
Dr. Priyanka Patel, P17157, Dr. Vasavada Abhaykumar Raghukant, Dr. Shail, Dr. Viraj Abhayakumar Vasavada
ABSTARCT
Title: Comparison of different IOL Power calculation formulas in post myopic LASIK eyes undergoing cataract surgery
Priyanka Patel, DNB, VirajVasavada, MS, ShailVasavada, DO, DNB, FRCS, FICO, Abhay Vasavada, MS, FRCS
Purpose:To evaluate the predictive accuracy of different IOL power calculation formulae in post myopic LASIK patients undergoing cataract surgery
Methods:Retrospective observational study. Accuracy of 4 different IOL power calculation formula,Wang-Koch-Maloney, Shammas, Haigis – L and Barrett true K were evaluated in 40 eyes of 26 patients undergoing cataract surgery. All eyes had undergone myopic LASIK previously. IOL Prediction Error (PE), Absolute IOL Prediction Error(APE),Refractive Prediction Error (RPE) and Absolute Refractive Prediction Error was calculated 3 months post-operative. Percentage of eyes with Refractive prediction error within ±0.50 D and ± 1.00D were calculated.
Results:The mean IOL PE was -0.45+0.26,-0.09+0.30, 0.44+0.20 & 0.13+0.14 diopters with Wang-Koch-Maloney, Shammas, Haigis – L & Barrett true K respectively.The mean RPE was -0.35 ± 1.45,-0.1 ± 0.62,0.19 ± 0.76,0.03 ± 0.72 with Wang-Koch-Maloney, Shammas, Haigis – L & Barrett true K respectively. Mean RPE was significantly lower with Shammas and Barrett true k formula (P = 0.03). Percentage of eye within ± 0.50 D of RPE were 47.5 %, 80%, 65% and 67.5% with Wang-Koch-Maloney, Shammas, Haigis – L & Barrett true K respectively. Percentage of eye within ± 1.00 D of RPE were 67.5 %, 90%, 82.5% and 85% with Wang-Koch-Maloney, Shammas, Haigis – L & Barrett true K respectively.
Conclusion:Barrett true K and Shammas formula provided better IOL power predictability in post myopic LASIK eyes undergoing cataract surgery
Financial Disclosure: No author has a financial or proprietary interest in any material or method mentioned.
Key Words: IOL power calculation, Post LASIK cataract surgery, Myopic LASIK
Introduction
The number of patients who have had keratorefractive surgery [radial keratotomy(RK), photorefractive keratotomy (PRK), laser-assisted in situ keratomileusis (LASIK)] has increased steadily over the past few decades. Intraocular Lens (IOL)Power determination for the eyes that have had corneal refractive surgery is difficult and less accurate as compared to normal eye. 1-3IOL power calculation error in these patients can be attributed to: inaccurate determination of the true total corneal refractive power and incorrect estimation of the effective lens position (ELP) by third- or fourth-generation IOL power calculation formulas when the postoperative corneal powers are used.4,5
Over the past decade, more than 20 methods6-8like Shammas, Haigis L, Wang-Koch-Maloney, Barrett True K etc have been devised to improve the accuracy of IOL power calculation in eyes with previous refractive surgery. All methods can be divided into 3 groups according to whether the refractive surgery data are known, partly known, or not known. The data-known or data partly known methods, better known as historical methods, rely on pre-refractive corneal power and surgery data or a verified change in spherical equivalent refraction. The data-unknown methods use only the keratometric data at the initial cataract consultation or measure both anterior and posterior corneal powers directly using specialized equipment such as the slit Scheimpflug camera or optical coherence tomography (OCT). However, no standard resolution has been agreed on by surgeons worldwide.
