
Dr. Manavi Deokrishna Sindal, S11035, Dr. Sabyasachi Sengupta, Dr. Tejashree Sathe
INTRODUCTION
Diabetes mellitus (DM) has in recent times, gained importance as one of the most common non-communicable diseases, which contributes to disabilities and deaths in the world. DM is best defined as metabolic cum vascular syndrome of multiple etiologies characterized by chronic hyperglycemia with disturbances of carbohydrate, fat and protein metabolism resulting from defect in insulin secretion, insulin action or both leading to changes in both small vessels (microangiopathy) and large blood vessels (macroangiopathy) and which is often associated with long term damage leading to malfunction and failure of various organs like eyes, kidneys, hearts, nerves and blood vessels.1
Diabetic retinopathy (DR) is highly specific microvascular complication common to both type 1 and type 2 DM. Chances of getting DR in lifetime are higher for type 1 diabetics but people with type 2 DM contribute to the majority of the clinical cases since their overall number is larger.Some form of DR will be present in all the diabetics after 15 to 20 years of DM.2Onsetof DR may be delayed with meticulous control of blood sugar and other risk factors. Vision loss secondary to DR sets in late, with the early grades of DR being asymptomatic without any symptoms.While DR may not be preventable, screening for DR with timely intervention, in the form of laser, intravitreal injections (Anti-VEGF or steroid) and surgery, can prevent vision loss from DR.3
Awareness of the risk of DR and its resultant visual loss is very poor among the general population. This results in delay in seeking care with patient reporting late oncethey experience loss or diminution of vision. Screening can help diagnose early grades of DR, provide timely intervention and increase awareness amongst the population. One setting wherein screening can occur opportunistically is when a person with DM reports to an ophthalmologist for a routine eye check –up. Our institute sees an average of 800 cases a day. Based on population prevalence rates of 13.5% an estimated 110 are likely to be diabetics.4New cases form about one third of daily patient load, enabling us to evaluate approximately 40 diabetics presenting for the first time to our institution every day. This enables us to screen this subset of population and also provide necessary intervention. In this study we aim to determine the proportion of DR amongst the diabetics evaluated at our center and analyze the reason for presenting for an eye examination.
The incidence of DR in population is reported by many population based studies, but the same in a hospital population has not yet been reported, to the best of our knowledge. Most population based studies also tend to survey a particular region or district. We are a tertiary eye care center in south India, catering to a population of Pondicherry, over five districts in Tamil Nadu, parts of Andhra Pradesh, enabling us to screen a wide region of population. Moreover, being an eye care set up, we also were able to elucidate the reason why a diabetic person sought eye care and its correlation to the ophthalmic diagnosis.
In our study, we sought to determine the incidence of DR in known and new diabetic patients reporting to a tertiary eye care centre. We also analyzed the presenting complaint of the patient, correlated it with the ophthalmic diagnosis and demographic as well as systemic factors. We also looked at the patients presenting to us with vision threatening DR (VTDR) at primary visit.
Aims and Objectives not mentioned as separate heading
MATERIALS AND METHODS
MATERIAL AND METHODS
Methodology: The observational cross sectional study adhered to all tenets of the declaration of Helsinki. The study was approved by the institutional review board and ethics committee of the institution, and was carried out from 1st November 2014 to 31st December 2015. All known and newly diagnosed diabetic patients presenting to the outpatient department of Aravind Eye Hospital, Pondicherry for the first time during the study period were included. Known diabetics or the self-reported diabetics were defined as those who were already diagnosed to have DM and were on some form of medication or control method for DM irrespective of their blood sugar levels. Newly diagnosed diabetics were defined as those who werediagnosed for the first time at our hospital on routine blood sugar evaluation, with either RBS > 200 mg/dL or PPBS > 140mg/dL or FBS >126mg/dL at the time of presentation.Follow up cases of DM previously seen at our institution were excluded.
