
Dr. Shruti Kochar Maru ( K17834 )
Abstract
Sub-epithelial corneal haze is a complication of Photorefractive keratectomy (PRK). Our aim was to study biomarkers and inflammatory pathways involved in development of corneal haze by gene expression analysis of corneal epithelium. Epithelium of 4 eyes of 2 patients who developed haze postoperatively and that of 6 eyes of 3 age matched controls was analyzed. Quantitative real-time PCR was performed for inflammatory markers, corneal structure genes, fibrosis associated genes and regulators of signalling cascade. Gene expression analysis showed that Collagen I and Collagen IV were reduced in haze patients. Inflammatory factor TNFα was elevated in haze patients. Development of haze is a multifactorial process that depends on molecular status of corneal epithelium prior to surgery. This demonstrates that pre-screening of patients based on their corneal biomarker status may help identify patients prone to develop haze.
Key Words:
Corneal haze, PRK, biomarkers, inflammation, gene expression
Introduction:
Development of excimer laser was a breakthrough in correction of ametropia. Corneal refractive surgery is a constantly evolving field following its discovery in 1949 by Jose Barraquer [1] Photorefractive keratectomy (PRK) has certain advantages over LASIK such as elimination of flap related complications, epithelial ingrowth, flap striae and diffuse lamellar keratitis. In addition, PRK maintains sufficient residual stromal thickness, thus reducing the risk of post refractive surgery ectasia. However, PRK is associated with development of post excimer ablation corneal haze, which affects the visual outcome. Corneal haze is an excessive wound healing response with an incidence of 1.44% following refractive surgeries. [2] The nature and location of corneal haze is associated with the type of the preceding surgical procedure – corneal collagen crosslinking (CXL) is linked to mid-stromal haze, whereas PRK results in sub-epithelial haze. [3] Despite significant evidence available regarding the characteristics of corneal haze, the etio-pathogenesis and predisposing factors are poorly understood. Multiple clinical risk factors that may predispose to corneal haze include high refractive error, higher ablation depth, smaller ablation zone [4], UV B exposure [5] and color of the iris [6]. Proliferation and migration of stromal keratocytes are in part mediated by factors from the corneal epithelium [7]. In addition, contribution of the epithelium in the development of myofibroblasts in the stroma, essential for normal wound healing is regulated by cytokines / growth factors including TGFβ [8]. Hence, corneal epithelium would serve as an appropriate tissue to determine factors that may predispose to haze in a subset of patients undergoing refractive surgery. This study aims to elucidate the molecular factors underlying corneal haze utilizing both clinical samples.
Methods:
Inclusion and exclusion criteria were as follows: Patient must be at least 18 years of age with a stable refraction for the past 12 months. Patient must not have more than 3.5 D of spherical equivalent refractive error as determined by manifest subjective refraction. Patients must have no significant ocular or systemic pathologies. Corneal epithelium was collected intra-operatively from patients undergoing PRK, none of who had any clinical indicators suggesting a risk for development of haze. In the current study, 110 eyes of 55 patients were examined. 4 eyes that developed haze postoperatively and 6 eyes of age matched controls without haze were recruited in the study. Corneal epithelium was collected intraoperatively prior to excimer ablation and stored in the biorepository. Our study has investigated the pre-surgical predisposing factors driving corneal haze in epithelium collected from patients prior to haze development following PRK. Clear cornea that went on to develop corneal haze and had corneal epithelium stored from the primary surgery (PRK) were categorized as ‘haze predisposed’ group. Age, gender and duration matched patients who continued to maintain corneal transparency were chosen as controls. The isolation of mRNA and the analysis of gene expressions was done.
