
Dr. Anna Elias, A06573, Dr. Mekhla Naik, Dr. Marian Anne Jacob
Aim: The purpose of the study was to present the diversity of clinical presentations and treatment options for ocular amyloidosis.
Method: A retrospective study of five patients, diagnosed to have ocular amyloidosis on histopathological examination between 2011 and 2017 at a tertiary referral center was carried out.
Results:The case series included five patients [three males and two females].The average age of the patients was 52 years. Of the five patients, three presented witha mass lesion,one with blepharoptosis and one with lid swelling. HPE in all five cases proved to be amyloidosis.The main treatment was surgical excision with tissue biopsy. None of the patients had systemic involvement.
Conclusion: Ocular amyloidosis has a varied clinical presentation,commonly involving lids and conjunctiva. As amyloidosis can mimic a variety of conditions,histopathological examination is essential to confirm the diagnosis.Systemic involvement,including malignancies has to be thoroughly investigated.
Introduction
Amyloidosis is a spectrum of disorders characterized by the deposition of amyloid, an extra cellular protein in an abnormal fibrillar form, with highly characteristic histopathological staining properties.[1] Mathias Schleiden, a German botanist first used the term amyloid in 1838 in his description of plant histology. Virchow in 1854, began contemporary medical use of this term in neuroanatomy and described its characteristics in liver autopsies.[2]Amyloid proteins are deposited as insoluble fibrils as a consequence of abnormal protein folding, detected on electron microscopy as non branching, rigid and mostly extracellular. The clinical presentation can vary from a focal, localized lesion with minor clinical consequences to extensive systemic disease that can involve any organ system of the body leading to severe pathophysiological damage. Ocular amyloidosis has been reported in almost every part of the eye. Amyloidosis of the eye can occur as a localized mass or as part of a systemic disorder. The gold standard of amyloid detection is the demonstration of apple-green birefringence on Congo red staining when viewed with polarized light.[3][Fig.1,2] In haematoxylin and eosin staining, amyloid appears eosinophilic.[Fig.3] Historical guidelines promoted a classification based on clinical presentation and consisted of four subtypes: primary localized amyloidosis (most common), primary systemic amyloidosis, secondary localized amyloidosis and secondary systemic amyloidosis.[4] With advances in protein sequence analysis, recent guidelines recommend greater classification based on the specific precursor(A-) of each individual amyloid protein.[5] Broadly these amyloid proteins can be classified into Immunoglobulin light chains (AL) in primary systemic amyloidosis, Amyloid A protein(AA) in secondary amyloidosis, Transthyretin in familial amyloidosis and Amyloid P component(AP). As amyloidosis can affect any part of the eye, ocular signs and symptoms include lid malposition, globe displacement, abnormal motility, diplopia, ptosis, recurrent subconjunctival haemorrhage, conjunctival mass, corneal opacity, raised intraocular pressure, vitreous opacities, and abnormal fundus appearance. Ocular amyloidosis is a rare clinical entity. Eyelid or conjunctival amyloidosis usually present as a mass or diffuse thickening of the eyelids or conjunctiva. Having a varied presentation, it could be misdiagnosed and systemic evaluation may be forfeited. Hence we decided to study the clinical characteristics of patients who had presented at our institution and were diagnosed as ocular amyloidosis.
Aim
The purpose of the study was to present the diversity of clinical presentations, treatment options and to evaluate the prognosis of ocular amyloidosis.
Subjects and Methods
A retrospective study of five patients diagnosed to have ocular amyloidosis on histopathological examination between 2011 and 2016 at our institution which is a tertiary referral eye care center, was done. We reviewed the case records of patients with ocular amyloidosis, with special emphasis on clinical presentation, surgical management and histopathological diagnosis. We compared our findings with those reported in the literature.
Results
Illustrative case series.
Patient 1 [Figure 4]
A 46-year-old lady presented with drooping of the upper eyelid of the right eye. Examination revealed an irregular, yellow coloured mass involving the upper palpebral conjunctiva, resulting in ptosis of moderate intensity. An incisional biopsy was done. Surgery showed a diffuse mass infiltrating the tarsus and muscle. Histopathological examination (HPE) confirmed the mass as conjunctival amyloid. Evaluation for systemic amyloidosis was negative.
Patient 2
A 29-year-old lady presented with a swelling involving the lower lid of the left eye for the past six years. An excisional biopsy of the mass was done through a subciliary incision. The mass was adherent to the conjunctiva and tarsus. HPE of the mass was reported as conjunctival amyloidosis.
