
Dr. Vandna Sharma ( V19433 )
INTRODUCTION
Ocular morbidities include wide range of conditions like refractive errors, infectious eye diseases, ocular trauma, vitamin A deficiency (VAD), color blindness and allergic eye diseases. Majority of these conditions are either potentially preventable or curable if early attention through eye screening is given1.
Visual impairment at birth or during childhood can affect communication, employment, health, quality of life and the effects are lifelong2. Childhood blindness is among the commonest cause of blind-person-years, as the number of years lived with blindness by blind children is almost the same as the total number of blind years due to age related cataract3. Moreover it is estimated worldwide that the cumulative number of blind-person-years due to childhood blindness ranks second after cataract blindness4. So the economical, psychological and social consequence of childhood blindness is manifold.
With increasing number of children going blind every year, there has been a fact quoted by World Health Organization (W.H.O.) that “Every minute a child goes blind” which reflects the ever increasing global burden of childhood blindness5. Though proportion of infants and school aged children with visual impairment is less than 5 % worldwide, yet they account for 20% of individuals with visual impairment after adjusting disability adjusted life years (DALYS) 6. That is why prevention of childhood blindness is a priority of the W.H.O.’s VISION 2020 Programme3. The Right to Sight a global initiative has been launched in 1999, as a joint programme between W.H.O. and International Agency for Prevention of blindness (IAPB). This programme aims to eliminate avoidable blindness like cataract, xerophthalmia, refractive errors, trachoma and other causes of childhood blindness by the year 20207.
The available data suggest that difference in prevalence of childhood blindness between the wealthiest and the poorest countries of the world may be fifteen fold, ranging from as low as around 0.1 per 1000 children aged 0-5 years in high economic nations to 1.5/1000 children in low economic nations8. If this correlation is used to estimate the prevalence of blindness in children, the number of blind children in the world is estimated to be 1.4 million. According to W. H. O. statistics, approximately three-quarters of the world’s blind children live in the poorest regions of Africa and Asia, where the prevalence is high3.
School going children in India are susceptible to various types of ocular morbidities. Blindness is one of the most significant social problems in India. A national survey on blindness 2001-2002 showed that 7% of children aged 10-14 years have problems with their vision9. Considering the fact that 30% of India’s blind lose their eyesight before the age of 20 years and majority of them are under five when they become blind. So the importance of early detection and treatment of ocular diseases and visual impairment among young children is obvious10.
Children having ocular problems would rarely complain to their parents. Sometimes the parents are also ignorant about the need to get their child examined by the ophthalmologist. Some of the conditions like VAD, allergic conjunctivitis, vernal keratoconjunctivitis (VKC) and eyelid infections, if left undetected may be precursors to more serious eye diseases like corneal ulceration. Also it is imperative to tackle causes of ocular morbidity on an urgent basis as children can develop amblyopia unlike adults11.
A child with visual impairment finds schooling and various other activities extremely difficult. They adjust to their poor vision by holding books close to the face, sitting close to black board in classroom, blinking excessively and frequent rubbing of eyes. So this affects learning ability, performance and adjustment in school, and overall development of a child. Later on, it may have a negative impact on social health and employment opportunities. In competitive world of today, good physical and mental health is indispensable. To get employment in certain fields like navy, military, railways and aviation good visual acuity is essential. So the effective methods of vision screening in school children are useful in detecting correctable causes of decreased vision, especially refractive errors and in minimizing long-term visual disability4, 10.
However, there is scarce information about magnitude of childhood ocular morbidities in Himachal Pradesh. In a study done by Gupta et al, children of age group between 6-16yrs were studied during the year 2001-2002 in Shimla4. Moreover there has been a substantial improvement in healthcare services in the state. The present study is of great importance as it has provided valuable data on prevalence of childhood ocular morbidity in this part of country.
AIMS AND OBJECTIVES-
To study the prevalence and pattern of ocular morbidity in primary school going children from age group 5-11yrs in Kangra district, Himachal Pradesh.
MATERIALS AND METHODS
Study design: Cross-sectional study.
Setting: All primary coeducational schools, both government and private functional in Kangra block were enlisted. Out of this list two government primary schools and two private schools were selected randomly from each category of schools. In case requisite sample size was not achieved in the randomly selected schools then adjacent school /schools were visited for completion of sample size.
Sample size: Based on the preliminary data from previously described studies, ocular morbidity prevalence was estimated to be about 30%. Based on this, required sample size was calculated by formula 4PQ/L2, came out to be 933. Where P=30% (prevalence), Q=100-P, L=10% of P (allowable error). In this study a total 1007 students were included.
Study duration: One year.
Study tool: Pretested semi structured interview cum examination proforma was used.
Inclusion criterion: All school going children of age group 5-11 years were included.
Exclusion criteria: Children whose guardians did not give consent for detailed examination. After taking permission from the Institutional ethical committee, Principals of identified schools were informed about the study and permission was taken .They were also informed before each visit. All study subjects were interviewed after getting written informed consent from the teacher/parent/guardian. First part of proforma included demographic information, ocular complaints if any and school performance. Second part of it included the preliminary ophthalmic examination for diagnosing ocular morbidity. Preliminary examination module in schools
1. Visual acuity test: with the help of Snellen’s vision chart. The vision was taken unaided, with available glasses and with pinhole.
2. Assessment of extra ocular movements.
3. Cover-uncover tests.
4. Color vision test with Ishihara color plates.
5. Diffuse light examination with a torch light.
6. Undilated fundus examination was done.
All the study subjects were clinically examined with torch-light. Those who required special examination process were advised to come to department of ophthalmology, Dr. Rajendra Prasad Government Medical College, Tanda where further evaluation and appropriate treatment was given with consent of parents or guardians.
