
Dr. Shobhana Phukan (S19549 )
Abstract
Background: Subclinical Hypothyroidism (SCH) is defined as an asymptomatic condition characterized by normal serum levels of free thyroxine and elevated serum concentration of thyrotropin (>4.0µIU/ml). Association between Diabetic retinopathy and SCH is unclear.
Aim: To study the relationship between severity of Diabetic Retinopathy and SCH in patients of Diabetic Retinopathy with type2 Diabetes Mellitus.
Method: 120 patients of Diabetic Retinopathy with known type2 Diabetes Mellitus were taken and categorized them according to severity of Diabetic Retinopathy as per ETDRS classification. Serum thyrotropin (TSH) and free Thyroxine (FT4) concentration were measured in all 120 patients. Patients with normal TSH and FT4 values are euthyroid patients and those with normal FT4 but TSH value >4µIU/ml are considered as having subclinical hypothyroidism. Severity of Diabetic Retinopathy is compared between the Euthyroid and Subclinical Hypothyroid group.
Result: Out of the 120 patients included in the study, 72(60%) were male and 48(40%) were female. 97 patients (80.83%) were Euthyroid and 23 patients (19.17%) had subclinical hypothyroidism. It was observed that prevalence of more severe form of Diabetic retinopathy (severe NPDR and PDR) was higher in SCH group as compared to euthyroid group. Severity of Diabetic retinopathy was compared with serum TSH level and it was seen that severity of Diabetic retinopathy significantly increases with increase in serum TSH value.
Conclusion: Patients with SCH had more severe form of Diabetic retinopathy as compared to patients with euthyroidism. Severity of diabetic retinopathy significantly increases with increase in serum TSH value.
Key words: Subclinical hypothyroidism, free Thyroxine, Thyrotropin, ETDRS
Introduction
Diabetic Retinopathy (DR) is one of the major micro vascular complications of diabetes. If untreated, it may lead to blindness. If diagnosed and treated promptly, blindness is usually preventable.
Diabetes is fast gaining the status of epidemic in India and as of 2000, India (31.7 million) topped the world with the highest number of people with diabetes.With the increasing prevalence of diabetes, burden of blindness due to the disease is also increasing.
Assessing the risk factor of DR, particularly modified risk factor, is important for early intervention to reduce the onset and progression of DR. Hence the present observational study is conducted to study the relationship between severity of diabetic retinopathy and subclinical hypothyroidism.
Association between diabetic retinopathy with duration of diabetes, poor glycemic control, dyslipidemia and elevated blood pressure are already found in various studies.1,2Whereas studies are still going on regarding its relationship with other factors like plasma fibrinogen level, plasma homocysteine level, thyroid dysfunction including subclinical hypothyroidism etc. Association between diabetic retinopathy and subclinical hypothyroidism is a topic of growing interest and there are only few studies in recent literature.
Subclinical hypothyroidism (SCH) is defined as a condition where thyroid stimulating hormone (TSH) levels is above the upper limit of the reference range in addition to a normal free thyroxine level (FT4).3
SCH is a common endocrine disorder and has been reported to range from 4-10% in general population. The frequency of thyroid dysfunction in diabetic patients is higher than that of the general population, the most common dysfunction being SCH. Prevalence of SCH in diabetes varies between 2 and 17%.4,5 Few reported studies have investigated the association between Subclinical hypothyroidism and microvascular complications in type 2 diabetes.
Methods:
The present study was conducted taking up 120 Diabetic Retinopathy patients with known type 2 diabetes mellitus. The study was conducted for a duration of 1 year from July 2014 to June 2015. Ethical clearancewas taken from institutional ethics committee.
Patients were explained the nature of the study and prior written informed consent was taken from every patient before enrolment. After obtaining detailed history, a comprehensive ophthalmological examination was done with special emphasis on the fundus examination. The level of severity of retinopathy was determined by indirect ophthalmoscopy for a pan retinal view, and stereoscopic slit lamp biomicroscopy of the disc and macula using +90D lens. Ancilliary tests selectively done were stereo fundus photography, fluorescein angiography and OCT. Based on ETDRS criteria patients were graded according to their severity of retinopathy into mild NPDR, moderate NPDR, severe NPDR, very severe NPDR, Early PDR and High risk (HR) PDR. Out of the two eyes, the eye having more severe form of retinopathy was considered in grading. Patients with severe NPDR and very severe NPDR were considered in one group and those with PDR and HR PDR were considered in one group for data analysis.