Informed consent was obtained from all the participants. The consent was initially developed in English and later translated into Tamil (regional language) ensuring the meaning and content was preserved. To identify 10% patients with vision threatening diabetic retinopathy (VTDR) with a precision error of 2% the sample size was estimated to be 864. 1000 patients were recruited. The data was recorded in a proforma. Baseline demographic data like age, gender, place of residence (urban or rural), family profile (nuclear or joint), type of occupation (sedentary versus active), education status,monthly income, diet consumed (vegetarian or non-vegetarian), consumption of alcohol or tobacco were recorded.Details regarding DM with regards to duration, family history, control method (exercise, oral hypoglycemic agents or insulin), treatment regularity (regular or irregular) and any prior ocular treatment for DR were noted. Details of co-morbid conditions like hypertension, cardiac disease, nephropathy and hyperlipidemia along with their duration and treatment regularity were also recorded.Anthropometric parameters like heightand weight were measured by trained paramedical personnel. .5A trained paramedical personnel measured blood pressure Routine blood investigations with regards to DM (hemoglobin, fasting/ post prandial/ random blood sugar level, lipid profile, blood urea, serum creatinine and glycosylated hemoglobin) were advised to all patients and recorded for those in whom this data was available. Blood investigations were performed in standardized laboratories either at our hospital or from other laboratories, based on patient preference and convenience. Available blood values were recorded. As the cases without DR did not review back within the study period and also due to financial constraints, not all values were available in all the cases, especially of lipid profile.
Uncorrected visual acuity (UCVA) and best corrected visual acuity (BCVA) was recorded by a trained refractionist in Snellen equivalent and converted to logMAR for analysis. Detailed Anterior segment examination was carried out by slit lamp biomicroscopy, by a post graduate qualified ophthalmologist. Any pathology was noted. Cataract was graded according to LOCSII.6Dilated dilated fundus examination was done by indirect ophthalmoscopy and slit lamp biomicroscopy using a 78D lens, by any of four fellowship trained vitreo-retina consultants. Presence or absence of DR and/or CSME was determined clinically and graded based on standard definitions as described by the ETDRS.7Any other associated retinal pathology was also noted. DR status of some eyes were not gradable due to advanced cataract obscuring the view of fundus. Based on the anterior and posterior segment diagnosis patients were advised appropriate investigations and treatment. In cases were deemed necessary by the examining physician, fundus fluorescein angiography and/or optical coherence tomography was performed to confirm grading of DR, and was recorded in proforma accordingly.
Methods of measurement of outcome of interest:
- Detection of proportion of DR in known and newly diagnosed diabetics availing tertiary eye care hospital facilities.
- To evaluate the presenting complaint of the patient and correlate it to their clinical diagnosis.
- Effect of various demographic and systemic variables on the proportion and severity of DR.
- Detection of percentage of patients presenting with vision threatening DR.
STATISTICAL ANALYSIS
Statistical method:
For statistical analysis, the worse eye was considered, which was defined as the eye with more severe grade of DR. When the DR was equal in both eyes, the eye with lesser visual acuity was considered as the worse eye. If DR and visual acuity was equal in both eyes, then right eye was considered for analysis. Vision threatening diabetic retinopathy (VTDR) was defined as presence of severe NPDR or worse (i.e. PDR or HRPDR) and/or presence of CSME irrespective of grade of DR.8Cataract was considered significant if it was of grade NS3 and above and/or posterior sub-capsular cataract. A total of 1000 cases were recruited for the study of which 44 had mature cataract and could not be analyzed for grades of DR.
Mean (SD) and Frequency (Percentage) were used to describe summary information of data. Test of significance such as Chi-square, t-test were applied. Chi-square test was used to evaluate the association between categorical variables like age, gender, residence, family history with DR category. Student’s t-test was used to evaluate the difference between DR and No DR for the continuous variable such as age, height, weight and BMI. Logistic regression model was carried out to elucidate factors that associate with DR. Probability values, (p<0.05) were considered as statistically significant.All statistical analysis was done by statistical software STATA 11.0.
RESULTS
Out of the 1000 patients recruited, 956 were analyzed. There were 29 (3%) newly diagnosed diabetics and 927 (97%) known diabetics. Six (20.7%) of new DM had DR at presentation. The overall proportion of DR was 51.5%. The proportion of DR in known diabetics and newly diagnosed diabetics was found to be 52.4% and 20.4% in our study.
Table 1 enlists the basic demographic details.Baseline demographics indicate younger age in patients with DR, with increasing risk in age > 50 years. We had one case of Type 1 DM who was 10 years old and showed No DR. Rest of the demographic characteristics did not show much influence on the prevalence of DR in our study. Figure 1 shows the presenting complaints of patients with DM to our institute. The commonest was diminution of vision followed by for a routine check-up. Figure 2 shows the diagnosis at presentation. Out of 956 diabetics, 303 (31.7%) had diagnosis other than cataract and DR. The diagnosis in others included Refractive error and Presbyopia in 240 patients (79.2%), Age related macular degeneration in 19 (6.3%), retinal vein occlusion in 15 (5%), glaucoma in 7 (2.31%) and one case each of – rhegmatogenous retinal detachment, posterior scleritis, anterior ischemic optic neuropathy, dropped nucleus, vitreous hemorrhage, optic atrophy, pathological myopia, retinitis pigmentosa, epiretinal membrane, acute retinal necrosis, corneal foreign body, two cases of corneal dystrophy, and three cases each of pseudophakic bullous keratopathy, central serous retinopathy and retinal dystrophies.
