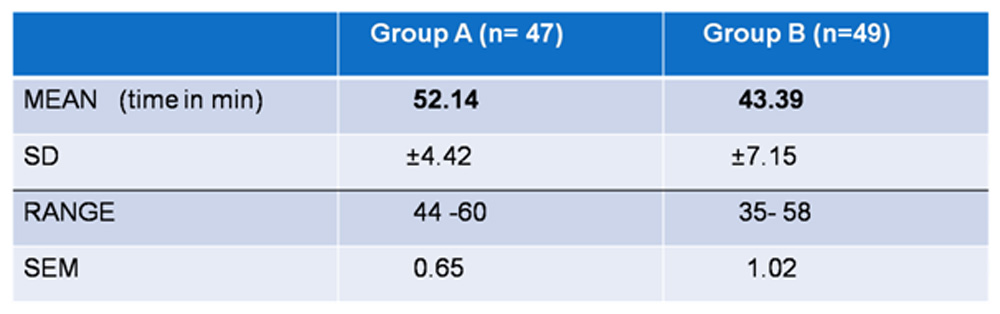
Table 4.Mean surgical time taken in the two groups.
Discussion
Nasolacrimal duct obstruction is more common in females in 4th
and 5th decade. According to Duke Elders the incidence of
dacryocystitis in females is 75% to 80% and 20% to 25% in males. Jorgeet al. states that narrow lacrimal fossa in females predispose them toobstruction by sloughed off debris, due to hormonal changes thatbring about a generalized de-epithelisation.[6]The mean age of study group in the present study was 37.25 years withstandard deviation of 10.58 years. Out of total 96 cases, females78.12% (75 cases) outnumbered males 21.8% (21) and the male:female ratio was 1:3.5. Our findings are in accordance with those ofDeka et al who observed mean age of 41 years with 8.4 years standard
deviation in their study of which 65% were females and 35% males. [7].
Similarly Kacaniku et al. reported mean age of the patients to be 44.6
years with 9.9 years standard deviation years, including 71% (37)females and 29% (15) males. The male: female ratio in their study wasalso 1:2.5 [8]. External dacryocystorhinostomy is a highly successful procedure inmanaging epiphora due to nasolacrimal duct obstruction [9].The reported success rate varies between 85% to 99%(Table 4) .However, surgical procedure is not technically easy and requiresconsiderable experience as well as operative time. Meticulousattention to atraumatic handling of the soft tissues, a clear, properlyplaced and uniform rhinostomy with smooth edges, careful dissection to expose the true lumen of the lacrimal sac, followed by careful suturing of mucosal flaps, are important determinants of the outcome of the surgery. Moreover, individual response to tissue healing process is also an important factor for a successful DCR
surgery[10]. In the present study, the overall surgical success of external DCR was 94.79 %. Shun-Shin et al in their study combined the results of a total of 799 cases and showed an overall success rate of 91% for primary external DCR which isaccordance with this study.[11].
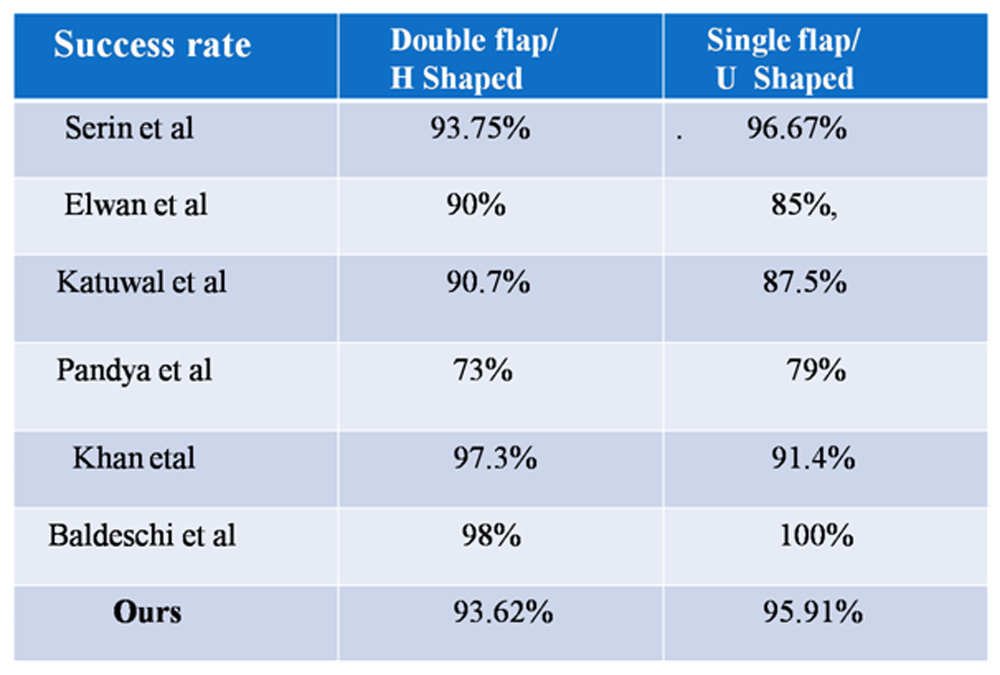
Table-5; Comparison of success rate of external DCR in different
studies
In current study 93.62 % and 95.91% cases had favourable surgical outcome that were patent on lacrimal irrigation, in group A and group B respectively (Table-3). The difference between the two was statistically insignificant (p>0.05) which is in accordance with several other studies as shown in the Table-5. The difference in the success rate could be attributed to difference in sample size and different surgeon in different studies. However, Welham et al and Kansu et al have advocated that, both anterior and posterior mucosal flaps should be sutured, as this increases the probability of primary healing of the mucosal anastomosis and the tendency of primary and
secondary haemorrhages and formation of granulation tissue is reduced [12,13].In our study we found intraoperatively bleeding in 4 cases (5%) , and nasal mucosal tear in 2 (2.5%) cases. The difference in complications in both groups was statistically insignificant (p=1.0). Kacaniku et al reported intraoperative bleeding in 3(5.8%) cases and laceration of the nasal mucosa in 2(3.8%) cases with statistically insignificant difference in their study groups which is in accordance with our study [8]. Most common post-operative complications were epistaxis and periorbital ecchymosis in 4 cases and 2 cases respectively in both the groups. The difference in complications in both groups was statistically insignificant (p=0.61). Deka et al reported five cases (3 cases of epistaxis and 2 cases of periorbital ecchymosis) with postoperative complications in their study. [7] Other complicationswere postoperative infection, canaliculitis, suture granuloma andwound gap one case each. This variation in types of complicationscould be attributed to individual response to tissue healing processrather than surgical intervention. Mean surgical time taken in our study in Hshaped flap technique was52.14± 4.42 min and in U shaped