Patient 3 [Figure 5]
A 48-year-old man presented with a mass involving the conjunctiva near the lateral canthus of the left eye. He was a known diabetic for the past three years. Excision biopsy of the mass was done. HPE of the mass proved to be conjunctival amyloidosis. He presented with recurrence of the mass involving the superior, inferior and lateral fornix of the left eye and a conjunctival mass in the right eyetwo years later. Excision biopsy with cryotherapy and amniotic membrane graft was performed in the left eye. The biopsy was consistent with conjunctival amyloidosis. Systemic evaluation for amyloidosis and multiple myeloma were negative.
Patient 4 [Figure 6]
A 67-year-old man presented with a swelling involving the margin of the lower lid of the left eye of one-month duration. The mass was firm, measuring 11 x 6 mm and extending into the tarsal conjunctiva. The meibomian gland orifices were occluded. Wedge resection and biopsy of the mass was done. HPE of the mass was reported as conjunctival amyloidosis. Evaluation for systemic amyloidosis was negative.
Patient 5 [Figures 7,8]
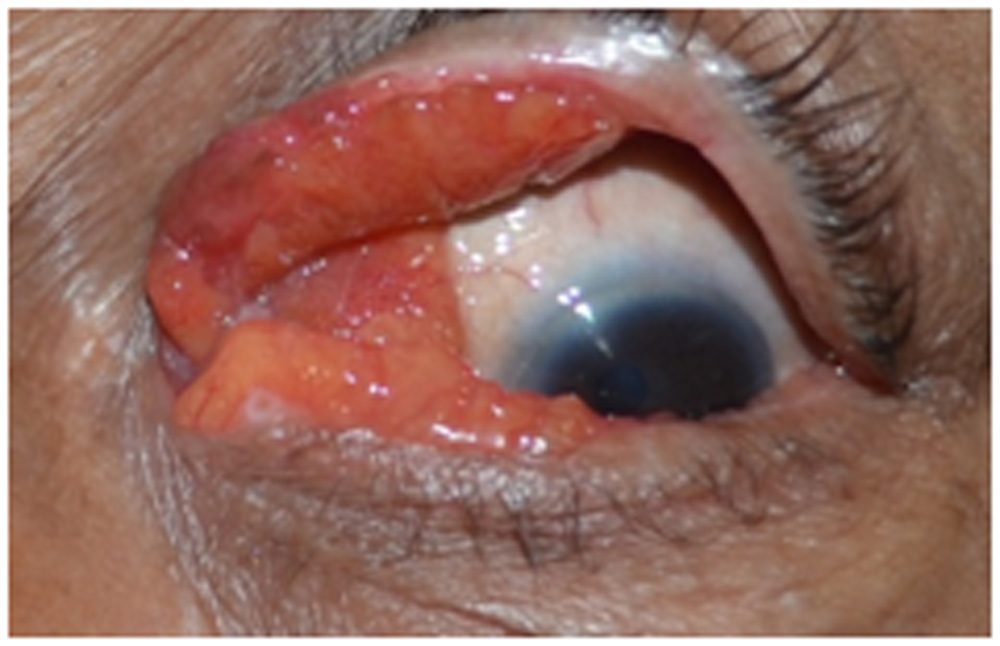
A 70-year-old man had presented with defective visionand pain in the right eye and swelling of the lids and conjunctiva in both eyes. He was a diabetic for the past twelve years. His BCVA was CF 1m, less than N36 in the right eye and 6/6 N6 in the left eye. Both eyes were pseudophakic. He had pseudophakic bullous keratopathy in the right eye. Both eyes appeared to have giant papillary conjunctivitis. An incisional biopsy of the left eye was done which proved to be conjunctival amyloidosis. He had conjunctival amyloidosis of both eyes. A corneal opacity developed in the left eye. His vision dropped to 6/36<N36 in the left eye. Debulking of amyloid tissue in both the lids and fornices was done. Cryotherapy was applied. The raw area was covered with amniotic membrane. He developed entropion of the left eye. The corneal edema of the left eye worsened. Entropion correction and release of symblepharon was done for the left eye. The corneal edema reduced and his vision improved to 6/12N6 in the left eye. Systemic evaluation for amyloidosis was negative.