Serum free T4 and TSH was obtained in all patients. Free T4 level was estimated by Radioimmunoassay using BRIA COAT – 1 RIA KIT for free thyroxin, ( two step assay),Isotopes and radiation: Health & prosperity, Board of Radiation and Isotope Technology (BRIT) and TSH level by Immunoradiometricassay using IRMA Kit for human thyroid stimulating hormone, IRMAK-9, Isotopes & Radiation: Health & Prosperity, Board of Radiation and Isotope Technology. The normal reference range considered are- for free T4 – (10-20)pg/mland for TSH – (0.17-4.05)µIU/ml. Patients having TSH value > 4.0µIU/ml in presence of normal free T4 value were considered as having subclinical hypothyroidism. Patients having TSH and free T4 value within normal reference range were euthyroid patients. Severity of Diabetic retinopathy was compared between the two groups.
Following patients were excluded from the study: 1. Patients with significant media opacity interfering in diagnosis and classification of DR 2. Patients taking thyroid hormones, after thyroidectomy or radioactive iodine therapy 3. Patients with overt hypothyroidism, overt hyperthyroidism and subclinical hyperthyroidism 4. Pregnant patient 5. Critically ill patients
Statistical analysis: Data are represented in terms of number, percentage, mean ±SD. ‘p’ value is calculated using chi square and ANOVA test. ‘p’ value <0.05 is considered as significant.
Results:
Inthe presentstudy,most of the patientswerefound tobe in the agegroupof 51-60years.Outofthe120 patients includedin the study,72(60%) were male and48(40%)werefemale. It was seen that most of the patients with subclinical hypothyroidism were female with male: female ratio of 1:1.3.On fundoscopy,variousfeatures of DR were observed carefully onboththe eyes. Different fundusfindingsonboththe eyes ofstudy subjects arepresentedonthefig-1.
Fig – 1
Fundus findings of Diabetic retinopathy patients
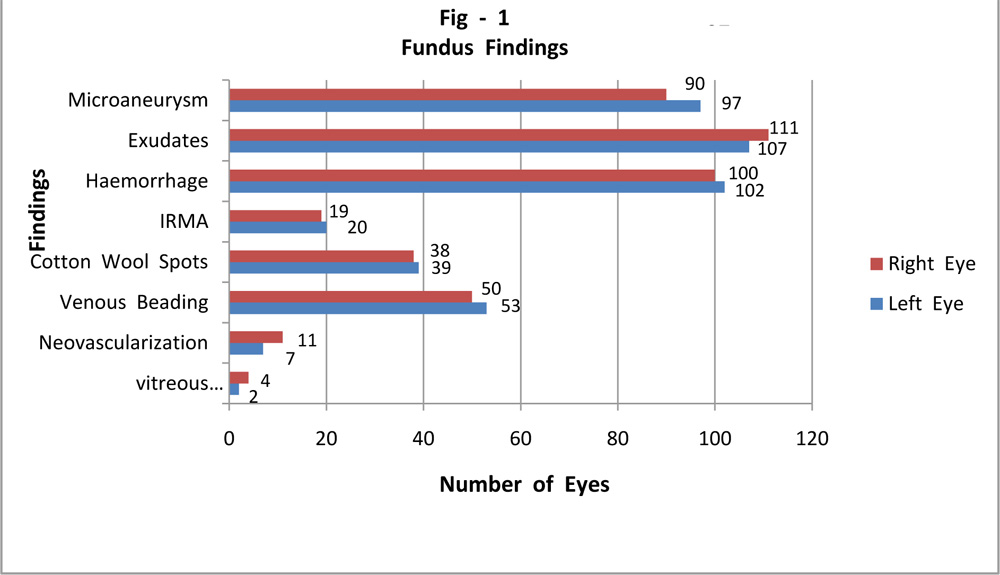
IRMA – Intraretinal microvascular abnormalities
Table – 1 showsdistributionofDiabeticRetinopathy according to different stages
Table – 1
Distribution of severity of Diabetic Retinopathy
| Retinopathy Group | Number | Percentage |
| (n) | (%) | |
| Mild NPDR | 34 | 28.33 |
| Moderate NPDR | 49 | 40.83 |
| (Severe + Very Severe) | 24 | 20.00 |
| NPDR | ||
| PDR (Early + High Risk) | 13 | 10.84 |
| Total | 120 | 100.00 |
NPDR – Non proliferative Diabetic Retinopathy, PDR – Proliferative Diabetic Retinopathy
Fig- 2shows distribution of SCH among patients of diabeticretinopathy with type2DM.97patients(80.83%)wereEuthyroid and 23patients (19.17%)hadsubclinical hypothyroidism.So, theprevalenceofSCHamong thepatientsofDR withtype2DMwas foundto be19.17%.