Table 2 shows a comparison of presenting complaint Vs diagnosis. On analyzing the presenting complaints, the commonest complaint was diminution of vision, out of which 55.5% (24.6% + 30.9%) had DR. Amongst those presenting for just a routine check-up the majority had refractive error, but DR was noted in 42.7% (29.1% +13.6%) cases. Other presenting complaints were trauma, diplopia, pain, fleshy growth, swelling, referral for laser, referral for posterior capsule rupture. Table 3 shows grade of DR with relation to various complaints. When an analysis of complaints in those with DR was done, severe NPDR and worse was found in 28.7% of cases presenting with DOV, 11.2% for routine check-up, 9% with headache, 3.6% with watering and 14.2% with other complaints. AT evaluation, No DR was seen in 464 (48.5%) cases, Mild non proliferative diabetic retinopathy (NPDR) in 100 (10.5%), moderate NPDR in 176 (18.4%), severe NPDR in 72 (7.5%), proliferative DR (PDR) in 67 (7%) and High risk PDR (HRPDR) in 77 (8.10%) cases. Clinically significant macular edema (CSME) was present amongst 73 diabetics out of 956 diabetics examined (7.63%). 244 of 956 (27.11%) diabetics, of the entire cohort, already had vision threatening DR at first presentation itself. Table 4 shows a multivariate analysis of factors associated with DR. The analysis showed that when age was >50 years there was 1.58 times higher risk of developing DR. Similarly when duration was > 5years there was 4.26 times higher risk of DR. The insulin treated group had 7.37 times risk of DR
DISCUSSION
DR is a potentially blinding condition, affecting individuals in the productive years of life. Vision loss can be prevented through timely diagnosis and treatment of DR. Regular ophthalmic evaluation to screen for DR, prior to the onset of vision loss is of utmost importance. This can be achieved by ophthalmic evaluations at remote screening camps, in diabetologists’ clinics, via telemedicine eye care institute.9As our institute caters to a large population base in southern India; we are in an ideal situation to be able to screen large number of diabetics for DR. While screening remains the ideal scenario, referral for screening by other health care providers involved in care of DM is not optimal and patients themselves rarely report for screening. The reason for which diabetics seek eye evaluations is not elucidated in literature. In this study we attempt to fill these lacunae in knowledge.
Evaluation of demographics in our cohort showed a mean age of 55.02 years, with those having DR being significantly younger (p=0.017). People in their fifties form the most productive section of society, with many holding positions of importance. Increasing prevalence of a vision threatening disease in these years can lead to decreased productivity and an increasing socio-economic burden on society.DM and its associated systemic comorbidities add to the financial burden for the patients and their family resulting in poor quality of life. Visual handicap due to DR further aggravates the physical and financial issues, whereby patients may not be able to avail optimal health care.
No statistically significant difference was seen in the proportion of DM on the basis of gender in our study, whereas a male preponderance was seen in CURES and SN DREAMS.10,11 Place of residence, education, sedentary or active occupation as well as dietary habits did not differ in the two groups.The family history was positive in 52.1% patients with DM, but this was not statistically significant. These all conclusions were similar to clinic-basedstudiesby Rema et al and Narendran et al.12, 13
The most common reason for seeking eye evaluation amongst our cohort was “diminution of vision” followed by for a “routine eye check-up”. Among the DOV group 55.5%showed some grade of DR and 28.7% had VTDR at presentation. In the routine eye check-up group majority had refractive error and/or presbyopia. Despite this 42.7% cases had DR and 11.2% had VTDR. On evaluation of diagnosis, 51% of the cohort had DR 25% had refractive error and 17% had cataract alone. The high number of refractive errors in the cohort was in concordance with the study by Narendran et al.13This data highlights the fact that patients with DM tend to report for an eye checkup only when symptomatic, with a significant number showing VTDR at presentation. Thus for a person coming for an eye check-up, possibility of having DR cannot be excluded and though lesser grades of retinopathy are expected in this scenario, presence of VTDR cannot be ruled out even in apparently asymptomatic patients. This also emphasizes that VTDR can be present at first presentation itself, increasing vision related morbidity.Our study puts a spotlight on the importance of a detailed fundus examination for every diabetic attending an eye clinic. Ophthalmologists are in a very key position to perform opportunistic screening thereby aiding prevention of vision related morbidity.