In summary, five patients were included in the study. There were 3 (60%) males and 2 (40%) females. The average age of the patients was 52 +16.08years. One (20%) patient presented with blepharoptosis, 2(40%) patients with a swelling of the lids involving one eye, one(20%) patient with a conjunctival mass in both eyes and one (20%) patient with bilateral conjunctival masses, corneal decompensation in one eye and a corneal opacity in the other eye. Four[80%] of the five patients did not had systemic amyloidosis. One patient did not report with the results of systemic evaluation. An incisional biopsy and surgical debulking was done for the patient with ptosis. Excisional biopsy was performed in three patients with the lid or conjunctival masses. Wedge resection was performed in one patient with a lid mass. In the patient with bilateral conjunctival amyloidosis, excisional biopsy was done in both eyes and cryotherapy and amniotic membrane grafting was performed in one eye. Incisional biopsy and debulking of the mass was performed in the patient with bilateral conjunctival amyloidosis and corneal decompensation. All the patients had conjunctival amyloidosis, either localized or diffuse form.
Discussion
Amyloidosis is a rare disease and ophthalmic manifestations are uncommon. Amyloidosis has a varied presentation. In our study we have reported five patients who presented with varying ocular signs and symptoms such a ptosis, swelling of the lids, conjunctival mass and corneal opacities. The largest case series of ocular and periocular amyloidosis was reported by Liebovitch et at. (6) Their study included 24 patients [15 females and 9 males] with a mean age of 57+17 years. In our study of five patients, 3[60%] were males and 2[40%] females. The mean age of our patients was 52+16.08 years. In their study, clinical signs and symptoms included a visible or palpable periocular mass or tissue infiltration [95.8%], ptosis [54.2%], periocular discomfort or pain [25%], proptosis or globe displacement [21%] limitations in ocular motility [16.7%], recurrent periocular subcutaneous haemorrhages [12.5%] and diplopia [8.3%] with orbital involvement [7 cases] and periocular involvement [17 cases]. In our study one [20%] patient presented with ptosis and four [80%] patients presented with periocular masses, namely, swelling involving lids and conjunctiva.
Amyloidosis can affect almost all ocular and periocular structures. The conjunctiva is involved in a majority of patients [6]. Conjunctival amyloidosis mainly affects the fornices and most commonly the superior fornix and tarsal conjunctiva[7]. Conjunctival amyloidosis is usually a localized process, that is rarely associated with systemic involvement. Local amyloidosis can be caused by deposition of monoclonal immunoglobulin light chains (K or λ), usually by benign B-cell or plasma cell clones. [8]
Conjunctival amyloidosis is commonly seen in middle aged adults. It can present as confluent fusiform lesions or polypoidal papules that have a waxy or yellow colour. [9] In most patients, the palpebral conjunctiva is involved. Patients may present with ocular symptoms that simulate conjunctival malignancies such a lymphoma,leukemia,metastatic malignancies or inflammation. Furthermore, conjunctival malignancies may lead to amyloid deposition.
Secondary conjunctival amyloidosis is the deposition of amyloid as a result of an antecedent local conjunctival disorder such as trachoma. [10]Additionally certain diseases such as lymphoma, rheumatoid arthritis, Churg-Strauss syndrome, syphilis, hypothyroidism and Addison disease have shown an association with conjunctival amyloidosis. [11] Conjunctival amyloidosis can rarely be associated with primary systemic amyloidosis. Of 50 patients previously published in literature only 3[6%] were reported to have primary systemic amyloidosis. [12] [13]
Shields and associates reported a 56 year old man who presented with a fleshy hemorrhagic lesion of the semilunar fold of the left conjunctiva.[7] Subsequent systemic evaluation disclosed primary systemic amyloidosis with involvement of bonemarrow, liver and kidney. It is necessary to evaluate every patient with conjunctival amyloidosis for systemic amyloidosis. Baseline investigations include complete blood count, serum electrolytes, 24-hour urine protein, urine analysis for BenceJones protein, immune electrophoresis and immune fixation of the serum and urine, renal and liver function test, echocardiography, ultrasound of the abdomen, and skeletal survey. Primary systemic amyloidosis is considered if there is nephrotic range proteinuria (nondiabetic), cardiomyopathy (non-ischaemic), hepatomegaly and peripheral neuropathy. The suspicion is heightened if monoclonal protein is detected during immunelectrophoresis of serum or urine. The diagnosis is confirmed by biopsy of subcutaneous fat aspirate, bone marrow biopsy or rectal biopsy stain with Congo red [90% sensitive].