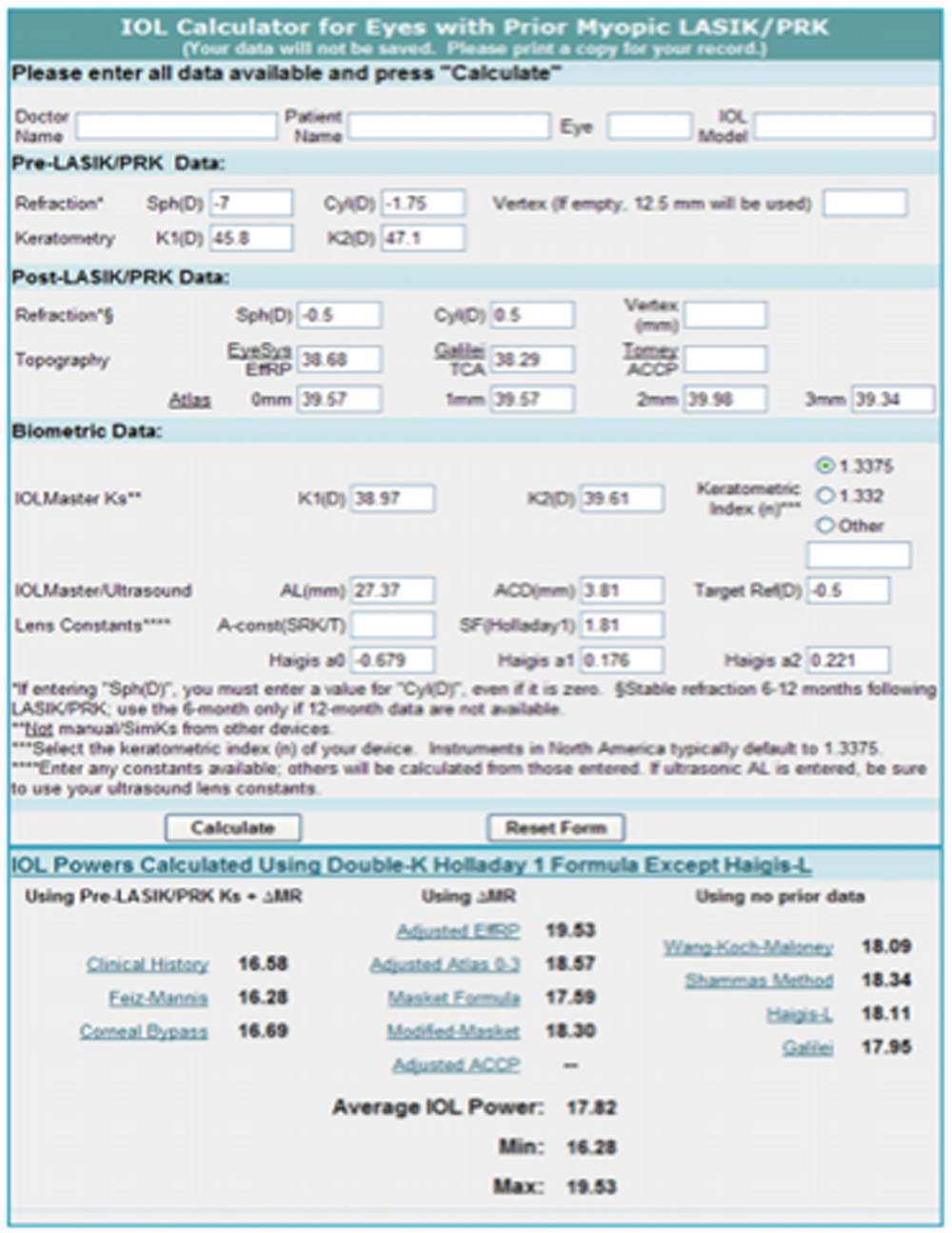
Figure – 1: Online IOL calculator for eyes with previous myopic LASIK or PRK.
At present, surgeons can perform IOL power calculations for post-refractive surgery patients without previous refractive data using several software programs. The 2 most popular are the Holladay IOL Consultant Program and the American Society of Cataract and Refractive Surgery (ASCRS) IOL Power Calculator (Figure – 1). This online calculator has 3 modules: (1) IOL power calculation for eyes with previous myopic laser in situ keratomileusis (LASIK) or excimer laser photorefractive keratectomy (PRK), (2) IOL power calculation for eyes with previous hyperopic LASIK or PRK, and (3) IOL power calculation for eyes with previous radial keratotomy (RK).
The purpose of this study was to evaluate the accuracy of various methods of IOL power prediction using ASCRS IOL power calculator after previous myopic LASIK or PRK.
Patients and methods
This retrospective study included 40 eyes that had myopic laser in situ keratomileusis (LASIK) or photorefractive keratectomy (PRK) 8 to 14 years ago and subsequently had cataract surgery from January 2012 to March 2017 at Raghudeep Eye Hospital, Ahmedabad. Eyes with a history of intraocular disease, other ocular surgeries, ocular trauma, or intraoperative complications during refractive or cataract surgery were excluded from the study.