The setting of an eye clinic is also an excellent opportunity to increase DR related awareness amongst the general population. It has been proved that most of the patients of open angle glaucomaare asymptomatic and eventually present with greater degree of damage. Thus active screening for the early diagnosis is utmost important. Similar to glaucoma is the scenario with DR.14Making patients aware of the need for regular eye exams, irrespective of symptoms or clinical signs of DR at presentation can go a long way in preventing vision related morbidity. Use of information posters or videos in waiting areas, distribution of brochures and good communication with patients and their care givers can help achieve this.
Visual acuity was good (>6/18) in majority of the DR alone group, indicating a majorityof non VTDR cases. Similar good vision was found in the ‘others’ group, which comprised of people with refractive errors. Cataract alone group also showed largely better visual acuity, but the group with DR as well as cataract had more individuals with poorer vision at presentation, signifying added comorbidity due to DR in cataract.
Consistent with other studies, our population also showed an increasing prevalence of DR with increasing duration of DM, which was statistically significant (p <0.001).11,15There is an inversion of proportion of DR vs No DR in duration <5 years and >5 years. This corroborates the increasing need for regular eye evaluation in cases of DM over their lifetime. Similarly increasing age also had increasing prevalence of DR, probably secondary to longer duration of DR in older individuals.
While assessing anthropological tests we found that the BMI was inversely proportional to diabetic retinopathy, which is consistent with clinic based study of Rema et al and contrary to that shown by CURES.10,12Over time, people with longer duration of diabetes may have better diet and exercise habits. Longer duration of DM and its comorbidities may lead to weight loss and may thus explain lower BMI. The presence of systolic blood pressure >130 mmHg was strongly related to occurrence of diabetic retinopathy similar to that seen in clinic based study of Rema et al, P Namaperumalsamy et al.12,15
The mean blood sugar values as well as HbA1C was more in those with DR, suggestive of poorer systemic control contributing to occurrence of DR. UKPDS study showed that for every percentage decrease in HbA1Cthere is 35% reduction in the microvascularcomplications of DM. Thus complications of DM can be reduced improving blood sugar control. Similarly,in our studyamongst those receiving insulin for DM control, the proportion of DR was higher. Analysis showed that patients receiving insulin therapy were 7 times more likely to have DR than their counterparts. This could again be a reflection of overall poorer glycemic control in this cohort. The findings were consistent with clinic based study of Rema et al, CURES, SNDREAMS, Beaver Dam study.10,12,15,16Diabetics who need to be put on insulin therapy and those with historically poorer glycemic control form a group that needs more intense eye evaluation. This is an area where diabetologist can play a major role by ensuring all patients that are started on insulin therapy receive an immediate ophthalmic evaluation.
In our general ophthalmic clinic based population of self-reported diabetics, the percentage of DR was high; with overall proportion of DR at 51.5%,with 7% of PDR and 8.1% of HR PDR. There are very few clinic based studies carried out to determine the prevalence of DR in DM. Prevalence of DR in a study from Nepal, from a vitreo-retina center was very high at 78%.17Rema et al, in a study conducted at a diabetic center showed 34.1% prevalence of DR while a teaching hospital from Lahore, Pakistan had 33.3% prevalence of DR.12, 18In two studies conducted on self-reported diabetics, one from Japan had the prevalence of DR at 38%, while in study by Narendran it was 26.2%.13, 19
Population based studies carried out in India, where DR was diagnosed clinically with an indirect ophthalmoscope (APEDS, Narendran et al, Ramachandran et al.) or by telemedicine by evaluating fundus photographs (CURES, SNDREAMS), the prevalence of DR was lower at 12 to 22.4%.10,11,13,20,21But thepopulation based studies from western world showed higher prevalence of DR like 50.30% in the United States, 39% in the United Kingdom, 29.30% in Australia, and 28.5% in the West Indies, 52% in English town Melton and 36.8% in Beaver Dam study.22,23,24,25,26,27Overall the proportion of DR in DM attending eye clinics is higher than that in population based studies from India and the developing world, but DR proportion in clinic based study is similar to population based data from the western world. Since Aravind Eye Hospital, Pondicherry is tertiary eye care institute and main regional referral center, higher proportion of DR is to be expected in our population. The cohort would therefore be different from general population, with symptomatic cases having predominance. These factors might introduce a referral bias and thus influence the proportion of DR observed in the study. Moreover each diabetic patient was examined by retina consultants and so we believe that they were able to pick up almost all the cases of diabetic retinopathy including those with subtle changes.