Detailed ocular examination module in Department of ophthalmology, Dr. R. P. Govt. Medical College, Tanda
1. Visual acuity test: with the help of Snellen’s vision chart.
2. Assessment of extra ocular movements.
3. Cover-uncover tests.
4. Anterior segment examination using slit-lamp bio-microscope (Haag Streit BM 900).
5. Retinoscopy and subjective refraction.
6. IOP was recorded by Applanation Tonometer wherever suspicion of high IOP was there.
7. Cycloplegic refraction followed by subjective verification of refraction.
8. Detailed fundus examination using Heine beta 200s ophthalmoscope.
9. Ancillary investigation was done whenever indicated.
The principal cause of ocular morbidity was assigned after completion of the ocular examination and major cause of ocular morbidity was noted. Refractive error was recorded as the cause of visual impairment in eyes improving to 6/9 or better with refractive correction. Children needing medical or surgical treatment were evaluated accordingly.
OBSERVATIONS
| NO. OF CHILDREN | SCHOOLS GOVERNMENT PRIVATE |
Total
|
|
| MALE | 217 (44.3%) | 273 (55.7%) | 490 |
| FEMALE | 289 (55.9%) | 228 (44.1%) | 517 |
| TOTAL | 506 (50.2%) | 501 (49.8%) | 1007 |
This study included 48.7% males and 51.3% female going children. Almost equal number of children from government schools (50.2%) and private schools (49.8%) were screened in the study.
Table 2- Gender wise distribution of children across age-groups.
| No. Of Children | |||
| Age Group | Male | Female | Total |
| 5-7yrs | 112(49%) | 117(51%) | 229 |
| 7-9yrs | 182(45%) | 220(55%) | 402 |
| 9-11yrs | 156(50%) | 153(50%) | 309 |
| 11-12yrs | 40(60%) | 27(40%) | 67 |
| Total | 490(48.7%) | 517(51.3%) | 1007 |
In all age groups, male and female had equal presentation except in 11-12years age group males were more (60%) than females (40%).
Table 3- Prevalence of ocular morbidity.
| NORMAL | OCULAR DISEASES | |
|
NO. OF CHILDREN (PERCENTAGE) |
763 (75.8%)
|
244 (24.2%)
|
The overall prevalence of ocular morbidity among primary school going children of age group 5-11 years in district Kangra was 24.2 %.
Table 4– School wise distribution of ocular morbidity.
|
NO. OF CHILDREN |
|||
| SCHOOLS | NORMAL | OCULAR DISEASE | Total |
|
GOVERNMENT |
361 (71%) | 145 (29%) | 506 |
| PRIVATE | 402 (80%) | 99 (20%) | 501 |
| TOTAL | 763(76%) | 244 (24%) | 1007 |
|
Chi-square =10.851 p value=< 0.001 Highly Significant |
|||
There was significant difference in ocular morbidity between government and private school going children. It was higher (29%) in government school going children as compared to 20% in private schools going children.
Figure 1- Gender wise distribution of ocular morbidity.
There overall prevalence of ocular morbidity was almost similar in both genders. It was found to be 24.17% in males and 24.28% in females.
Table 5- Prevalence of ocular morbidity among male and female children of government and private schools.
| (NO. OF CHILDREN) | MALES
|
FEMALES
|
||||
| SCHOOLS | NORMAL | OCULAR DISEASES | TOTAL
|
NORMAL | OCULAR DISEASES | TOTAL |
| GOVERNMENT | 149 | 68 | 217 | 212 | 77 | 289 |
| PRIVATE | 222 | 51 | 273 | 180 | 48 | 288 |
| TOTAL | 371 | 119 | 490 | 392 | 125 | 517 |
| Chi-square=10.530
p value=<0 .001( Highly Significant) |
Chi-square =2.173
p value=>0.140 (Not Significant) |
|||||
There was statistically significant difference in prevalence of ocular morbidity among male children in government & private schools. It was more among male children in government schools (38.3%) as compared to those of private schools (18.6%). Whereas, this difference in prevalence of ocular morbidity was not significant among female children of government schools (26.6%) and private schools (21%).
Figure 2- School wise distribution of ocular morbidity among male and female group.
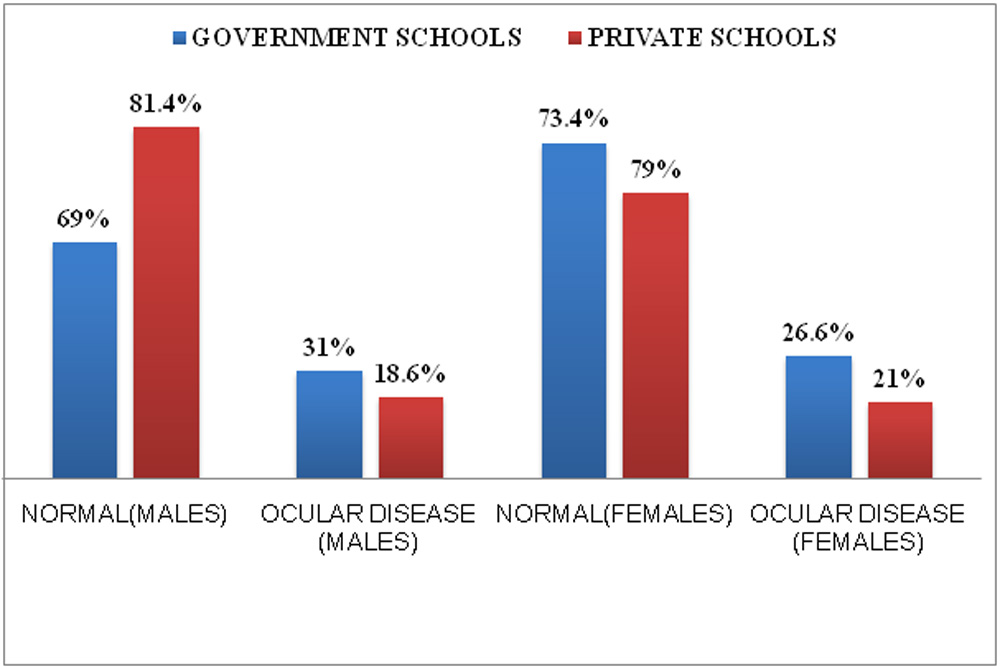
Table 6- School wise distribution of ocular morbidity among children of age group 5-9 yrs and 9-11yrs.