All cataract surgeries were performed by one of the two surgeon(V.A.V, S.A.V) using the same technique of temporal clear corneal 2.2 mm incision and phacoemulsification. The preoperative examinations related to IOL power calculation included best corrected visual acuity and manifest refraction, keratometry (K) readings measured with manual keratometry and IOL master, rotating Scheimpflug imaging (Pentacam, Oculus, Inc.), corneal topography (Atlas, version 3.0.0.39, Carl Zeiss Meditec AG), lens thickness (Lenstar, LS900, Haag-Streit International), axial length (AL), anterior chamber depth (ACD), and white-to-white (WTW) distance (corneal horizontal diameter).The target refraction was determined by the surgeon’s experience and the patient’s visual needs. Preoperative parameters were entered into the ASCRS IOL Power Calculatorto calculate IOL power. All previous clinical history data, such as pre-refractive surgery corneal power and pre-refractive and post-refractive surgery refractions (before the onset of cataract), were unavailable. The surgeon selected the IOL power to be implanted based on his judgment in terms of the target refraction and the IOL powers predicted by these methods.
Methods Used for Intraocular Lens Power Calculation:
Following are the ASCRS IOL power calculator methods that use current pre-cataract surgery data:
1. Wang-Koch-Maloney. This method was developed based on the modified Maloney formula using converted anterior central corneal power from corneal topography.9To cover more points over the central ablated area, the mean annular corneal power, determined by Atlas 0.0 to 3.0 mm measurements, is used as follows:
Adjusted corneal power = 1.114 × (Atlas 0 to 3) – 5.59
2. Shammas with Regression Analysis.10This method calculates the post-LASIK or PRK corneal power by adjusting the measured post-LASIK or PRK K values. In the IOL calculator,9the Atlas 0.0 to 3.0 mm ring average K value is used as the post-LASIK or PRK K-value as follows:
Adjusted corneal power = 1.14 × post – LASIK/PRK K – 6.8
3. Haigis-L.11This algorithm modifies the measured corneal radius (Rmeas) of curvature by the IOLMaster based on regression analysis and then determines the corrected corneal radius of curvature (Rcorr) and calculates IOL power using the regular Haigis formula as follows12:
Rcorr = 331.5/ (- 5.1625 × Rmeas + 82.2603 – 0.35)
4. Barrett true K no history method:
Intraocular Lens Prediction Error
The manifest refraction after cataract surgery was obtained at the most recent examination (range 3 weeks to 1 year). IOL prediction error was obtained by subtracting the IOL power calculated by each formula from the power of the IOL implanted. Thus, a positive value indicates that method predicts an IOL of lower power than the power of the implanted IOL; this would leave the patient hyperopic.
The following results were evaluated:
1. Mean arithmetic IOL prediction error. Positive values indicate the method underestimated the IOL power. Negative values indicate the method overestimated the IOL power.
2. Mean absolute IOL prediction error.
3. Percentage of eyes within a certain refractive prediction error. Using the assumption that 1.00 D of IOL prediction error produces 0.70 D of refractive error at the spectacle plane,13the percentage of eyes within a refractive prediction error of ± 0.50 D and within ± 1.00 D were computed for each method.
Statistical Analysis
The 1-sample t test was used to determine whether the mean arithmetic IOL prediction errors produced by various methods were significantly different from zero. The percentages of eyes within certain refractive prediction errors were compared using the chi-square test. The Bonferroni correction was applied for multiple tests. Statistical analysis was performed using SPSS for Windows software (version 15.0, SPSS, Inc.). A P value less than 0.05 was considered statistically significant.
Results
The study comprised 40 eyes of 26 patients undergoing cataract surgery with history of myopic LASIK/PRK done. Pre LASIK/PRK refractive data was not available for any patient.
