
Dr. Virender Sachdeva, S10208, Dr. Ramesh Kekunnaya, Dr. HimanshuGoyal, Dr. Mithila Negalur
Introduction
Idiopathic intracranial hypertension (IIH) is a syndrome characterized by increased intracranial pressure of unknown cause.1It is characterized by headaches, double vision,pulsatile tinnitus, and transient visual obscurations. Many of these patients present first to ophthalmologists due to transient visual obscurations and double vision. Of these patients, majority of these have bilateral disc edema which is often severe, and marked.
However, Idiopathic intracranial hypertension treatment trial, asymmetric (> 1 Frisén grade difference) ONHE was reported in 3.6% -7.8% of patients.2-4 In a prior study, Bidot et al3 reported ONHE was strictly unilateral in 20/559 eyes (1.4%) cases. The pathophysiology of the unilateral disc edema is not so well characterized, but is believed to be secondary to anatomical differences in the optic canal, cerebral venous sinuses, etc, however, it is not so well characterized. In addition, unilateral disc edema in these
patients may often diagnostic dilemma with conditions such as papillitis or ischemic optic neuropathy. The purpose of this study is to study and compare the characteristics of the patients with unilateral and bilateral disc edema in patients with idiopathic intracranial hypertension.
Purpose:
To describe the clinical features and outcomes of unilateral idiopathic intracranial hypertension (IIH) and its characteristics in an Indian population.
Study Location
Nimmagada Prasad Children’s Eye Care Centre, LVPEI, GMRV Campus
Study Design
Retrospective review of clinical records of patients with unilateral disc edema in IIH
Methods
We reviewed case records of all patients with idiopathic intracranial hypertension seen at our institute, from 2009-2015. All cases of unilateral disc edema with a clinical suspicion of IIH underwent further analysis with Humphrey visual fields(HVF) 30-2, optical coherence tomography(OCT), MRI brain with venography and CSF analysis to confirm the diagnosis by modified Dandy-Walker criteria.
Data was collected regarding the demographic profile, clinical features, optic nerve head characteristics, diagnostic characteristics, and visual outcomes.
Results:
During the period from January 2010 to December 2015, we saw 146patients with idiopathic intracranial hypertension, of which 7 patients had unilateral disc edema (4.7%). Table 1 characterizes the baseline clinical features of these patients. As seen in table 1, majority of the patients were young women, however, only one patient was obese unlike majority of the patients with IIH. Most of these patients had a short duration of the symptoms (median 2, range 0.1 to 6 months), and majority of the patients presented with headaches, and blurred vision. None of the patients had associated cranial nerve palsy. Majority of the patients had Friséngrade II-disc edema in the affected eye and there was no disc edema in the other eye (figure 1). Initial clinical diagnosis was optic neuritis in 3 cases, ischemic optic neuropathy in 3 and optic nerve sheath tumor in 1 case was presumed.
Table 1: Showing the distribution of the clinical characteristics of the patients with unilateral IIH:
| Case no. | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| Age | 53 | 50 | 54 | 15 | 36 | 35 | 30 |
| Sex | F | F | F | F | F | F | F |
| Eye | Right | Right | Right | Right | Right | Left | Left |
| Obesity (BMI > 30) | No | Yes | No | No | No | No | No |
| Presenting Complaints | |||||||
| Blurred vision | Yes | Yes | Yes | Yes | No | Yes | Yes |
| Headache | Yes | No | Yes | Yes | No | Yes | No |
| Transient visual obscuration | No | No | No | No | No | Yes | No |
| Diplopia | No | No | No | No | No | No | No |
| Abducens nerve palsy | No | No | No | No | No | No | No |
| Grade of disc edema (Frisén scale) | IV | II | II | II | II | II | II |
Table 2 shows the change in the visual function and optic nerve characteristics of the patients at presentation and last follow-up.
| Case no | 1 | 2 | 3 | 4 | 5 | 6 | 7 | ||||||||||||||||
| Characteristics | |||||||||||||||||||||||
| BCVA at presentation | 0 | 0.1
|
0.1 | 0 | 1 | 1 | 0 | ||||||||||||||||
| BCVA at last follow-up | 0 | 0.1 | 0.1 | 0 | 1 | 1 | 0 | ||||||||||||||||
HVF at first presentation
|
|
|
|
|
|
|
|
||||||||||||||||
HVF at last presentation
|
|
|
|
|
|
|
|
Automated perimetry performed using the Humphrey visual field 30-2 SITA-Standard strategy showed an enlarged blind spot in 4 (66.7%), superior arcuate defect in 1 (16.7%), and inferior arcuate defect in 1 (16.6%) eye on the affected side and was full in the contralateral eye.
MRI brain and orbits in these patients showed signs of elevated ICP in all patients and MR venography did showed mild stenosis in all patients and significant hypoplasia of the cerebral venous sinuses in 1 patient. CSF analysis showed a bland CSF with a median CSF opening pressure of 28.3 cm of H20. All patients were treated medically with oral acetazolamide.