Fig – 2
Distribution of SCH in patients of Diabetic Retinopathy with type 2 DM
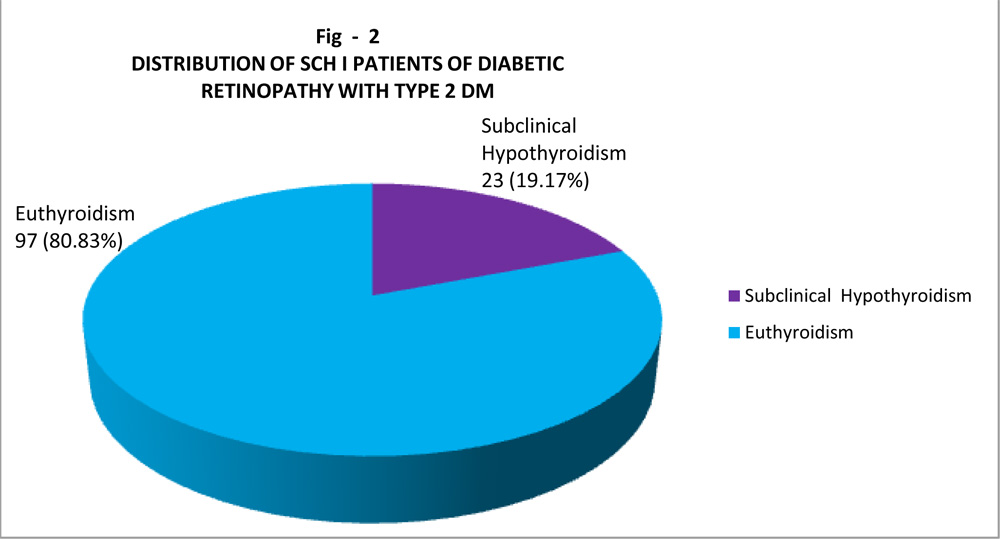
Fig- 3shows comparison ofdifferent stagesof DiabeticRetinopathy inSCH andEuthyroidpatients. Wehaveobservedthat 29out of97 euthyroid patients and 5 outof 23SCHpatients hadmild NPDR (29.9% vs 21.74%). 41 out of 97 euthyroid patients and 8outof23 SCH patientshad moderate NPDR (42.27% vs 34.78%).Severe NPDRwas seen in 18euthyroidand6SCH patients(18.56%vs26.09%). PDRwasseenin 9euthyroid and4 SCHpatients(9.27%vs17.39%).So,wehaveseen thatprevalenceof severe NPDR andPDR was higherintheSCH group as compared toeuthyroid group andprevalence ofmildand moderate NPDR washigher in theeuthyroidgroup as compared toSCH group. However thisassociation isfoundtobestatisticallynot significant (p =0.503296).Here ‘p’ value is calculated using chi square test.