Our study showed 27.11%diabetics and 49.6% of subjects with DR already had vision threatening diabetic retinopathy (VTDR) at presentation itself. The incidence is more than 26.3% of VTDR shown by the study by Huang et al.28 It implies that in developing countries like India most of the diabetics do not seek ophthalmic consultation early and thus they tend to present with VTDR and eventually compromised outcome adding to the disabilities.CSME was seen in 7.63% cases at presentation, irrespective of grade of DR.
Conclusion?
REFERENCES
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2004; 27 (Suppl 1):S5–10.
- Klein R, Klein BE, Moss SE et al. The Wisconsin epidemiological study of Diabetic retinopathy. III Prevalence and risk of diabetic retinopathy when age of onset is 30 or more years. Arch ophthalmol.1984;102:527-532
- Albert DM, Miller JW, Azar DT, Blodi BA, Cohan JE, Perkins T: Diagnosis, Management, and Treatment of No proliferative Diabetic Retinopathy. Albert &Jakobiec’s Principles & Practice of Ophthalmology, 3rd edition. Philadelphia: Saunders Elsevier; 2008.p.1776
- Kaveeshwar SA, Cornwall J. The current state of diabetes mellitus in India. Australas Med J 2014;7:45–8.
- World Health Organization. Global database on body mass index page (accessed 7 Jul 2008). Available from: https://www.who.int/bmi.
- Chylack LT, Leske MC, McCarthy D, Khu P, Kashiwagi T, Sperduto R. Lens opacities classification system II (LOCS II). Arch Ophthalmol1989; 107:991–7.
- Grading diabetic retinopathy from stereoscopic color fundus photographs-an extension of the modified Airlie House classification. ETDRS report number 10. Early Treatment Diabetic Retinopathy Study Research Group. Ophthalmology 1991;98(5 Suppl):786–806.
- Eye Diseases Prevalence Research Group. The prevalence of diabetic retinopathy among adults in the United States. Arch Ophthalmol 2004;122:552–63
- Raman R, Rani PK, Mahajan S, Paul P, Gnanamoorthy P, Krishna MS, et al. The tele-screening model for diabetic retinopathy: evaluating the influence of mydriasis on the gradability of a single-field 45 degrees digital fundus image. Telemed J E Health 2007; 13:597–602.
- Rema M, Premkumar S, Anitha B, Deepa R, Pradeepa R, Mohan V. Prevalence of diabetic retinopathy in urban India: the Chennai Urban Rural Epidemiology Study (CURES) eye study, I. Invest Ophthalmol Vis Sci 2005;46:2328–33.
- Raman R, Rani PK, Reddi Rachepalle S, Gnanamoorthy P, Uthra S, Kumaramanickavel G, et al. Prevalence of diabetic retinopathy in India: Sankara Nethralaya Diabetic Retinopathy Epidemiology and Molecular Genetics Study report 2. Ophthalmology 2009; 116:311–8.
- Rema M, Ponnaiya M, Mohan V. Prevalence of retinopathy in non insulin dependent diabetes mellitus at a diabetes centre in southern India. Diabetes Res ClinPract1996; 34:29–36.
- Narendran V, John RK, Raghuram A, Ravindran RD, Nirmalan PK, Thulasiraj RD. Diabetic retinopathy among self reported diabetics in southern India: a population based assessment. Br J Ophthalmol2002; 86:1014–8.
- Albert DM, Miller JW, Azar DT, Blodi BA, Cohan JE, Perkins T: Diagnosis, Clinical Evaluation of the Glaucoma Patient. David Dueker and Ibrahim Al Jadan. Principles & Practice of Ophthalmology, 3rd edition. Philadelphia: Saunders Elsevier; 2008.p.2481.
- Namperumalsamy P, Kim R, Vignesh TP, Nithya N, Royes J, Gijo T, et al. Prevalence and risk factors for diabetic retinopathy: a population-based assessment from Theni District, south India. Br J Ophthalmol2009; 93:429–34.
- Klein R, Klein BE, Moss SE, et al. The Beaver Dam Eye Study: retinopathy in adults with newly discovered and previously diagnosed diabetes mellitus. Ophthalmology 1992; 99:58–62.