The demographic pattern of primary conjunctival amyloidosis is different from primary systemic amyloidosis. A review of 229 patients found that primary systemic amyloidosis occurred at a mean age of 65 years and had a male preponderance. [14] In contrast, the mean age of localized conjunctival amyloidosis in published 44 patients was 48 years.[12][13] In our study the mean age was 52+16.08 years with a male preponderance. None of our patients who had systemic evaluation had systemic amyloidosis.
The final diagnosis of amyloidosis requires tissue biopsy that shows the pathognomonic red-green dichroism after staining with Congo red and viewing in intense unidirectional polarized light.[15] With Congored, amyloid shows two phenomena, first is apple-green birefringence, which indicates the ability of amyloid to rotate a plane of polarized light exactly 90°. The second is dichroism, which if green light is plane-polarized parallel to the long axis of the amyloid protein, it gives the deposit a bright green colour. When the green light is plane- polarized perpendicularly to the long axis of the amyloid protein, it gives the deposit a dull red colour.[16] Shields et al, in their review of six cases of conjunctival amyloidosis reported that immunehistochemistry staining in three patients of localized conjunctival amyloidosis showed monoclonal light chains of IgDlambda, IgA lambda or IgG Kappa. [17]Amyloid deposits may be of AL type associated with local monoclonal B cell or plasma cell proliferation. It is postulated that amyloid protein can accumulate in the conjunctiva as a localized immunological reaction to foreign antigenic material.[18] Serum amyloid P component scintigraphy [SAP] is a technique developed for specific evaluation and diagnosis of amyloidosis. Serum amyloid P component is a glycoprotein that is highly concentrated in all amyloid deposits. Using iodine 123- labeled SAP can show specific uptake in various organs including the orbits. Measuring SAP retention and intensity of organ uptake has diagnostic sensitivity and specificity to amyloidosis and for monitoring the effect of treatment. [15]
The clinical differential diagnosis of conjunctival amyloidosis includes lymphoma, leukemia, metastatic carcinoma, sarcoidosis, papilloma, melanoma and sebaceous carcinoma. [9] The smooth pink appearance of amyloidosis is similar to lymphoma or leukemia. However palpebral conjunctival involvement and haemorrhages are rare with lymphoma. [19]
The management of conjunctival amyloidosis depends on the extent of local involvement and the systemic status of the patient. Conservative management with ocular lubricants is useful. Extensive conjunctival infiltration is difficult to treat and supportive therapy is the only option available. Excision of solitary lesions or debulking of diffuse lesions can relieve symptoms caused by the mass effect of the amyloid deposits. There have been no significant advances in the treatment of localized amyloidosis. Surgical debulking remains the main treatment modality.[15] In most cases, complete surgical excision is not possible and the aim of treatment is relief of symptoms, restoration of function and prevention of ocular morbidity. Among the five patients in our study, surgical excision was performed in three patients and surgical debulking in two patients. One patient showed recurrence of amyloidosis. In the study by Leibovitch et al, half their cases were treated with surgical debulking or conjunctival mass excision.[6] One third of the patients were observed. Most of the patients [79%] had no significant recurrence or no obvious progression. In a minority of patients [21%] the disease continued to progress significantly.In their study of 24 patients,biopsy of 7 patients demonstrated a local monoclonal B-cell or plasma cell disease.Such immunoglobulin light-chain deposition was identified previously in biopsies of localized conjunctival and orbital amyloidosis.[8]Previous studies of 45 published patients with available management data showed that 29[64%] had excisional biopsy and 15[33%] had incisional biopsy.[20] One patient preferred observation. Four[9%]patients required membrane grafting and 4[9%] underwent eyelid reconstruction or ptosis repair surgery.In our study of five patients,incisional biopsy was performed on 2[40%]patients and excisional biopsy on 3 patients.[60%] One patient[20%] required amniotic membrane grafting and one patient[20%] required wedge resection and lid reconstruction.
Conclusion
Ocular amyloidosis is a rare disease which is slowly progressive and has a wide spectrum of clinical manifestations.Consequently,the clinical diagnosis is often overlooked or delayed.Amyloidosis can cause significant ocular morbidity. Conjunctival or eyelid amyloidosis commonly presents as a mass or diffuse thickening of the conjunctiva or eyelids.An excisional biopsy for a localized lesion and an incisional biopsy for a diffuse lesion should be performed.Histopathological examination of the biopsy specimen gives the definitive diagnosis. Conjunctival malignancies such as lymphoma,leukemia and metastatic carcinomas should be ruled out.A complete systemic work up for systemic amyloidosis and associated malignancies such as multiple myeloma is mandatory.Excision of localized,solitary lesions and debulking of diffuse lesions can relieve symptoms caused by mass effect of amyloid deposits. The choice of treatment should be individualized,taking into consideration the patient’s general health,extent of tissue infiltration,the degree of ocular morbidity and the presence of systemic involvement.