Figure 1. Representative photograph of the patient showing Frisén grade 4 unilateral disc edema with hyperemia and peripapillary edema in the right eye(1a) and normal disc in the left eye (1b). The same photograph shows interval reduction in the optic disc edema at 1 month (1c) and complete resolution at 3 months (1d) with oral acetazolamide therapy.
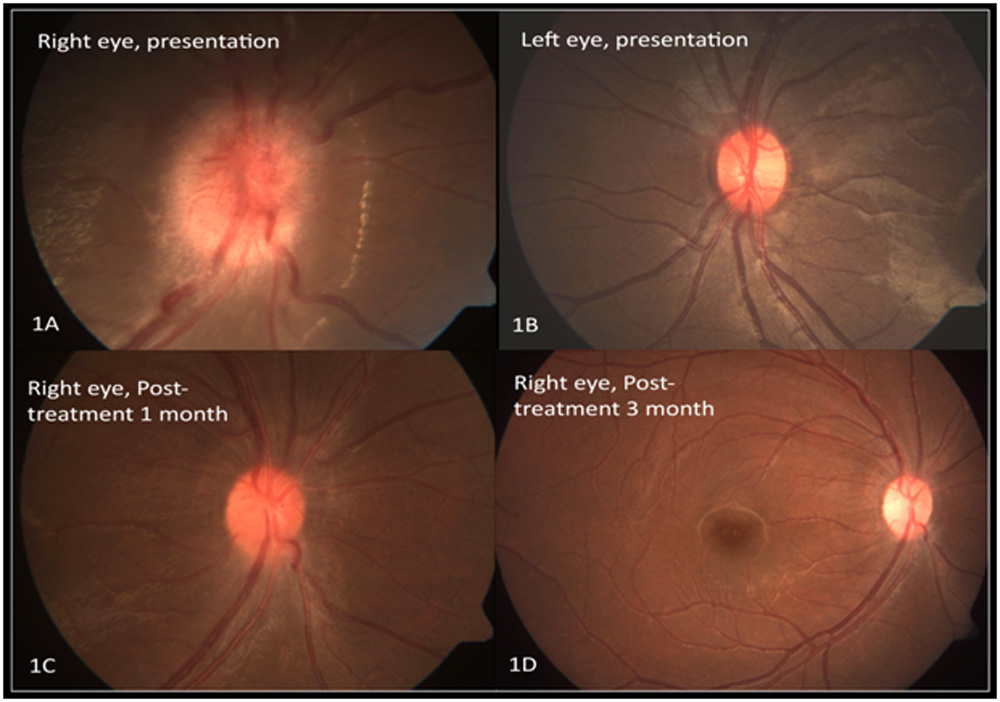
Figure 2 HVF 30-2 showing superior arcuate defect in the right eye and normal field in the left eye in the same patient
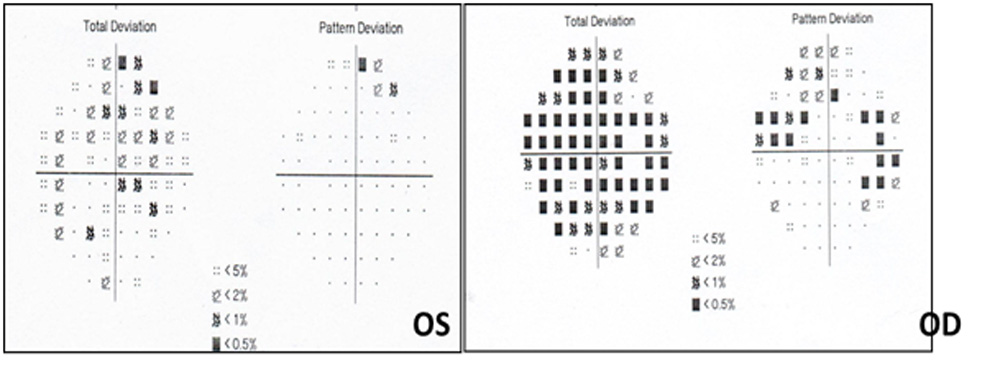
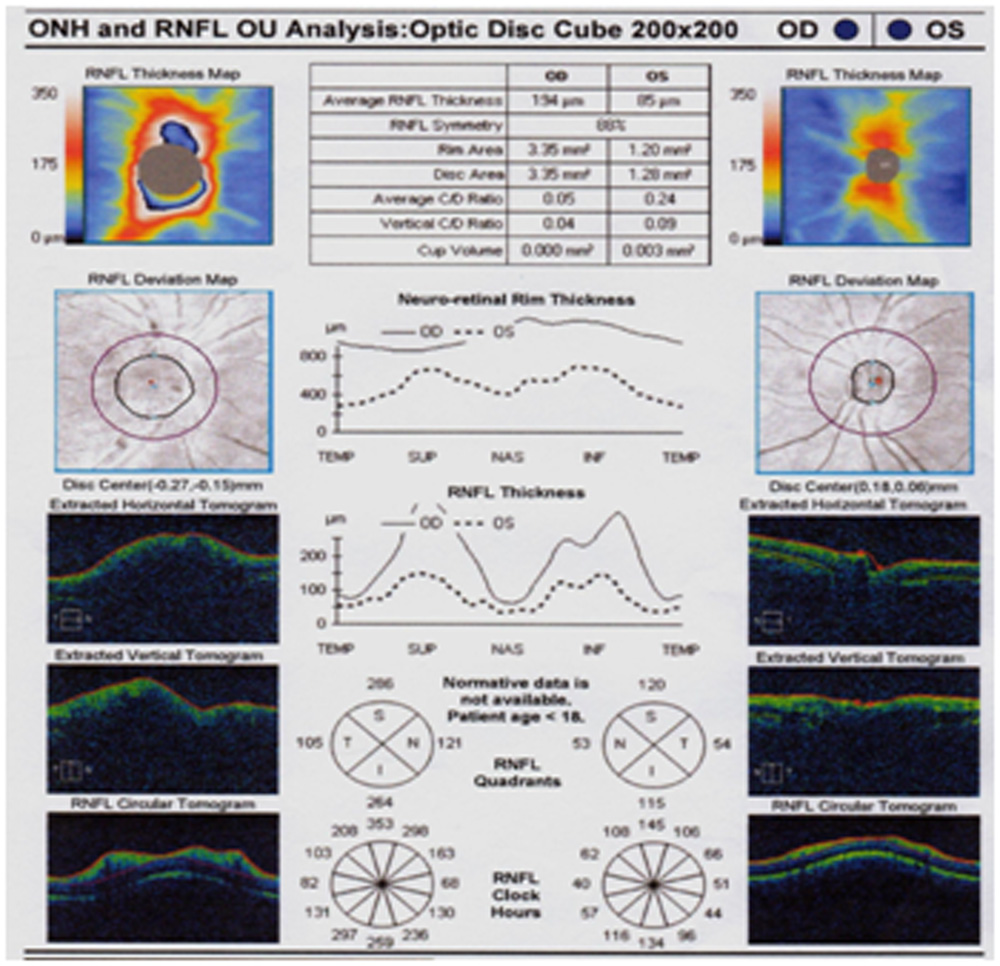
Figure 3 OCT of the peripapillary optic nerve head of patient showing disc edema with increased retinal nerve fiber layer thickness in the right eye at presentation.
Discussion
IIH with very asymmetric papilledema is not a very common phenomenon and has been reported to be present in less than 4-8% of the cases.2-4The most commonly accepted of mechanism is the asymmetric transmission of the CSF pressure to the lamina cribrosa.5
Contrasting to our demographic profile, Wall and White have found an over representation of men i.e. around 29%.3
These patients may be asymptomatic with disc edema as an incidental finding or a lower proportion of headaches compared to the bilateral group as in our study. One of the reasons attributed to this might
be the relatively lower CSF opening pressure in such patients.4
Neuroimaging studies4 of these cases with asymmetric disc edema has shown the cross-sectional optic canal measurement to be 14.9% smaller on average on the side of the lower-grade edema with more prominent signs of raised CSF pressure on the side with greater edema like our findings.