Fig – 3
Comparison of different stages of DR in SCH patients with Euthyroid
Patients
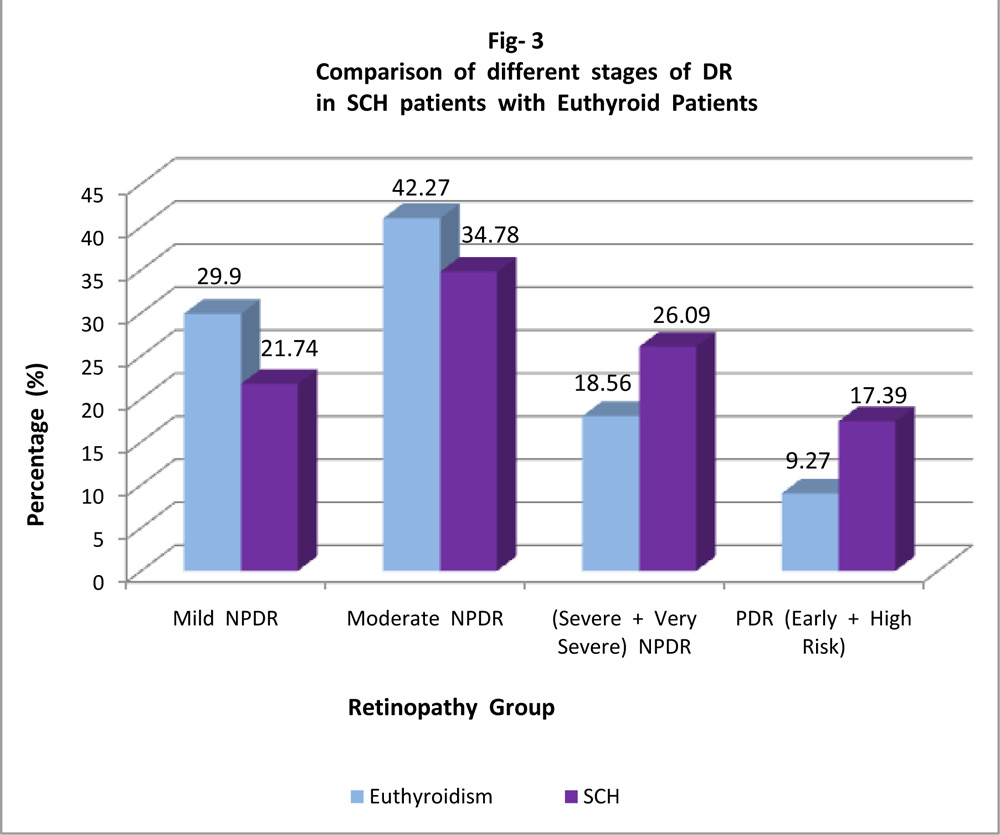
Fig- 3
Comparison of different stages of DR
in SCH patients with Euthyroid Patients
NPDR : Non Proliferative Diabetic Retinopathy, PDR : Proliferative Diabetic
Retinopathy, SCH : Subclinical Hypothyroidism
Table – 3 shows serum thyroid stimulating hormone (TSH) levels according to different stages of diabetic retinopathy in type 2 diabetic patients with subclinical hypothyroidism. Itwasseen that severityofdiabetic retinopathysignificantlyincreaseswithincreaseinserumTSH value.Whenstatistical analysis was done usingANOVA test,this associationwas foundto be statistically significant(p=0.025554).
Table -3
Serum Thyroid Stimulating hormone (TSH) levels according to different stages of diabetic retinopathy in type 2 diabetic patients with subclinical hypothyroidism
| Retinopathy Group | Number | TSH Range (µIU/ml) | P value | |||
| (n) | Mean±SD | Range | ||||
| Mild NPDR | 5 | 5.42 | ± 0.94 | 4.30 | – 6.56 | |
| Moderate NPDR | 8 | 5.45 | ± 0.73 | 4.73 | – 7.00 | 0.0255554 |
| (Severe + Very Severe) | 6 | 6.68 | ± 0.77 | 6.03 | – 8.00 | (S) |
| NPDR | ||||||
| PDR (Early + High Risk) | 4 | 7.08 | ± 1.69 | 4.73 | – 8.40 | |
NPDR :Non Proliferative Diabetic Retinopathy, PDR : Proliferative Diabetic Retinopathy
Discussion:
In thepresent study,wehaveseen thatout of the 120 patients,23patients(19.17%)had subclinicalhypothyroidism.So,the prevalence of SCH among thepatientsofDiabetic Retinopathy with Type2Diabetes Mellituswasfoundto be 19.17%.Our study foundtheprevalenceof SCH intype 2 DM patients similar to other studies. TheprevalenceofSCH ingeneral populationis estimated to be4.3-9 %.6,7 Patientswith
diabetesmellitusare at anincreasedriskofthyroid dysfunction,withthe reportedprevalenceofSCHin diabetes varyingbetween 2and17%.8
Wehaveseenthatprevalence ofmoresevere form of retinopathy,i.e.severeNPDRandPDRwas higherintheSCH groupas compared to euthyroidgroup.