| NO. OF AGE GROUP
CHILDREN) |
(5-9 yrs) |
AGE GROUP
(9-11 yrs) |
||||
| SCHOOLS | NORMAL | OCULAR DISEASES | TOTAL | NORMAL | OCULAR DISEASES | TOTAL |
| GOVERNMENT | 252 | 106 | 358 | 109 | 39 | 148 |
| PRIVATE | 221 | 52 | 273 | 181 | 47 | 228 |
| TOTAL | 473 | 158 | 631 | 290 | 86 | 376 |
| Chi-square = 9.204
p value=<0.002 (highly significant) |
Chi-square =1.675
p value=>0.196 not significant |
|||||
There was significant difference in prevalence of ocular morbidity in government & private schools going children of age group 5-9yrs. It was found to be higher (30%) in government schools going children in comparison to 19% in private schools.
Table 7- Age wise distribution of ocular morbidity in government & private schools.
| OCULAR DISEASES
( No. of children and percentage) |
|||
| AGE | GOVERNMENT
SCHOOLS |
PRIVATE
SCHOOLS |
P-VALUE |
| 5-6yrs | 20(32.3%) | 2 (40%) | 0.723 |
| 6-7yrs | 28(30.8%) | 12(17%) | 0.042* |
| 7-8yrs | 27(25.5%) | 15(19%) | 0.319 |
| 8-9yrs | 31(31.3%) | 23(19%) | 0.041* |
| 9-10yrs | 22(26.2%) | 25(20%) | 0.308 |
| 10-11yrs | 9(22.5%) | 13(21%) | 0.887 |
| 11-12yrs | 8(33.3%) | 9(21%) | 0.263 |
*Significant P-value
There was significant difference in prevalence of ocular morbidity in government and private schools in age groups 6-7 years and 8-9 years.
Table 8- Pattern of ocular morbidity in school children in age group 5-11yrs.
| OCULAR DISEASES | NO.OF CHILDREN
N=1007 |
PERECENAGE |
| 1. REFRACTIVE ERROR | 128 | 12.8% |
| 2. VITAMIN A DEFICIENCY | 26 | 2.6% |
| 3. ALLERGIC CONJUNCTIVITIS* | 26 | 2.6% |
| 4. VKC* | 24 | 2.4% |
| 5. AMBLYOPIA | 23 | 2.3% |
| 6. EYELID CONDITIONS | 21 | 2.1% |
| 7. SQUINT | 19 | 1.9% |
| 8. CONGENITAL ANOMALIES | 13 | 1.3% |
| 9. INFECTIVE CONJUNCTIVITIES* | 11 | 1.1% |
| 10. PTOSIS | 4 | 0.4% |
| 11. OTHER DISEASES | 4 | 0.4% |
| 12. COLOUR BLINDNESS | 26 | 2.6% |
* Conjunctivitis (6%)
(Including VKC, Allergic conjunctivitis & infective conjunctivitis)
In the present study refractive errors were detected in 12.8%, vitamin A deficiency, allergic conjunctivitis and colour blindness in 2.6% each, VKC, and amblyopia in 2.4% each, eyelid diseases (blepharitis, chalazion, stye) in 2.1%, squint in1.9%, congenital anomalies in 1.3% , infective conjunctivitis in 1.1% , ptosis in 0.4%, and miscellaneous eye disorders in 0.4% . In this study, out of total 244 children with ocular disease, 43 (17%) children had more than one ocular disease.
Figure 3- Pattern of ocular morbidity in primary school children in age group 5-11yrs in district Kangra.