- Thapa R, Poudyal G, Maharjan N, Bernstein PS. Demographics and awareness of diabetic retinopathy among diabetic patients attending the vitreo-retinal service at a tertiary eye care center in Nepal. Nepal J Ophthalmol2012; 4:10–6.
- Kayani H, Rehan N, Ullah N. Frequency of retinopathy among diabetics admitted in a teaching hospital of Lahore. J Ayub Med Coll Abbottabad 2003; 15:53–6.
- Kuzuya T, Akanuma Y, Akazawa Y, Uehata T. Prevalence of chronic complications in Japanese diabetic patients. Diabetes Res ClinPract 1994; 24 (Suppl):S159–64.
- Dandona L, Dandona R, Naduvilath TJ, McCarty CA, Rao GN. Population based assessment of diabetic retinopathy in an urban population in southern India. Br J Ophthalmol1999; 83:937–40.
- Ramachandran A, Snehalatha C, Vijay V, King H. Impact of poverty on the prevalence of diabetes and its complications in urban southern India. Diabet Med 2002; 19:130–5.
- Klein R, Klein BE, Moss SE. The Wisconsin epidemiological study of diabetic retinopathy: a review. Diabetes Metab Rev 1989; 5:559–70.
- Kohner EM, Aldington SJ, Stratton IM, et al, United Kingdom Prospective Diabetes Study. United Kingdom Prospective Diabetes Study, 30: diabetic retinopathy at diagnosis of non-insulin-dependent diabetes mellitus and associated risk factors. Arch Ophthalmol 1998; 116:297–303.
- Cugati S, Kifley A, Mitchell P, Wang JJ. Temporal trends in the age-specific prevalence of diabetes and diabetic retinopathy in older persons: Population-based survey findings. Diabetes Res ClinPract2006; 74:301–8.
- Leske MC, Wu SY, Hyman L, Li X, Hennis A, Connell AM, et al. Diabetic retinopathy in a black population: the Barbados Eye Study. Ophthalmology 1999; 106:1893–9.
- Sparrow JM, McLeod BK, Smith TD, Birch MK, Rosenthal AR. The prevalence of diabetic retinopathy and maculopathy and their risk factors in the non-insulin-treated diabetic patients of an English town. Eye (Lond) 1993; 7:158–63.
- Klein R, Klein BE, Moss SE, Linton KL. The Beaver Dam Eye Study. Retinopathy in adults with newly discovered and previously diagnosed diabetes mellitus. Ophthalmology 1992; 99:58–62.