Demographic data(Table- 1):
Mean age of all patients was 48.2 ± 6.48 (years ± SD, Range :37 to 60). Out of 40 patients 25 (62.5 %) were females and 15 (37.5%) were males (Figure 2).Mean axial length was 26.87 ± 2.67 mm (mean ± SD).
| Table -1 : Demographic Data | |
| Mean age ± SD | 48.2 ± 6.48 (range : 37 – 60) |
| Mean AL ± SD | 26.87 ± 2.67 mm |
Intraocular Lens Prediction Error:
| Table – 2 : IOL Prediction Error (D) | ||||
| Arithmetic | Absolute | |||
| Mean ± SD | Range | Mean ± SD | Range | |
| Wang-Koch-Maloney | -0.41 ± 2.04 | -7.82 to 3.07 | 1.3 ± 1.62 | 0.04 to 7.82 |
| Shammas | -0.15 ± 0.88 | -2.83 to 2.16 | 0.56 ± 0.69 | 0 to 2.83 |
| Haigis-L | 0.28 ± 1.09 | -2.88 to 3.37 | 0.83 ± 0.76 | 0.02 to 3.37 |
| Barrett true K no history method | 0.05 ± 1.04 | -3.29 to 1.89 | 0.69 ± 0.76 | 0 to 3.29 |
| P value | 0.12 | 0.013 | ||
| PE – Prediction Error, SD – Standard Deviation | ||||
Table -2 shows the mean IOL prediction errors and mean absolute IOL Prediction error with each formula.Mean arithmetic IOL Prediction error with Wang-Koch-Maloney, Shammas, Haigis- L and Barrett true K no history method was -0.41 ± 2.04, -0.15 ± 0.88, 0.28 ± 1.09 and 0.05 ± 1.04, respectively. Mean IOL PE was least with the Shammas formula followed by Barrett true K no history method. Difference of mean IOL PE was not statistically significant between different formulas (P = 0.12). Mean absolute IOL prediction error with Wang-Koch-Maloney, Shammas, Haigis- L and Barrett true K no history method was 1.3 ± 1.62, 0.56 ± 0.69, 0.83 ± 0.76 and 0.69 ± 0.76 respectively. Mean absolute IOL PE was minimum with the Shammas formula with a statistically significant difference (P = 0.013).
Refractive Prediction Error:
| Table – 3 : Refractive Prediction Error (D) | ||||
| Arithmetic | Absolute | |||
| Mean ± SD | Range | Mean ± SD | Range | |
| Wang-Koch-Maloney | -0.35 ± 1.45 | -5.47 to 2.15 | -0.97 ± 1.12 | 0.03 to 5.47 |
| Shammas | -0.1 ± 0.62 | -1.98 to 1.51 | 0.39 ± 0.48 | 0 to 1.98 |
| Haigis-L | 0.19 ± 0.76 | -2.02 to 2.36 | 0.57 ± 0.53 | 0.01 to 2.36 |
| Barrett true K no history method | 0.03 ± 0.72 | -2.3 to 1.32 | 0.49 ± 0.53 | 0 to 2.3 |
| P value | 0.03 | 0.002 | ||
| RPE – Refractive Prediction Error, SD – Standard Deviation | ||||
Table – 3 shows mean refractive prediction error (RPE) and mean absolute refractive prediction error for each formula. Mean arithmetic RPE was -0.35 ± 1.45, -0.1 ± 0.62, 0.19 ± 0.76 and 0.03 ± 0.72 with Wang-Koch-Maloney, Shammas, Haigis- L and Barrett true K no history method, respectively and mean absolute RPE was -0.97 ± 1.12, 0.39 ± 0.48, 0.57 ± 0.53 and 0.49 ± 0.53 with Wang-Koch-Maloney, Shammas, Haigis- L and Barrett true K no history method, respectively. Mean arithmetic RPE was minimum with the Shammas and Barrett true K no history method. Difference of mean RPE between different methods was statistically significant for both mean arithmetic RPE (p=0.03) and mean absolute RPE (p=0.002).