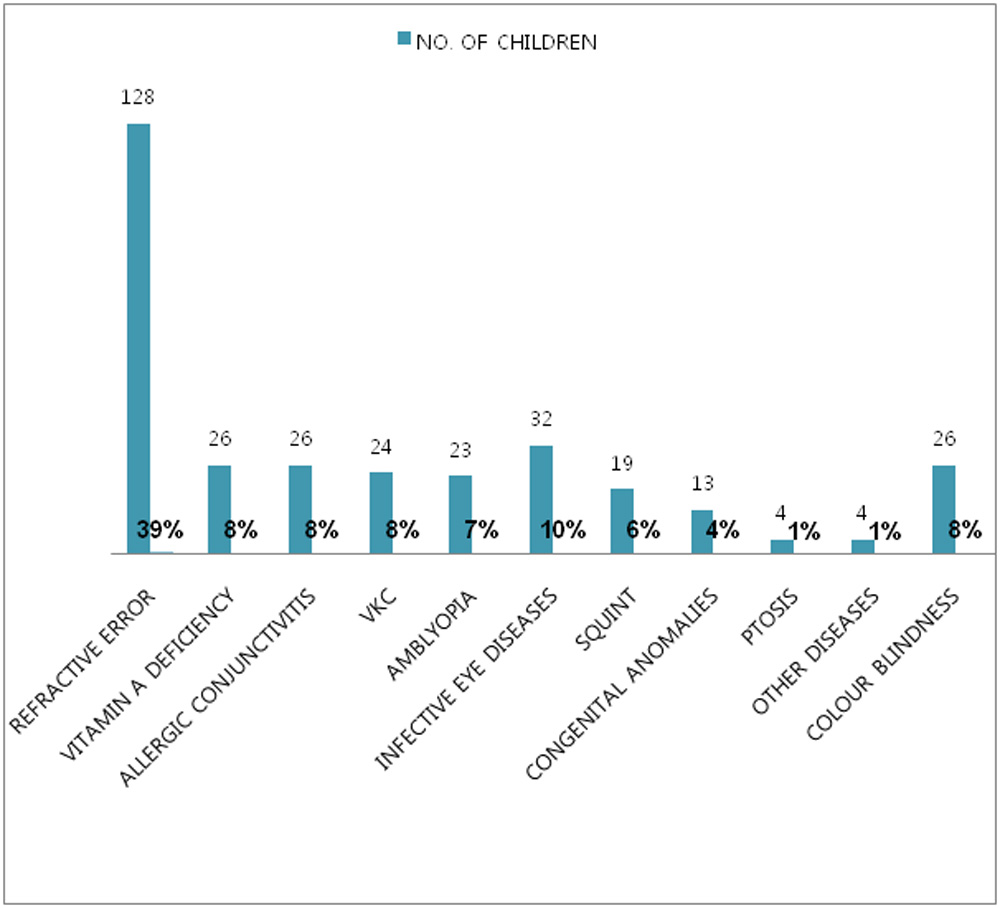
Refractive errors were major cause of ocular morbidity accounting 39% of total ocular morbidity, followed by infective eye diseases (including eyelid diseases and infective conjunctivitis) contributing 10% and rest were vitamin A deficiency, allergic conjunctivitis, VKC and colour blindness (8%) each, amblyopia (7%), squint (6%), congenital anomalies (4%), ptosis (1%), and miscellaneous eye disorders (1%).
Table 9 – School-wise distribution of ocular diseases.
| SCHOOLS | |||
| OCULAR DISEASES | GOVERNMENT
N=506 |
PRIVATE
N=501 |
P-VALUE |
| AMBLYOPIA | 14(2.8%) | 9(1.8%) | 0.303 |
| REFRACTIVE ERROR | 62(12%) | 66(13%) | 0.661 |
| SQUINT | 14(2.8%) | 5(1%) | 0.039* |
| VKC | 14(2.8%) | 10(2%) | 0.423 |
| EYE LID CONDITIONS | 18(3.6%) | 3(0.6%) | 0.001* |
| ALLERGIC CONJUNCTIVITIS | 17(3.4%) | 9(1.8%) | 0.118 |
| CONGENITAL MALFORMATION | 10(2%) | 3(0.6%) | 0.053 |
| PTOSIS | 2(0.4%) | 2(0.4%) | 0.992 |
| VITAMIN A DEFICIENCY | 25(5%) | 1(0.2%) | 0.000* |
| INFECTIVE CONJUNCTIVITIS | 9(1.8%) | 2(0.4%) | 0.035* |
| OTHER DISEASES | 1(0.2%) | 3(0.6%) | 0.312 |
*Significant P-value
Results showed that prevalence of refractive errors in government school children (12%) and in private school children (13%) was almost similar. However, the prevalence of vitamin A deficiency was more (5%) among children of government schools in comparison to private schools (0.2%). Similarly, prevalence of eyelid diseases was higher (3.6%) in government school children in comparison to 0.6% in private schools, which was statistically significant.
Moreover, prevalence of conjunctivitis (including VKC, allergic & infective conjunctivitis) was also significantly higher (8%) among government school children as compared to private school children (4%) with p-value<0.014 .The prevalence of rest of ocular morbidities did not vary significantly with type of school. Different pattern of ocular diseases was observed in government and private schools leading to significant difference in overall prevalence of ocular morbidity.
Figure 4 – School wise distribution of ocular morbidities.