Limitations :
Retrospective study with a small sample size and lack of data on optic canal dimensions.
Conclusion:
Although papilledema secondary to IIH is expected to be bilateral and symmetric, can be highly asymmetric, and sometimes strictly unilateral among patients with IIH, raising concern for alternative diagnosis. Unlike the bilateral symmetric cases, these patients are often asymptomatic or have fewer
symptoms and are not always obese females in the child bearing age. Recognition of IIH as the underlying etiological diagnosis among patients with unilateral disc edema is important for appropriate diagnosis and timely treatment.
Bibliography :
- Friedman DI, Jacobson DM. Diagnostic criteria for idiopathic intracranialhypertension, Neurology 2002;59(10):1492–1495.
- Sedwick LA. Burde RM. Unilateral and asymmetric optic disc swelling with intracranial abnormalities. Am J Ophthalmol 1983; 96: 484-487.
- Wall M, White WN. Asymmetric papilledema in idiopathic intracranial hypertension: prospective interocular comparison of sensory visual function. Invest Ophthalmol Vis Sci 1998; 39: 134-142.
- Bidot S, Bruce BB, Saindane AM, et al. Asymmetric papilledema in idiopathic intracranial hypertension. J Neuroophthalmol 2015; 35: 31-36.
- Tso MO, Hayreh SS. Optic disc edema in raised intracranial pressure. III. Apathologic study of experimental papilledema. Arch Ophthalmol.1977;95:1448–1457
Leave a Comment