References
- Pepys M B: Amyloidosis, in Weatherall D J, Ledingham JCG, Warrell D A (eds): Oxford Textbook of Medicine Vol 2. Oxford, Oxford University Press, 1996, PP 1512-24.
- Sipe J D, Benson M D, Buxbaum J N, et al. Amyloid fibril protein nomenclature: 2012 recommendations from the Nomenclature Committee of the International Society of Amyloidosis. Amyloid 2012; 19:167-170.
- Picken M M. Amyloidosis-where are we now and where are we heading? Arch Pathol Lab Med. 2010; 134(4):545-51.
- Anon Nomenclature of amyloid and amyloidosis. WHO-IUIS Nomenclature Sub-Committee. Bull World Health Organ 1993; 71:105-12.
- Sipe J D, Benson M D, Buxbaum J N, et al. Amyloid fibril protein nomenclature:2010 recommendations, from the nomenclature committee of the International Society of Amyloidosis. Amyloid 2010; 17:101-4.
- Leibovitch I, Selva D, Goldberg R A, et al. Periocular and orbital amyloidosis: clinical characteristics, management and outcome. Ophthalmology 2006; 113:1657-64.
- Shields J A, Eagle R C, Shields C L, et al. Systemic amyloidosis presenting as a mass of the conjunctival semilunar fold. AMJ Ophthalmol 2000; 130:523-5.
- Dithmar S, Linke R P, Kolling G, et al. Ptosis from localized A-lambda-amyloid deposits in the levatorpalpebrae muscle. Ophthalmology 2004; 111:1043-7.
- Shield J A, Shields C L. Conjunctival amyloidosis, in Shields J A, Shields C L (eds): Atlas of Eyelid and Conjunctival Tumors. Philadelphia, Lippincott Williams and Williams 1999; pp 324-5.
- Smith M E, Zimmerman L E. Amyloidosis of the eyelid and conjunctiva. Arch Ophthlmol 1966; 75:42-51.
- Marsh W M, Streeten B W, Hoepner J A, et al. Localized conjunctival amyloidosis associated with extranodal lymphoma. Ophthalmology 1987; 94:61-4.
- Chaturvedi P, Lala M, Desai S, et al. A rare case of both eyelids swelling: isolated conjunctival amyloidosis. Indian J Ophthalmol 2000; 48:56-7.
- Knowles D M, Jakobiec F A, Rosen M, et al. Amyloidosis of the orbit and adnexae. Surv Ophthalmol 1975; 19:367-84.
- Kyle R A, Greipp P R. Amyloidosis (AL). Clinical and laboratory features in 229 cases. Mayo Clin Proc 1983; 58:665-83.
- Pepys M B. Amyloidosis. Annu Rev Med 2006; 57:223-41.
- Lamkin J C, Jakobeic F A. Amyloidosis of the eye, in Albert D M, Jakobeic F A (eds): Principles and Practice of Ophthalmology. Philadelphia, WB Saunders, 1994; pp 2956-75.
- Demirci H,ShieldsCL,Eagle RC,Shields JA.Conjunctival amyloidosis:Report of six cases and review of literature. Surv Ophthalmol 2006;51:419-33.
- O Donnell B,WuebboltG,Collin R. Amyloidosis of the conjunctiva.Aust NZ J Ophthalmol 1995;23:207-12.
- Nau J A. Shield C L, Shields J A, et al. Clinicopathologic reports, case reports, and small case series: acute myeloid leukemia manifesting initially as a conjunctival mass in a patient with acquired immunodeficiency syndrome. Arch Ophthalmol 2002; 120:1741-2.