Percentage of eyes within a certain refractive prediction error:
| Table – 4: Percentage of Eyes within a certain Refractive Prediction Error | |||
| <± 0.50 D | <± 1.00 D | >± 1.00 D | |
| Wang-Koch-Maloney | 47.5 | 67.5 | 32.5 |
| Shammas | 80 | 90 | 10 |
| Haigis – L | 65 | 82 | 17.5 |
| Barrett true K no history method | 67.5 | 65 | 15 |
| P value | >0.05 | >0.05 | >0.05 |
Table -4 shows percentage of eyes within ± 0.50 D, ± 1.00 D and >± 1.00 D of refractive prediction error. Percentage of eyes within ± 0.50 D of refractive prediction error were 47.5%, 80%, 65 % and 67.5 % with Wang-Koch-Maloney, Shammas, Haigis- L and Barrett true K no history method, respectively. Percentage of eyes within ± 1.00 of refractive prediction error were 67.5 %, 90%, 82.5% and 85 % with Wang-Koch-Maloney, Shammas, Haigis- L and Barrett true K no history method, respectively. Only 32.5 %, 10%, 17.5% and 15 % of the eyes were having RPE of >± 1.00 D with Wang-Koch-Maloney, Shammas, Haigis- L and Barrett true K no history method, respectively. 90 % of the eyes with Shammas formula were having RPE within ±1.00 D however the difference was not statistically significant (p >0.05).
Discussion
Accurate IOL power calculation after corneal refractive surgery is an important clinical problem. Various methods have been proposed in the literature for the accurate IOL power calculation for this situation. The purpose of this study was to evaluate the accuracy of various methods of IOL power prediction after myopic LASIK/PRK in consecutive cases. In present study we compared 4 different formulas i.e. Wang-Koch-Maloney, Shammas, Haigis – L and Barrett true K no history methods which are available on ASCRS online calculator.
All methods produced mean arithmetic IOL prediction errors close to zero except for the Wang-Koch-Maloney method. The Wang-Koch-Maloney method predicted a higher IOL power by 0.41 D on average than the IOL power implanted. The Haigis -L method predicted a lower IOL power by 0.28 D than the IOL power implanted and would leave the patient hyperopic. Barrett True K no history method has least mean arithmetic IOL PE (0.05 ± 1.04) followed by Shammas formula (-0.15 ± 0.88).
With the assumption that 1.00 D of IOL prediction error produces 0.70 D of refractive error at the spectacle plane,13the refractive prediction error were significantly lower with Shammas and Barrett True K no history method. In normal eyes, benchmark standards for refractive outcomes after cataract surgery have been established in the National Health Service of the United Kingdom.14These standards are 55% of eyes achieving refraction within ±0.50 D of the predicted refraction and 85% of eyes achieving refraction within ±1.00 D of the predicted refraction.All formulas except Wang-Koch-Maloney fulfilled these criteria in our study, Shammas formula has maximum number of eyes having refractive prediction error within ±1.00 D.
Abulafia et al15 compared 8 different formulas of IOL power calculation for post myopic LASIK /PRK eyes and they showed that Barrett true K formula has the highest percentages of eyes with RPE within ± 0.50 D and ± 1.00 D. they showed that Barrett true K formula is the most accurate method for IOL power calculation in post LASIK/PRK eyes. On the other side a meta-analysis of different formulas done by Savini et al16 showed that in eyes where no preoperative data available, Shammas formula gave the most accurate IOL power calculation. results of our study are comparable with the results of these both studies. We found Shammas and Barrett True K no history method are equally effective for IOL power prediction.
In the study done by yang et al17, 8 methods (Holladay 2 PCI-K, Holladay 2 FlatK, Wang-Koch-Maloney, Shammas No-History, Haigis – L, ASCRS-Average, ASCRS-Min, and ASCRS-Max) were analysed and compared. They showed that of these 8 methods, the Holladay 2 Flat K method provided the most accurate prediction for IOL power calculation with the smallest mean absolute IOL prediction error, the smallest refractive prediction error, the smallest variances, and the greatest percentage of eyes within ± 0.50 D (58%) and ± 1.00 D (90%) of the refractive prediction error.
Traditionally, the clinical history method has been used as the standard, and historical data has been considered critical in eyes with previous corneal refractive surgery. In 2010, Wang et al18showed that ASCRS IOL Power Calculator methods using surgically induced refraction (Masket formula, adjusted Atlas corneal topography 0.0 to 3.0 mm, adjusted effective refractive power, and modified Masket) and methods using no previous data (Wang-Koch-Maloney, Shammas, and Haigis-L) gave better results than methods using whole clinical history data (clinical history, Feiz-Mannis, Corneal Bypass). In our study where no clinical history is available, we found that Shammas formula and Barrett True K No History methods are the most accurate methods. Limitations of our study were: (1) the smaller sample size (40 eyes/26 patients) (2) the IOL constants we used werenot personalized.