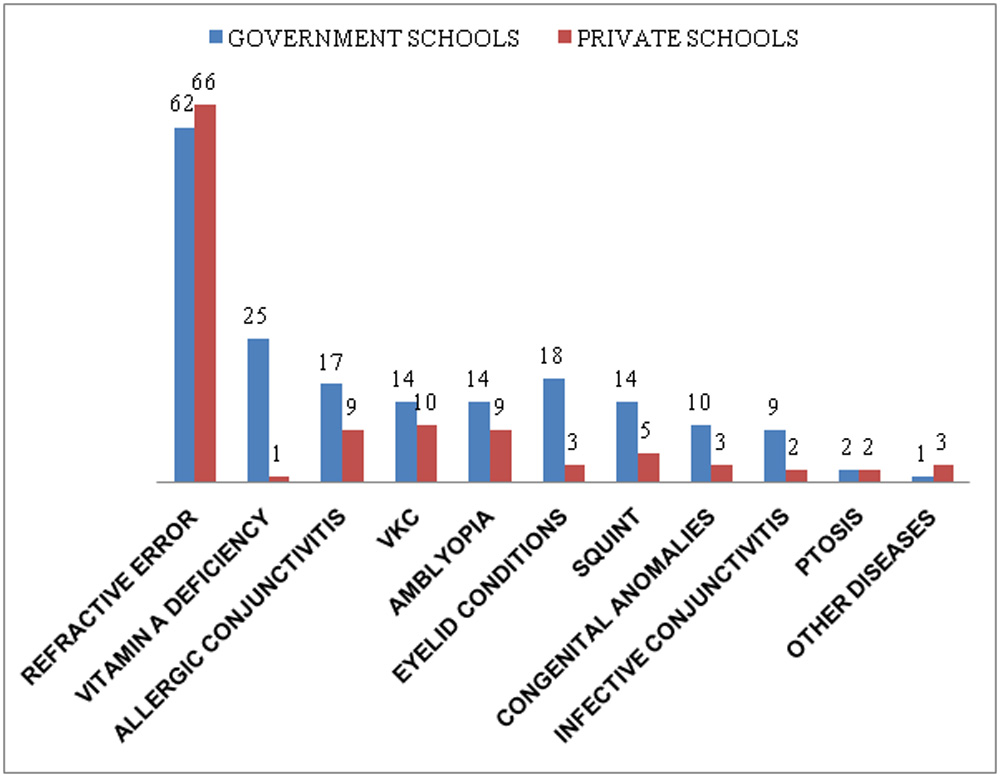
Table 10- Gender wise distribution of ocular diseases.
| OCULAR DISEASES | MALE
N=490 |
FEMALE
N=517 |
P-VALUE |
| REFRACTIVE ERRORS | 54(11%) | 74(15%) | 0.332 |
| ALLERGIC CONJUNCTIVITIS | 13(2.6%) | 13(2.6%) | 0.89 |
| VITAMIN A DEFICIENCY | 13(2.6%) | 13(2.6%) | 0.89 |
| VKC | 24(4.9%) | 0 | 0.00* |
| AMBLYOPIA | 11(2.2%) | 12(2.4%) | 0.936 |
| SQUINT | 9(1.8%) | 10(2.0%) | 0.91 |
| CONGENITAL MALFORMATION | 8(1.6%) | 5(1%) | 0.350 |
| INFECTIVE CONJUNCTIVITIS | 3(0.6%) | 7(1.4%) | 0.235 |
| STYE | 4(0.8%) | 7(1.4%) | 0.412 |
| BLEPHARITIS | 1(0.6%) | 6(1.2%) | 0.355 |
| CHALAZION | 1(0.2%) | 2 (0.4%) | 0.343 |
| PTOSIS | 0 | 4(0.8%) | 0.51 |
| OTHER DISEASES | 2(0.4%) | 2(0.4%) | 0.957 |
| COLOR BLINDNESS | 26(5%) | 0 | 0.000* |
*Significant P-value
There was no gender difference for overall prevalence of ocular morbidity. However, VKC (4.9%) and colour blindness (5%) were prevalent only in male children. The prevalence of refractive errors, lid diseases and infective conjunctivitis were slightly more in females then males but that was not significan
Table 11- Best corrected visual acuity (BCVA) in the better eye in Snellen’s notation.
| NO. OF CHILDREN | PERCENTAGE | |
| Group 1-6/6 -6/18 | 999 | 99.9% |
| Group2- <6/18-6/60
|
1 | 0.1% |
Majority of primary school children had visual acuity in normal range 6/6 -6/ 18 in either eye. Whereas, one child (0.1%) had moderate visual impairment with visual acuity in range <6/18-6/60 and none had severe visual impairment with vision in range <6/60-3/60.
Table 12- Association of myopia and hyperopia with age.
| AGE | MYOPIA | HYPERMETROPIA | TOTAL |
| 5-6yrs | 4 | 8 | 12 |
| 6-7yrs | 3 | 19 | 22 |
| 7-8yrs | 2 | 22 | 24 |
| 8-9yrs | 10 | 18 | 28 |
| 9-10yrs | 6 | 19 | 25 |
| 10-11yrs | 1 | 6 | 7 |
| 11-12yrs | 7 | 3 | 10 |
| TOTAL | 33 | 95 | 128 |
| P-Value = 0.006 (Highly significant) | |||
Higher prevalence of refractive errors in younger age group (5-9years) was seen because there was high prevalence of age-related hypermetropia (10%) in young children. This association was found to be statistically significant.
Table 13- School-wise distribution of children with corrected and uncorrected refractive error (R.E.).
| NO. OF CHILDREN | |||
| SCHOOLS | CORRECTED R.E. | UNCORRECTED R.E. | TOTAL |
| GOVERNMENT | 5 | 57 | 62 |
| PRIVATE | 14 | 52 | 66 |
| TOTAL | 19 | 109 | 128 |
| p-value = 0.037 | |||
Results suggested that 19 (15%) children had already corrected refractive error with glasses as compared to 109 (85%) children with uncorrected refractive error.
Table 14- Gender wise distribution of infective eye diseases in government and private schools.
| INFECTIVE EYE DISEASES | GOVERNMENT
N=506 |
PRIVATE
N=501 |
|||||
| MALE | FEMALE | TOTAL | MALE | FEMALE | TOTAL | TOTAL
N=1007 |
|
| BLEPHARITIS | 1 | 4 | 5 | 0 | 2 | 2 | 7 |
| STYE | 3 | 7 | 10 | 1 | 0 | 1 | 11 |
| CHALAZION | 1 | 2 | 3 | 0 | 0 | 0 | 3 |
| INFECTIVE CONJUNCTIVITIS | 1 | 8 | 9 | 2 | 0 | 2 | 11 |
| TOTAL | 6 | 21 | 27
|
3 | 2 | 5
|
32
|
| p- value=0.748 | p-value =0.082 | ||||||
| Infective eye diseases Males = 1.2% , Females = 4.2% P-value=<0.018(significant) | |||||||
| Government schools= 5%, Private schools= 1% P-value=0.000 (highly significant) | |||||||
Total prevalence of infective eye diseases was 3.2%. It was second most cause of ocular morbidity. It included infective conjunctivitis, blepharitis, chalazion and stye, which were seen in 1.1%, 0.7%, 0.3% and 1.1% children respectively. It was significantly higher (5%) in government school children as compared to 1% in private school children. Similarly, it was more significant (4.2%) among females in comparison to (1.2%) in males.