- Lee HM,NaorJ,DeAngelisD,et al. Primary localized conjunctival amyloidosis presenting with recurrence of subconjunctival hemorrhage. Am J Ophthalmol 2000;129:245-7
Legend – Amyloid Figures
Figure 1 .Amyloidosis HPE – Congo red stain
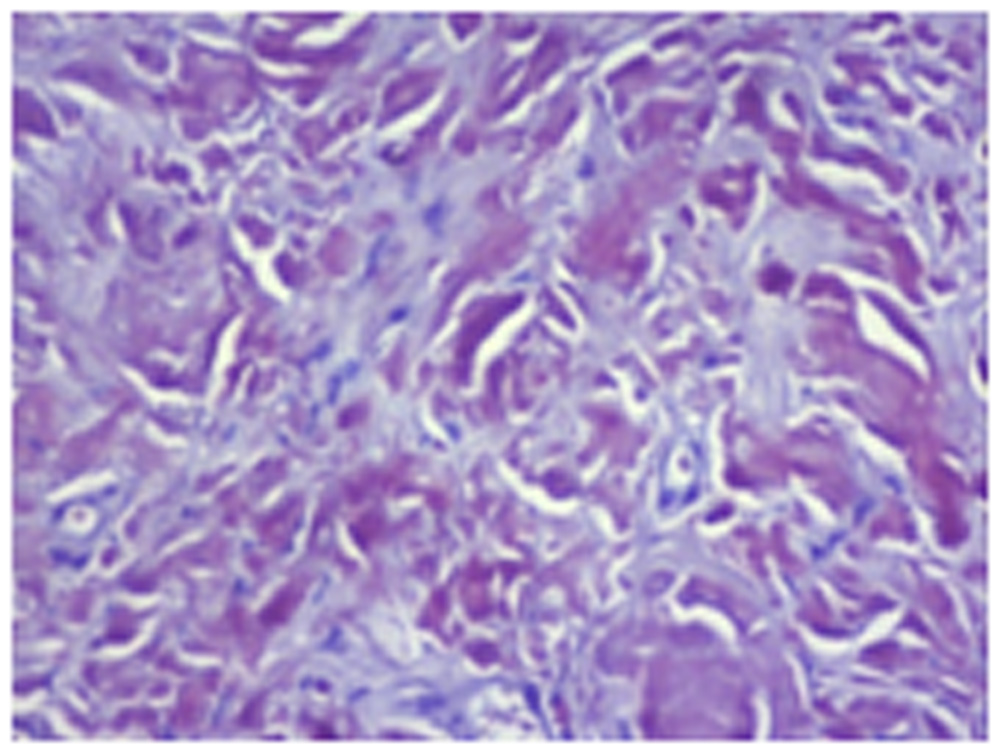