Results:
The representative slit lamp bio-microscopy and corneal densitometry (measure of corneal haze) features shown in Figure 1. Corneal haze is associated with a subset of inflammatory genes (Figure 2). Extra cellular matrix remodeling factors are deregulated in patients predisposed to haze (Figure 3)
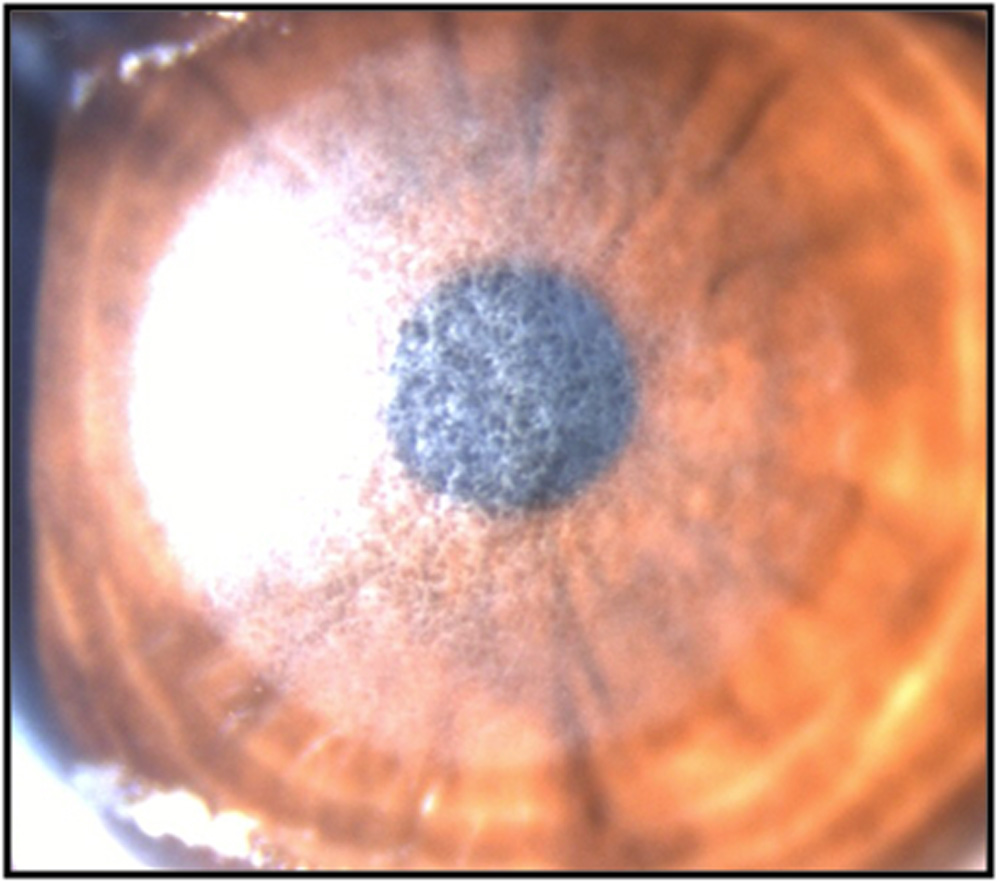
Figure 1 Post PRK haze
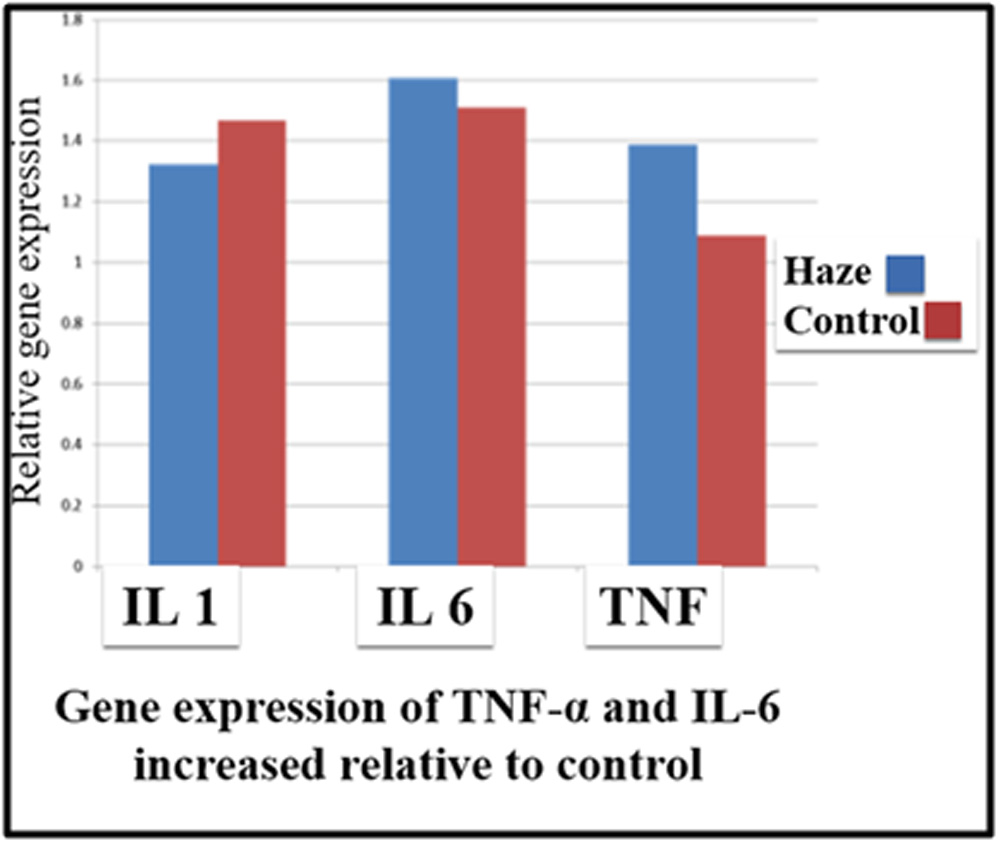
Figure 2 Tumor Necrosis Factor α (TNFα) and Interleukin (IL6) are up regulated in haze predisposed compared from controls.