Our results are consistent with the following studies:
Bo-Yeon Kim etal found that prevalence of severediabeticretinopathywas significantlyhigher in theSCH group comparedtothe euthyroidgroup(32.8% vs. 19.6%, p=0.036).They mentionedseveralmechanisms for thisinvolvementlike dyslipidemia,insulinresistance etc.9
Guang-Ran Yangetal ina case controlstudyfoundthat the prevalenceof Subclinical hypothyroidism in theProliferativeDiabeticRetinopathygroup(51/187, 27.3%) washigher than thatintheNon proliferative Diabetic Retinopathygroup(32/184, 17.4%). Intheir study,theyhaddonea logisticregression analysis to identify anindependentrelationshipbetween
SCH and PDR. They gavethe conclusion that ,PDR wasat increased riskin patients with SCH.10
SimilarobservationwasfoundbyJin-KuiYangetal in 2010. In theirstudy, they found that thetrend forsevereretinopathy was significantly higher in the Subclinical hypothyroidgroupthanin the euthyroidgroup. Subclinical hypothyroidism wasassociatedwith greater prevalence of diabetic retinopathy, especially sight-threateningdiabeticretinopathy.11
Inameta-analysisby JingyangWu et al, obtaining eight observational studies,foundthatthere is
a significant associationbetween DR and SCH, andexposure to SCH canincrease theDR risk 2.13 times.12
Inourstudy, wehave also seenthat,severity of DRsignificantly increases withincreasein serum TSHvalue (p=0.05554).
Khodeir et alin2012conducted astudy takingnewly diagnosed patients oftype 2diabetesmellitus.They foundthatsubclinical hypothyroidismis associated with diabetic retinopathy in type2diabetic patients.Theirresultsshowed ahigherrateof diabeticretinopathy ineuthyroid patientswhohad higherlevelsof TSH value.13Inthesameway, Guanget al in 2010, reported that patients with higher levels of TSHhadasignificantly higher rate of PDR thanpatientswithlower levels ofTSH.10
Yanget alreported anassociationbetween retinopathyandsubclinical hypothyroidism, especiallysight threatening diabeticretinopathy.They also mentionedthat, eveneuthyroid patients with TSHlevels between 2and<4µIU/mlhadahigherrateof sight threatening diabetic retinopathythanthose between 0.4 and<2.0µIU/ml (p=0.008).11
Several mechanisms may be involved intheassociationofDiabetic retinopathyandSCH. Endothelialdysfunctionand dyslipidemia seen in SCH are two important factorswhich maycontributetothe pathogenesis of DR.Hyperlipidemia causes endothelial dysfunction bydecreasing expressionof endothelial nitricoxide synthase and by increasing dimethylargininelevels,which is anendogenous inhibitor of endothelialnitricoxide. Other possible mechanism supportedbyKimet al was that Insulin resistance might bea probablefactorin theassociationbetween SCHand Diabetic retinopathy.14They foundhigher status ofinsulin resistance inthe SCHgroupthan in the euthyroid group.
Other mechanisms whichmaycontributeto the pathogenesisofdiabetic retinopathy inpatients ofSCHareinflammation,raised C-ReactiveProtein (CRP),oxidative stress etc. Oxidative stresshasbeen linkedtothe histopathological changes of DR, such asretinal basement membrane thickening15 and capillary cell loss.16
Conclusion: Inthe present study, the prevalence of SCHamongthe patientsofDRwithtype2DM was found to be 19.17%. Prevalence of severe NPDR& PDR was higher in patients with SCHascomparedtoeuthyroidpatients. Severity ofDR significantly increaseswith increase in serum TSHvalue. Therefore,SCHmay be associatedwith severityofdiabetic retinopathy.