Table 15- Relation between school performance and ocular morbidity.
| SCHOOL PERFORMANCE
(NO. OF CHILDREN) |
||||
| GOOD | AVERAGE | POOR | TOTAL | |
| NORMAL | 314 | 337 | 112 | 763 |
| OCULAR DISEASE | 77 | 117 | 50 | 244 |
| TOTAL | 391 | 454 | 162 | 1007 |
| P-value = 0.021(significant) | ||||
In this study, school performance was significantly affected by ocular diseases. Majority of children (45.1%) with ocular diseases had average school performance. Moreover, 16.1 % children with ocular diseases had poor school performance. Whereas, 38.8% of children’s school performance was not affected by ocular diseases.
DISCUSSION
Eyes are the most treasured organs of a human being. Although vision is very important for all ages but it is more so in case of children as it plays a key role in their mental, physical and psychological development1. Screening school children is arguably the second largest national programme for control of blindness in India after cataract surgery. It is one of the top priority programmes of the education initiative of the government (The Sarva Shiksha Abhiyan). However, studies pertaining to school screening programmes in India is scarce, especially when compared to evidence for initiatives addressing age-related cataract12. The present study was conducted to determine the prevalence and pattern of ocular morbidity among primary school going children in Kangra district of Himachal Pradesh.
Kangra is the most populous district, situated in western part of Himachal Pradesh. According to 2011 census, district Kangra had a population of 1,510,075; of which male and female were 750,591 and 759,484 respectively. Population of Kangra district living in rural and urban region is 94.29% and 5.71% respectively as per census 201113.
A total 1007 children of government and private schools were screened in present study. It included 506 children of 14 government schools and 501 children of 3 private schools with 48.65% males and 51.34% females. The overall prevalence of ocular morbidity among school going children from age group 5-11 years is 24.23 % in present study, which is lower than the prevalence reported by Gupta et al4 in Shimla (31.6%) in age group 6-16yrs and by Chaturvedi et al14 in Delhi (40%) in age group 5-15 years. Similarly, higher prevalence of ocular morbidity was also reported from neighboring states like Haryana (58.8% in 4-18 years) 15, Rajasthan (71.7% in 4-16 years) 10, and from Hyderabad in South India (43.5% in 3-16 years) 16. This difference was due to higher prevalence of trachoma and conjunctivitis in these two northern states and that of refractive errors in South India10, 15, 16. Lower prevalence (15%) of ocular morbidity was reported from Kolkata, West India among school children of 5-13 years because of small age group and low prevalence of refractive errors (2%) 17. These differences in ocular morbidity may be due to difference in examination method and diagnostic criteria used by various studies.
As per result of current study, majority of primary school going children had visual acuity in normal range 6/6 -6/18. Only one child (0.1%) had moderate visual impairment with visual acuity in range <6/18-6/60 in better eye, which was much lower than observed in the study conducted by et al18 in rural Delhi, who reported vision < 6/60 in 0.93% children. However, this result of present study is comparable to similar studies conducted among rural and urban school-aged children from other parts of India8, 14, 16
Various studies done in India and other developing countries quoted the spectrum of various types of refractive disorders as leading cause of visual impairment in school-going and school-aged children 8,16,19. Similarly in this study, prevalence of refractive error was most common cause of ocular morbidity, seen in 12.8 % children (Table-11), which is higher than the study conducted by Gupta et al 20 in U.P., and Kumar et al21 in Delhi, who reported prevalence 6.8% and 5.4% respectively. In contrast, the study done by Biswas et al22 in West Bengal found higher prevalence of refractive errors (23%). Similarly, higher prevalence of refractive errors has been observed among school children in Shimla and Ahmadabad studies4, 23.
The current study showed prevalence of squint in 1.9% children, which is comparable to the study done by Shrestha et al 24 in Kathmandu valley, who noted prevalence in 1.3% children. In comparison to present study, higher prevalence of squint was reported from previous studies conducted in North India by Pratap et al25 and by Gupta et al4, who observed the prevalence 2.8% and 2.5% respectively. Similarly, studies conducted in West Bengal and Delhi also observed higher prevalence of squint (7.4% in 5-15 years) than the current study14, 17. Whereas, lower prevalence was found by Desai et al10 in Rajasthan (0.2%) and Khurana et al15 in Haryana (0.6%) in 4-18 years age group. Studies done abroad by Wedner et al26 also revealed lower prevalence of squint (0.5%) among children of 7-19 years in Tanzania, Africa.
In the present study prevalence of amblyopia was found to be 2.3% which is much higher than reported from other studies24, 26. The most common cause for amblyopia noted by these studies was refractive error. In our study, it was found to be more (2.8%) among students of government schools than private schools (1.8%). This may be due to more aware parents of private school going children than parents of government school going children.