Figure 2 .Amyloidosis HPE – Congo red stain ,viewed with polarized light showing green apple birefringence
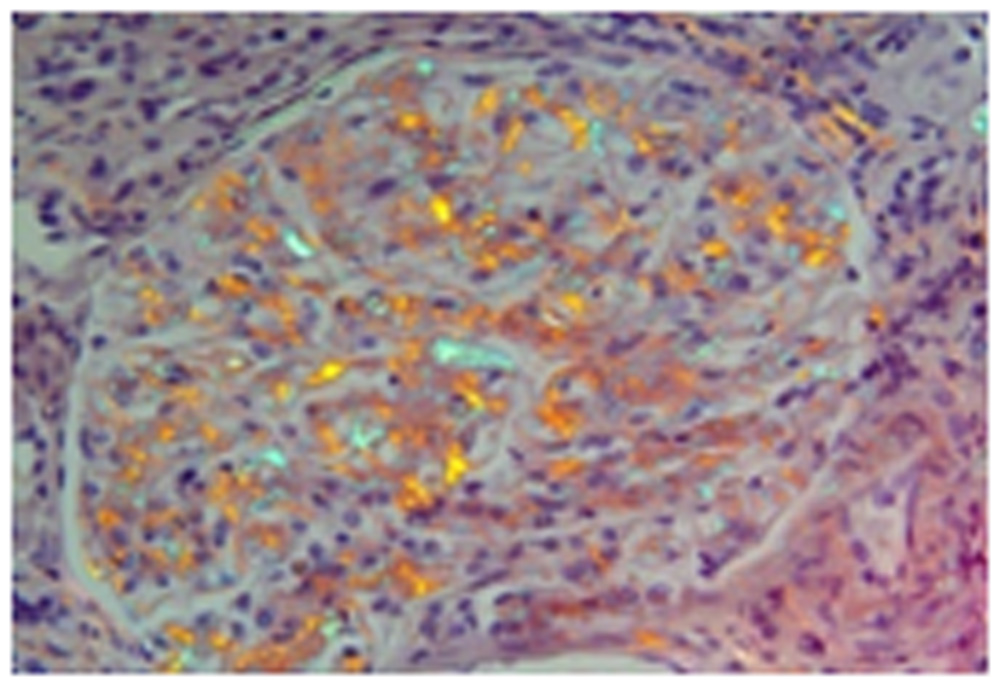
Figure 3.Amyloidosis histopathology examination[HPE]- haematoxylin and eosin stain ,showing eosinophilic staining
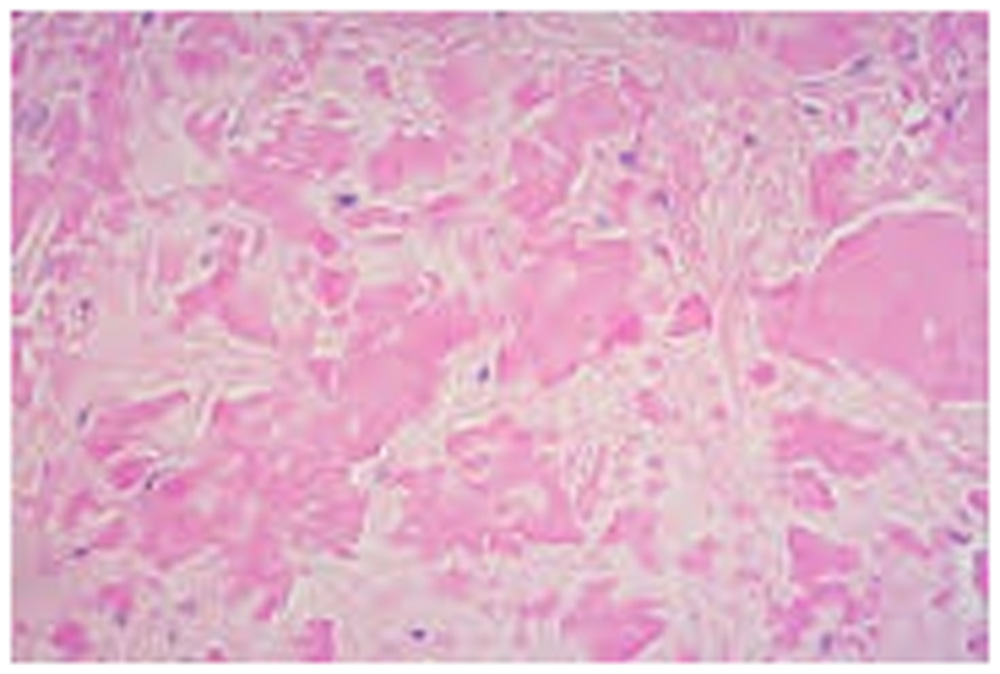
Figure 4. Amyloidosis causing ptosis of upper Lid RE