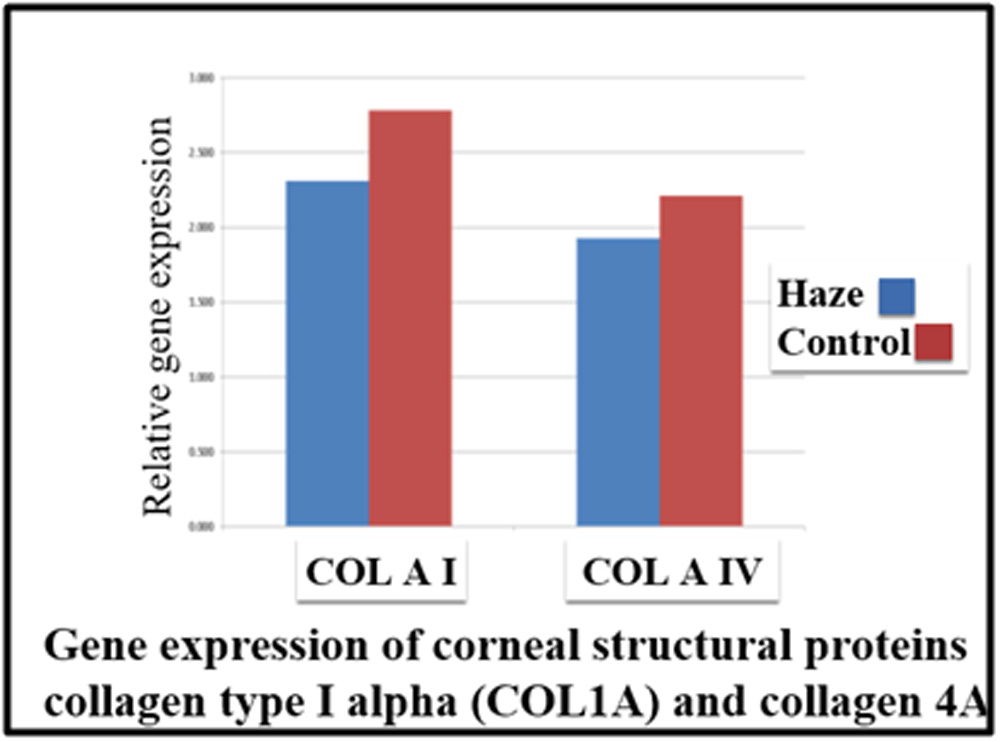
Figure 3 Collagens mRNA expression profile shows a down regulation in COL I A1 and COL IV A1 expression in haze predisposed.
Discussion:
A distinct gene expression pattern was observed in the stored epithelium of patients who went on to develop corneal haze suggests the presence of molecular factors that may predispose to corneal haze. Thus, we hypothesized that there are patient specific factors that may affect the course and severity of the fibrotic response that leads to poor visual outcomes in certain patients, post-surgery. In this study we provide a new outlook on predisposing factors which leads to corneal haze. Injury gives rise to a cascade of signalling events through all the layers of cornea. Epithelium is a good source of tissue to understand these events<
Conclusion
Our data shows a prolonged inflammatory response due to higher mRNA levels of IL6 and TNFα and reduced IL1 expression levels in patient epithelium. Development of haze is a multifactorial process that depends on molecular status of corneal epithelium prior to surgery. This demonstrates that pre-screening of patients based on their corneal biomarker status may help identify patients prone to develop haze. This is a unique study that co-related cell biology that co-relating patient epithelium data. Chronic low-grade inflammation pre-operatively may predispose to post-surgical haze.
References:
1. Nordan, L.T., Barraquer lecture. Jose Barraquer: father of modern refractive keratoplasty. Refract Corneal Surg, 1989. 5(3): p. 177-8.
2. Girgis, R., et al., Bilateral corneal scarring after LASIK and PRK in a patient with propensity to keloid scar formation. Eye (Lond), 2007. 21(1): p. 96-7.
3. Carr, J.D., R. Patel, and P.S. Hersh, Management of late corneal haze following photorefractive keratectomy. J Refract Surg, 1995. 11(3 Suppl): p. S309-13.4. Rajan, M.S., et al., Effects of ablation diameter on long-term refractive stability and corneal transparency after photorefractive keratectomy. Ophthalmology, 2006. 113(10): p. 1798-806.
5. Stojanovic, A. and T.A. Nitter, Correlation between ultraviolet radiation level and the incidence of late-onset corneal haze after photorefractive keratectomy. J Cataract Refract Surg, 2001. 27(3): p. 404-10.
6. Tabbara, K.F., et al., Corneal haze among blue eyes and brown eyes after photorefractive keratectomy. Ophthalmology, 1999. 106(11): p. 2210-5.
7. Mohan, R.R., et al., Apoptosis, necrosis, proliferation, and myofibroblast generation in the stroma following LASIK and PRK. Exp Eye Res, 2003. 76(1): p. 71-87.
8. Jester, J.V., W.M. Petroll, and H.D. Cavanagh, Corneal stromal wound healing in refractive surgery: the role of myofibroblasts. Prog Retin Eye Res, 1999. 18(3): p. 311-56.
Leave a Comment