In conclusion, when previous refractive surgery data are unavailable, the IOL power prediction with the Shammas and Barrett true K method seems to be the most accurate of the methods offered by ASCRS IOL Power Calculator.
References:
- Koch DD, Liu JF, Hyde LL, Rock RL, Emery JM. Refractivecomplications of cataract surgery after radial keratotomy. Am J Ophthalmol 1989; 108:676–682
- Seitz B, Langenbucher A, Nguyen NX, Kus MM, Ku¨chle M. Underestimation of intraocular lens power for cataract surgery after myopic photorefractive keratectomy. Ophthalmology 1999; 106:6936–702
- Gimbel HV, Sun R. Accuracy and predictability of intraocularlens power calculation after laser in situ keratomileusis. J Cataract Refract Surg 2001; 27:571–576
- Aramberri J. Intraocular lens power calculation after corneal refractive surgery: double-K method. J Cataract Refract Surg 2003; 29:2063–2068
- Koch DD, Wang L. Calculating IOL power in eyes that have hadrefractive surgery [editorial]. J Cataract Refract Surg 2003; 29:2039–2042
- Masket S, Masket SE. Simple regression formula for intraocularlens power adjustment in eyes requiring cataract surgery after excimer laser photoablation. J Cataract Refract Surg 2006; 32:430–434
- Holladay JT. Consultations in refractive surgery [comment]. Refract Corneal Surg 1989; 5:203
- Wang L, Hill WE, Koch DD. Evaluation of intraocular lens powerprediction methods using the American Society of Cataract and Refractive Surgeons post-keratorefractive intraocular lens power calculator. J Cataract Refract Surg 2010; 36:1466–1473
- Wang L, Booth MA, Koch DD. Comparison of intraocular lenspower calculation methods in eyes that have undergone LASIK. Ophthalmology 2004; 111:1825–1831
- Shammas HJ, Shammas MC. No-history method of intraocular lens power calculation for cataract surgery after myopic laser in situ keratomileusis. J Cataract Refract Surg 2007; 33:31–36
- Haigis W. Intraocular lens calculation after refractive surgery formyopia: Haigis-L formula. J Cataract Refract Surg 2008; 34:1658–1663
- .Haigis W, Lege B, Miller N, Schneider B. Comparison of immersion ultrasound biometry and partial coherence interferometry for intraocular lens calculation according to Haigis. Graefes Arch ClinExpOphthalmol 2000; 238:765–773
- Feiz V, Mannis MJ, Garcia-Ferrer F, Kandavel G, Darlington JK, Kim E, Caspar J, Wang J-L, Wang W. Intraocular lens power calculation after laser in situ keratomileusis for myopia and hyperopia: a standardized approach. Cornea 2001; 20:792–797
- Gale RP, Saldana M, Johnston RL, Zuberbuhler B, McKibbinM.Benchmark standards for refractive outcomes after NHS cataract surgery. Eye 2009; 23:149–152
- Adi Abulafia, MD, Warren E. Hill, MD, Douglas D. Koch, MD, Li Wang, MD, PhD, Graham D. Barrett, MD.Accuracy of the Barrett True-K formula for intraocular lens power prediction afterlaser in situ keratomileusis or photorefractive keratectomy for myopia. J Cataract Refract Surg2016; 42:363–369
- Giacomo Savini, MD, Piero Barboni, MD, Michele Carbonelli, MD,Pietro Ducoli, MD, Kenneth J. Hoffer, MD Intraocular lens power calculation aftermyopicexcimerlasersurgery:Selectingthe best method using available clinical data. J Cataract Refract Surg 2015; 41:1880–1888
- Ruibo Yang, MD, Annie Yeh, OD, Michael R. George, MD, Maria Rahman, BS, Helen Boerman, OD, FAAO, Ming Wang, MD, Ph, Comparison of intraocular lens power calculation methods after myopic laser refractive surgery without previous refractive surgery data. J Cataract Refract Surg 2013; 39:1327–1335
- Wang L, Hill WE, Koch DD. Evaluation of intraocular lens powerprediction methods using the American Society of Cataract and Refractive Surgeons post-keratorefractive intraocular lens power calculator. J Cataract Refract Surg 2010; 36:1466–1473
Leave a Comment