- Huang OS, Tay WT, Ong PG, Sabanayagam C, Cheng C-Y, Tan GS, et al. Prevalence and determinants of undiagnosed diabetic retinopathy and vision-threatening retinopathy in a multiethnic Asian cohort: the Singapore Epidemiology of Eye Diseases (SEED) study. Br J Ophthalmol2015; 99:1614–21.
Table 1: Demographics
| Variable | DR
(n=492) |
No DR
(n=464) |
Total
(n=956) |
p-value |
| Age (in years)
Mean(SD) Range |
54.16(11.86) 10 – 87 |
55.83(9.62) 25 – 89 |
55.02(10.79) 10 – 89 |
0.017 |
| Age
<=50 >50 |
148(44.1) 344(55.5) |
188(55.9) 276(44.5) |
336(35.2) 620(64.8) |
0.001
|
| Gender
Male Female |
309(53.6) 183(48.2) |
267(46.4) 197(51.8) |
576(60.2) 380(39.8) |
0.097 |
| Residence
Rural Urban |
132(53.2) 360(50.8) |
116(46.8) 348(49.1) |
248(25.9) 708(74.1) |
0.519 |
| Type of Family
Nuclear Joint |
313(51.6) 179(51.3) |
294(48.4) 170(48.7) |
607(63.5) 349(36.5) |
– |
| Education status
Illiterate <8th Secondary Higher secondary Graduate Post Graduate |
99(52.4) 152(50.3) 115(56.4) 44(47.8) 36(45.6) 46(51.1) |
90(47.6) 150(49.7) 89(43.6) 48(52.2) 43(54.4) 44(48.9) |
189(19.8) 302(31.6) 204(21.3) 92(9.6) 79(8.3) 90(9.4) |
– |
| Type of Occupation
Active Sedentary |
158(56.4) 334(49.4) |
122(43.6) 342(50.6) |
280(29.3) 676(70.7) |
– |
| Dietary habits
Veg Non-Veg |
69(52.7) 423(51.3) |
62(47.3) 402(48.7) |
131(13.7) 825(86.3) |
– |
| Alcohol consumption
Yes No |
93(51.1) 399(51.6) |
89(48.9) 375(48.4) |
182(19.0) 774(81.0) |
– |
| Tobacco
Yes No |
62(44.6) 430(52.6) |
77(55.4) 387(47.4) |
139(14.5) 817(85.5) |
– |
| Height
Mean(SD) Range |
159.84(9.98) 130 – 187 |
159.26(9.82) 130 – 196 |
159.56(9.90) 130 – 196 |
0.372 |
| Weight
Mean(SD) Range |
64.45(13.00) 34 – 160 |
66.21(11.78) 29 – 120 |
65.30(12.45) 29 – 160 |
0.028 |
| BMI
Mean(SD) Range |
25.25(4.99) 14.70 – 74.04 |
26.19(4.70) 11.19 – 53.25 |
25.71(4.87) 11.19 – 74.04 |
0.003 |
Table 2: Complaints and diagnosis
| Complaints (%) | Diagnosis | Total | |||
| DR | Cataract | DR + Cataract | Others | ||
| Headache | 9(41) | 1(4.5) | 1(4.5) | 11(50) | 22(2.3) |
| Watering, Redness | 9(16.1) | 5(8.9) | 11(19.6) | 31(55.4) | 56(5.8) |