Figure 5. Bilateral conjunctival amyloidosis
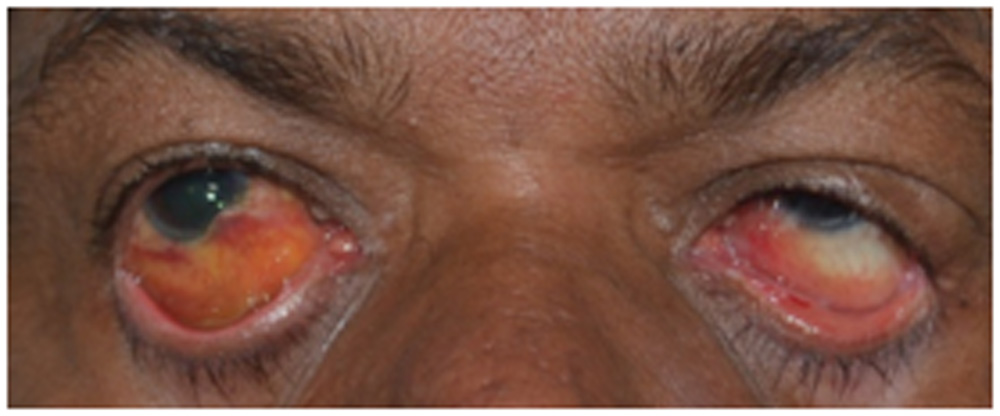
Figure 6. Amyloidosis localized – lower lid
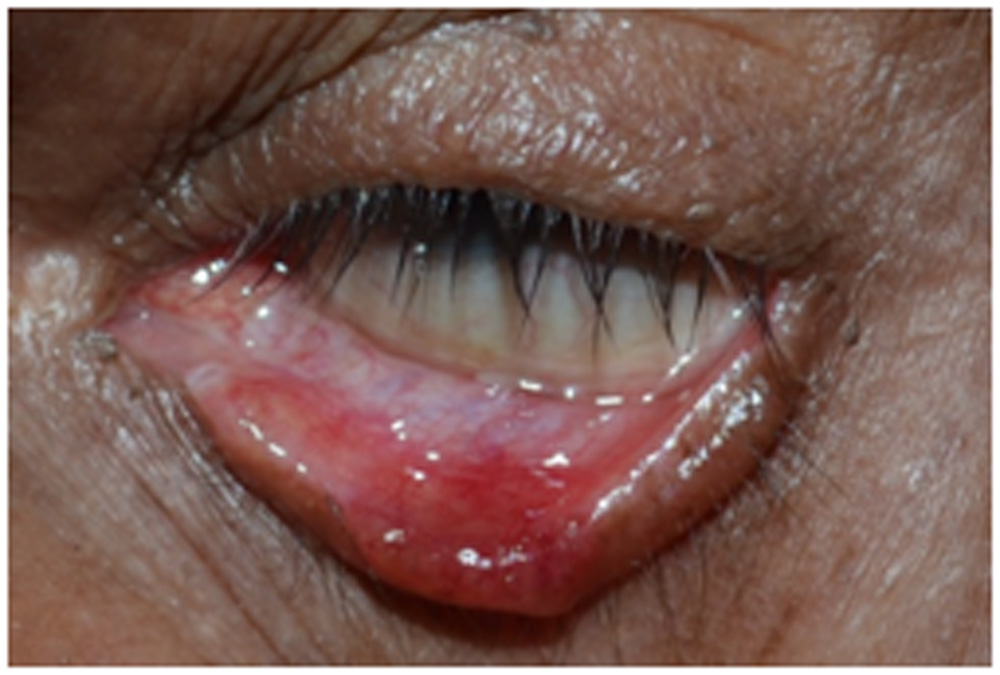
Figure 7. Amyloidosis diffuse –lower lid
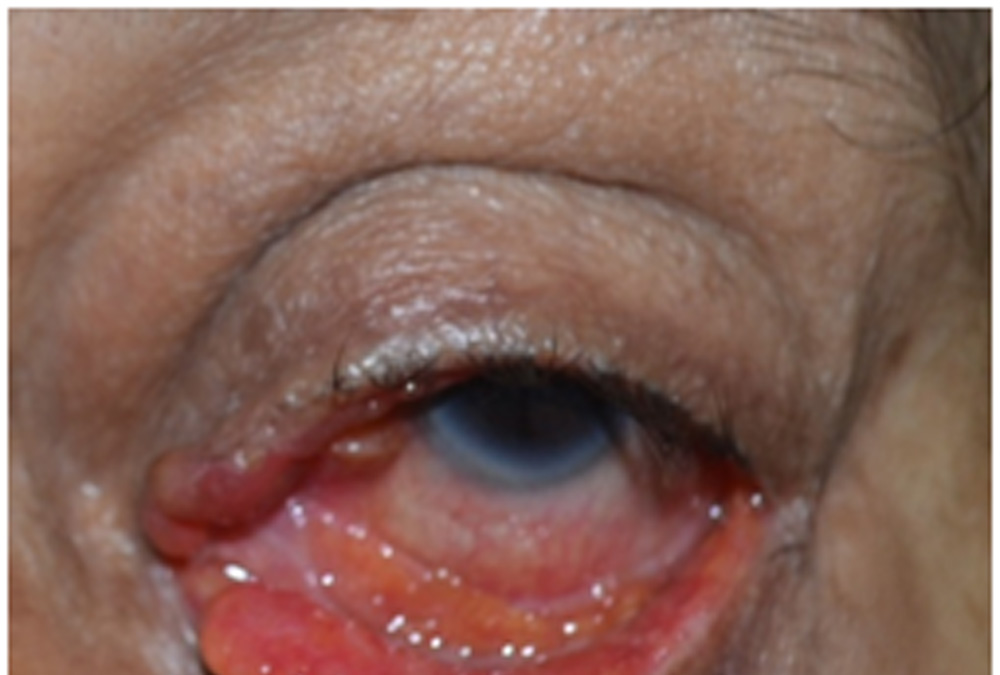
Figure 8. Amyloidosis diffuse – upper lid
Leave a Comment