technique was 43.39± 7.5 min ,the difference being clinically significant .This result is in consistencewith a similar study done by Agrawal et al. [14] Although they had more success rate with H shaped flaps in contrast to ours but the difference between the two groups was not significant as in ours. The overall surgical failure of external DCR was 10% in our study being 12.5% in group A and 7.5% in group B. All cases had non patent lacrimal irrigation between 7th postoperative day and 4 weeks. Similar observations were made by Walland et al who reported a [15]. failure rate for primary surgery as 12% However failure rates ranging from 0 to 18% have been reported in several other studies [11,13,14]. These differences in failure rates with external DCR can beattributed to many factors including position and size of the ostium,common canalicular obstruction, scarring within the anastomosisdue to infection or non-absorbable suture material, persistent mucocele, and the SUMP syndrome[16].The surgical outcomes of both procedures were comparable in thisstudy. Safe handling of posterior flap in double flap surgery inconstrained anatomical field is difficult. Single (anterior) flap DCR isa safe, easy to master and effective surgical procedure for relievingepiphora without any significant intraoperative and postoperative complications.
Conclusion;
Our study suggests that external dacryocystorhinostomy with suturing anterior and posterior flaps has no advantage over excision of the posterior flaps and suturing only anterior flaps with tenting it to orbicularis muscles .Later procedure is relatively easier to perform with lesschances of flap tears and takes significantly less time.
References:
- Duke-Elder S ed. System of Ophthalmology part II. 2nd ed. London: HeneryKimpton publishers;1974:568-718
- Toti A. Nuovo metodo conservatore di cura radicale delle suporazioni chroniche del sacco lacrimale. Clin Mod Firenze. 1904;10:385–389
- Hart RH, Powrie S, Rose GE. Primary External Dacryocystorhinostomy.In: Cohen AJ, Mercandetti M, Brazzo BG. ed. e Lacrimal System. New York, Springer, 2006: 127.
- H. Emmerich, H. Busse, H.W. Meyer- Rusenberg Dacryocystorhinostomia externa. Technique, indications and resultsOphthalmologe, 91 (3) (1994), pp. 395–398
- K.J. Tarbet, P.L. Custer External dacryocystorhinostomy: surgical success, patient satisfaction and economic cost Ophthalmology, 102 (7) (1995), pp. 1065–107011.
- Jorge GC, Alfanso UB. Nasolacrimal duct obstruction e medicine feb 9 2012; URL:https://emedicine.medscape.com/article/1210141-overview#a0104
- DekaA, Saikia SP, BhuyanSK. Combined posterior flap and anterior suspended flap dacryocystorhinostomy: A modification of external dacryocystorhinostomy. Oman J Ophthalmol. 2010;3:18–20.
- Kacaniku G, Spahiu K, Hoxha G. Anterior flapanastomosis in external dacryocystorhinostomy.Med Arh.2011;65:32-34
- Tarbet KJ, Cluster PL. External dacryocystorhinostomy: Surgical success, patient satisfaction and economic cost. Ophthalmoloy. 1995;102:1065-1070.
- Deka A, Bhattachajee K, Bhuyan SK, Barua CK, Bhattacherjee H, Khaund G. Effect of mitomycin C on ostium in dacryocystorhinostomy. Clin Experiment Ophthalmol.2006;34:557-61
- Shun-Shin GA, urairajan G. External dacryocystorhinostomy-an end of an era? Br J Ophthalmol. 1997;81:716-717
- Welham RAN, Wulc AE. Management of unsuccessful lacrimal surgery. Br J Ophthalmol. 1987;71:152-157.
- Kansu L, Aydin E, Avci S, Kal A, Gedik S. Comparison of surgical outcomes of endonasal dacryocystorhinostomy with or without mucosal flaps. Auris Nasus Larynx. 2009;36:555-559
- Agrawal RK,Behera S,Sahoo S.A comparative study of external dcr using single flap, double flap and intracystic implant (pawar) dacryocystorhinostomy techniques.Yuva Journal of Medical Science Vol 2, No 1, January 2016, pg.12-22 eISSN: 2395-6526
- Walland M, Rose G. Factors affecting the success rate of open lacrimal surgery. Br J Ophthalmol. 1994;78:888-891
- You YA, Fang CT. Intraoperative mitomycin C in dacryocystorhinostomy. Ophthal Plast Reconst Surg. 2001;17:115–119.
Leave a Comment