Infective eye disorders were second most common cause of ocular morbidity in current study, contributing 10% of total ocular morbidity. It included infective conjunctivitis, blepharitis, stye and chalazion (Table-19). Higher prevalence (3-17.5%) of conjunctivitis has been reported from various parts of India 10,15,17,25. In our study, higher prevalence of infective conjunctivitis (1.8%) in children studying in government schools as compared to private schools (0.4%) was observed. This finding is similar to that has been seen in the study conducted by Gupta et al4 in Shimla (1.5% among children of government schools as compared to 0.1% in children of private schools). The study conducted by Kumar et al27 in rural Delhi and by Singh et al28 in Patiala city, observed prevalence of conjunctivitis of 4.6% and 3.27% respectively, whereas present study reported higher prevalence of conjunctivitis (6%). Similarly, lower prevalence (1.5%) of conjunctivitis has been reported by Robinson et al21, among children of 1-17 years in North America. These differences in prevalence may be due to seasonal variations of occurrence of conjunctivitis and short duration of illness. In current study, chalazion was detected in 0.3% and conjunctivitis in 6% children. These results are comparable with Desai et al10 study who reported the prevalence of chalazion in 0.25% and conjunctivitis in 5.0% children. In this study, the occurrence of infective eye diseases was significantly higher among children of government schools (5%) as compared to private schools (1%). Moreover, it was more among females (4.2%) in comparison to males (1.2%). Variations in the prevalence of infective disorders can be explained by difference in socioeconomic status and personal hygiene of children.
In current study, prevalence of vitamin A deficiency (VAD) was found to be 2.6%. It was more (5%) among children of government schools in comparison to (0.2%) in private school. In this study, conjunctival xerosis with bitot’s spots was most common manifestation of VAD. In comparison to our study, lower prevalence of VAD was observed by Gupta et al4 in Shimla (1.8%), whereas higher prevalence was reported by Desai et al10 in Rajasthan (5.4%) and Datta et al17 in Kolkata (9%) in age group 4 to16 years. Prevalence of VAD decreased with age in the present study, which is similar to that has been observed by Desai et al study10. Internationally, Wedner et al26 noted higher prevalence (6%) among school children of age 7-19 years in Tanzania. These differences are because children included in these studies belonged to low socioeconomic status associated with unhealthy dietary pattern and had poor nutritional status, leading to higher chances of vitamin A deficiency.
This study showed prevalence of colour blindness of 2.6% which is comparable to results of earlier studies, conducted in North India by Gupta et al4 in Shimla and Desai et al10 in Rajasthan, who detected the prevalence 2.3% and 2.9% respectively in 4-16 years age group. However, lower prevalence of colour vision defects was reported by Pratap et al25 in North India (0.11%), and by Gupta et al29 in Chandigarh (1.2%). The identification of colour vision defects with concurrent vocational counseling should also be done at the earliest possible to save the child from frustration later on and help him to choose a suitable profession.
Present study found higher prevalence of congenital disorders (1.3%) than reported from other studies in India4, 10, 15. Lid and adnexal disorders were seen in 2.4% children in current study which is higher than the prevalence 1.01% noted by Murthy et al in urban Delhi 8 and 1.5% by Kariapatti study in south India 30.
There was almost similar overall prevalence of ocular morbidity in both genders. It was found to be 24.17% in males and 24.28% in females. Whereas, marginal difference in the prevalence of ocular diseases was observed in Gupta et al4 study in Shimla (males 31% and females 33%) and also in Sehgal et al31 study in Delhi (males 46.1% and females 48.3%). However, Khurana et al15 reported higher prevalence in females (73.5%) as compared to males (49.4%) in Haryana. In their study, prevalence of infectious diseases like trachoma, conjunctivitis and blepharitis was higher among females. Similarly, present study detected higher prevalence (4.6%) of infective eye disease among females as compared to 1.8% in males. Color blindness is a sex-linked disease hence it was found to be significantly higher among males in present study which is similar to the result of Gupta et al. study4. In almost all studies conducted in India, the prevalence of ocular morbidity decreased with age, the results of our study also confirmed this finding in North India 10, 15-17. Higher prevalence of ocular morbidity occurred in younger children (5-9 years), because higher prevalence of refractive errors specially hypermetropia (10%) and infective eye diseases (4.2%) was seen, which is similar to the other studies from North India10, 23. Results showed that there was decrease in prevalence with increasing age which is probably due to disappearance of age-related hypermetropia, improvement in ocular hygiene, and better health education in higher age group.
There was significant difference in between government and private school going children. Ocular morbidity was found in 145 out of 506 screened children in government schools (29%) as compared to 99 out of 501 screened children in private schools (20%). Whereas, this difference was not detected by Gupta et al4 study in Shimla. Results showed that prevalence of refractive errors in government schools (12%) and private schools (13%) was almost similar. But certain conditions including infective ocular disorders and vitamin A deficiency showed more prevalence in government school children than private school children.
The current study also included school performance of every child and its relation with ocular morbidity was also determined. Results suggested that school performance was significantly affected by ocular diseases. Majority of children (45.1%) with ocular diseases had average school performance. Results also suggested that 15% children had already corrected refractive error with glasses as compared to 85% children who were not aware of their refractive error. So, present study strongly highlights the need of early detection and treatment of vision related problems to avoid long term visual disability, which require intervention at school level by appropriate eye care programmes.
BIBLIOGRAPHY
- Prajapati P, Oza J, Prajapati J, Kedia G, Chudasama RK. Prevalence of ocular morbidity among school adolescents of Gandhinagar District, Gujarat. Online J Health Allied Scs 2010; 9:5.
- Brown MM, Brown GC, Sharma S, Bisbee B. Quality of life associated with visual loss: a time trade off utility analysis comparison with medical health states. Ophthalmology 2003; 110:1076–81.