However,this is ahospitalbased observationalstudy and further prospective population base dstudiesare requiredinthis fieldtocome to a definiteconclusion and to comment onwhether thyroid function screening in required in patients of DR.
References
- Stratton IM, Kohner EM, Aldington SJ, Turner RC, Holman RR, Manley SE, Matthews DR, Risk factors for incidence and progression of retinopathy in type2 Diabetes over 6 years from diagnosis, Diabetologia 2001, Feb;44(2):156-63.
- Chang YC, Wu WC .Dyslipidemia and diabetic retinopathy. Rev Diabet Stud. 2013;10(2-3):121-32.
- . Garber JR, Cobin RH, Gharib H, Hennessey JV, Klein I, Mechanick JI, Pessah-Pollack R, Singer PA, Woeber for the American Association of Clinical Endocrinologists and American Thyroid Association Task force on Hypothyroidism in Adults KA. Clinical practice guidelines for hypothyroidism in adults: cosponsored by the American Association of Clinical Endocrinologists and the American Thyroid Association. Thyroid. 2012 Dec 1;22(12):1200-35.
- Perros P, McCrimmon RJ, Shaw G, Frier BM. Frequency of thyroid dysfunction in diabetic patients: value of annual screening. Diabetic Medicine. 1995 Jul 1;12(7):622-7.
- Smithson MJ. Screening for thyroid dysfunction in a community population of diabetic patients. Diabetic medicine. 1998 Feb 1;15(2):148-50.
- Canaris GJ, Manowitz NR, Mayor G, Ridgway EC. The Colorado thyroid disease prevalence study. Archives of internal medicine. 2000 Feb 28;160(4):526-34.
- Hollowell JG, Staehling NW, Flanders WD, Hannon WH, Gunter EW, Spencer CA, Braverman LE. Serum TSH, T4, and thyroid antibodies in the United States population (1988 to 1994): National Health and Nutrition Examination Survey (NHANES III). The Journal of Clinical Endocrinology & Metabolism. 2002 Feb 1;87(2):489-99.
- . Perros P, McCrimmon RJ, Shaw G, Frier BM. Frequency of thyroid dysfunction in diabetic patients: value of annual screening. Diabetic Medicine. 1995 Jul 1;12(7):622-7.
- . Kim BY, Kim CH, Jung CH, Mok JO, Suh KI, Kang SK. Association between subclinical hypothyroidism and severe diabetic retinopathy in Korean patients with type 2 diabetes. Endocrine journal. 2011;58(12):1065-70.
- Yang GR, Yang JK, Zhang L, An YH, Lu JK. Association between subclinical hypothyroidism and proliferative diabetic retinopathy in type 2 diabetic patients: a case-control study. The Tohoku journal of experimental medicine. 2010;222(4):303-10.
- Yang JK, Liu W, Shi J, Li YB. An association between subclinical hypothyroidism and sight-threatening diabetic retinopathy in type 2 diabetic patients. Diabetes care. 2010 May 1;33(5):1018-20.
- Wu J, Yue S, Geng J, Liu L, Teng W, Liu L, Chen L. Relationship between Diabetic Retinopathy and Subclinical Hypothyroidism: a meta-analysis. Scientific reports. 2015 Jul 20;5.
- Khodeir, S.A.,Abd E 1 Raouf, Y.M, Farouk, G. and Allam, W.A., A study on the Relationship between Subclinical Hypothyroidism and Diabetic Retinopathy in Type2 Diabetic patients, Journal of American Science,2012;8(1)
- Kim SR, Tull ES, Talbott EO, Vogt MT, Kuller LH. A hypothesis of synergism: the interrelationship of T 3 and insulin to disturbances in metabolic homeostasis. Medical hypotheses. 2002 Nov 12;59(6):660-6.
- Robison Jr WG, Jacot JL, Katz ML et al. Retinal vascular changes induced by oxidative stress of alpha-tocopherol deficiency contrasted with diabetic microangiopathy. J OculPharmacol Ther.2000;16(2):109-20.
- Kowluru RA Diabetic retinopathy: mitochondrial dysfunction and retinal capillary cell death. Antioxid Redox Signal.2005;7(11-12):1581-87.
Leave a Comment