| Floaters | 8(40) | – | 4(20) | 8(40) | 20(2.1) |
| DOV | 155(24.6) | 133(21.1) | 195(30.9) | 148(23.4) | 631(66) |
| Routine Checkup | 62(29.1) | 21(9.9) | 29(13.6) | 101(47.4) | 213(22.3) |
| Others | 9(64.3) | 1(7.1) | – | 4(28.6) | 14(1.5) |
| Total | 252 | 161 | 240 | 303 | 956 |
Table 3: Complaints and DR grades
| Complaints (%) | DR Grade | ||||||
| No DR | Mild NPDR | Moderate NPDR | Severe NPDR | PDR | HRPDR | Total | |
| Headache | 12(54.6) | 2(9.1) | 6(27.3) | 2(9) | – | – | 22 |
| Watering, Redness | 36(64.4) | 9(16) | 9(16) | 1(1.8) | – | 1(1.8) | 56 |
| Floaters | 8(40) | 5(25) | 2(10) | – | 2(10) | 3(15) | 20 |
| DOV | 281(44.6) | 47(7.4) | 122(19.3) | 57(9.0) | 55(8.7) | 69(11) | 631 |
| Routine Checkup | 122(57.3) | 33(15.5) | 34(16) | 11(5.2) | 9(4.2) | 4(1.8) | 213 |
| Others | 5(35.7) | 4(28.7) | 3(21.4) | 1(7.1) | 1(7.1) | – | 14 |
| Total | 464 | 100 | 176 | 72 | 67 | 77 | 956 |
Table 4: Factors associated with DR
| Variable | DR | NO DR | Unadjusted OR | P-value |
| Age
<=50 >50 |
148(44.0) 344(55.5) |
188(56.0) 276(44.5) |
1.00 1.58(1.21 – 2.07) |
– 0.001 |
| Gender
Male Female |
309(53.6) 183(48.2) |
267(46.4) 197(51.8) |
1.00 1.25(0.96 – 1.61) |
– 0.097 |
| DM Duration
<=5 years >5 years |
140(33.4) 346(68.1) |
279(66.6) 162(31.9) |
1.00 4.26(3.23 – 5.61) |
– <0.001 |
| Family History
Yes No |
274(55.0) 218(47.6) |
224(45.0) 240(52.4) |
1.35(1.04 – 1.74) 1.00 |
0.022 – |
| Diet habit
Veg Non-Veg |
69(52.7) 423(51.3) |
62(47.3) 402(48.7) |
1.00 0.95(0.65 – 1.37) |
– 0.766 |
| Alcohol/Tobacco
Yes No |
127(48.3) 365(52.7) |
136(51.7) 328(47.3) |
0.84(0.63 – 1.11) 1.00 |
0.226 – |
| Insulin
Yes No |
158(85.0) 334(43.4) |
28(15.0) 436(56.6) |
7.37(4.81 – 11.28) 1.00 |
<0.001 – |
| Systolic BP
<=130 >130 |
262(47.5) 230(56.9) |
290(52.5) 174(43.1) |
1.00 1.46(1.13 – 1.89) |
– 0.04 |
| BMI
Normal Obese |
259(56.2) 233(47.1) |
202(43.8) 262(52.9) |
1.00 0.69(0.54 – 0.90) |
– 0.005 |
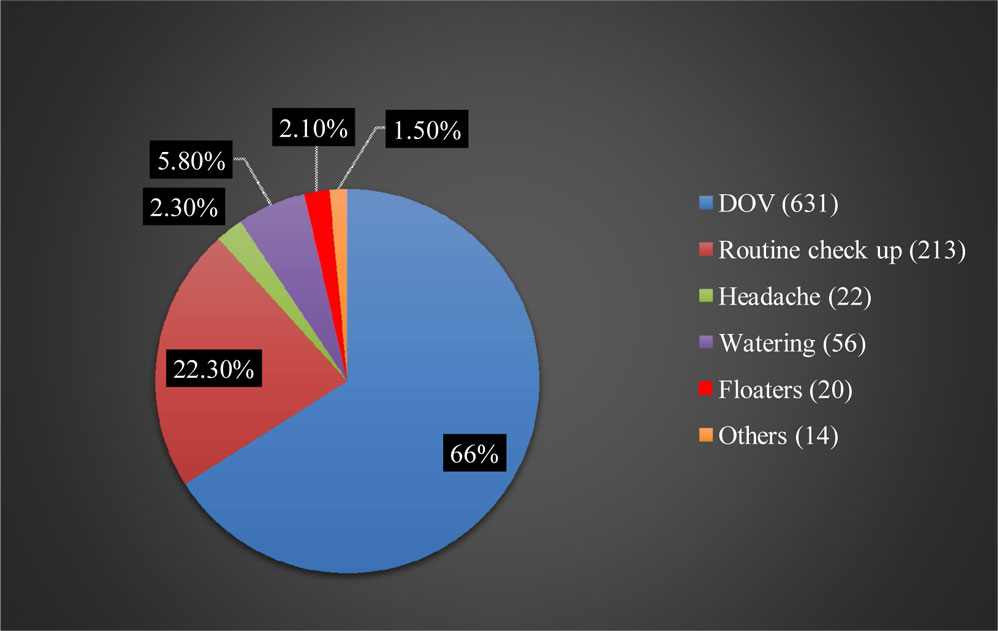
Figure 1: Spectrum of complaints
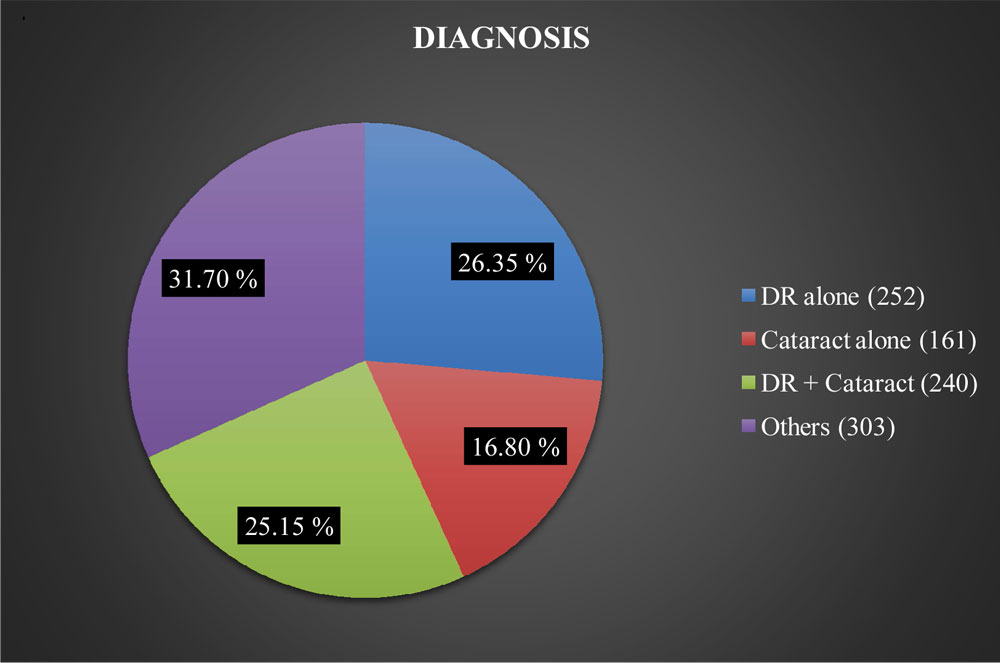
Figure 2: Diagnosis
Leave a Comment