- Gilbert C, Foster A. Childhood blindness in the context of VISION 2020—The Right to Sight. Bull World Health Organization 2001; 79:227–32.
- Gupta M, Gupta BP, Chauhan A, Bhardwaj A. Ocular morbidity prevalence among school children in Shimla, Himachal, North India. Indian J Ophthalmol 2009; 57:133-8.
- Vision 2020: The Right to Sight. (available at http ://www.v2020.org) (last accessed on 22.12.2014)
- Sun BC. Low vision in clinical practice. Beijing: Huaxia Publishing House. 1999; 36:154–9.
- Park K. Textbook of Preventive and Social Medicine. Banarasidas Bhanot Publications. 19th Ed. 2007; 337-8.
- Murthy GV, Gupta SK, Ellwein LB, Munoz SR, Pokharel GP, Sanga L, et al. Refractive error in children in an urban population in New Delhi. Invest Ophthalmol Vis Sci 2002; 43:623-31.
- Government of India. Annual Report, Ministry of Health & Family Welfare, New Delhi, 2004.
- Desai S, Desai R, Desai NC, Lohiya S, Bhargava G, Kumar K. School eye health appraisal. Indian J Ophthalmol 1989; 37:173-5.
- Babu R. Study on the prevalence of childhood eye morbidities in rural region of Karnataka state, south India. MSc Thesis in Community Eye Health submitted to Jr. London School of hygiene & tropical medicine; 2007-2008. (available at https://www.lshtm.ac.uk/library/MSc_CEH/2008-09/490527) (last accessed on12.1.2015)
- Gupta A, Lal R, Mazta S.R., Sharma D. Prevalence of refractive errors, color vision defects and other ocular disorders in school-going children: Primary screening by school teachers. JIMSA 2012; 25:223-24.
- Kangra District Population Census 2011, H.P. literacy sex ratio and density. (https://www.census2011.co.in/census/district/230-kangra)(Last assessed on 22.12.2014)
- Chaturvedi S, Aggarwal OP. Pattern and distribution of ocular morbidity in primary school children of rural Delhi. Asia Pacific J Public Health 1999; 11: 30-3.
- Khurana AK, Parmar IPS, Aggarwal SK. Ocular morbidity among school children in Rohtak city. Indian J Public Health 1984; 28:217-20.
- Kalikivayi V, Naduvilath TJ, Bansal AK, Dandona L. Visual impairment in school children in southern India. Indian J Ophthalmol 1997;45:129-34
- Datta A, Choudhury N, Kundu K. An epidemiological study of ocular condition among school children of Calcutta Corporation. Indian J Ophthalmol 1983; 31:505–10.
- Rustagi N, Uppal Y, Taneja Screening for visual impairment: Outcome among school children in a rural area of Delhi. Indian J Ophthalmol 2012; 60(3): 203-6.
- Nepal B P, Koirala S, Adhikary S, Sharma A K. Ocular morbidity in school children in Kathmandu. Br J Ophthalmol 2003; 87:531–4.
- Gupta Y, Sukul RR, Gupta M, Phougat A, Jain R, Varshney A. School eye survey in rural population in UP, India. Nepal J Ophthalmol 2011; 3:78-9.
- Robinson B, Acron CJ, Millar CC, Lyle WM. The prevalence of selected ocular diseases and conditions. Optom Vis Sci 1977; 74:79–91.
- Biswas J, Saha I, Das D, Bandyopadhyay S, Ray B, Biswas G. Ocular morbidity among children at a tertiary eye care hospital in Kolkata, West Bengal. Indian J Public Health 2012; 56:293-6.
- Sethi S, Kartha GP. Prevalence of refractive errors in school children (12-17 years) of Ahmedabad City. Indian J Community Med 2000; 25:181–3.
- Shrestha RK, Joshi MR, Ghising R, Pradhan P, Shakya S, Rizyal A. Ocular morbidity among children studying in private schools of Kathmandu valley: A prospective cross sectional study. Nepal Med Coll J 2006; 8:43-6.
- Pratap VB, Lal HB. Pattern of paediatric ocular problems in North India. Indian J Ophthalmol 1989; 37:171–2.
- Wedner SH, Ross DA, Balira R, Kaji L, Foster A. Prevalence of eye diseases in primary school children in a rural area of Tanzania. Br J Ophthalmol 2000; 84:1291–7. Kumar R, Dabas P, Mehra M. Ocular morbidity amongst primary school children in Delhi. Health &Population Perspectives & Issues 2007; 30:222-9.
- Kumar R, Dabas P, Mehra M. Ocular morbidity amongst primary school children in Delhi. Health &Population Perspectives & Issues 2007; 30:222-229.
- Singh S, Singh H, Joshi VS. Eye diseases among primary school children. Indian J Ophthalmol 1974; 22:1-3.
- Gupta N, Arya SK, Walia D, Mallik A, Sood S. Ocular morbidity among school-going children in the Union Territory of Chandigarh. Int Ophthalmol 2014; 34:251-7.
- Nirmalan PK, Vijayalakshmi P, Sheeladevi S, Kothari MB, Sundaresan K, Rahmathullah L. The Kariapatti pediatric eye evaluation project: baseline ophthalmic data of children aged 15 years or younger in Southern India. Am J Ophthalmol 2003; 136:703-9.
- Dantas PE, Alves MR, Nishiwaki-Dantas MC. Topographic corneal changes in patients with vernal keratoconjunctivitis. Arq Bras Ophthalmol 2005; 68:593-8.
Leave a Comment