
Dr. Mekhla Naik, N18166, Dr. Giridhar Anantharaman, Dr. Marian Anne Jacob
Abstract
Synopsis:Dirofilariasis is a mosquito borne zoonotic infection with progressive increase in incidence, especially in warm & moist areas such as India.We performed a retrospective analysis of 19patients with ocular dirofilariasis over past 7 years including clinical features, microbiological &/or histopathological aspects & management. Their locations included orbit (1 eye), lid (8), sub-tenons (2) & sub-conjunctival space (8). All patients with sub-conjunctival worms underwent live worm removal through a conjunctival incision after atropinisation for worm immobilization followed by oral albendazole. Rest of the patients underwent cyst excision with biopsy followed by oral antibiotics & oral steroids. In these patients, the diagnosis was confirmed on histopathology. We conclude that dirofilariasis should be considered as an important differential diagnosis in subcutaneous migratory swellings, conjunctival nodules & periocular inflammatory lesions, especially in endemic regions such as South India
Introduction and Aim of the Study
Periocular dirofilariasis is a mosquito borne end stage zoonotic infection in humans.1It is caused by a filarial parasite belonging to the genus Dirofilaria(Phylum Nematode – Roundworm).1Dogs and cats are the most common natural host of the parasite.2 Humans are accidental dead-end hosts in whom the microfilaria, the blood borne stage of the parasite, are transmitted by Aedes and Culex, the mosquito vectors.2
Human dirofilariasis has been reported rarely in parts of Africa, Latin America, Europe and Asia, including India.3 It is transmitted by blood feeding arthropods or mosquitoes.1, 3Dirofilaria species infections in humans have been mostly identified in lungs and subcutaneous tissues. The ophthalmic involvement in dirofilariasis represents 30% of extrapulmonary dirofilarial infections.4 It can occur subcutaneously in the lid causing nodules mimicking lid tumour.5 In the orbit it presents as an abscess or a mass.6 Presence of worm in subconjunctival space, anterior chamber and vitreous cavity have also been reported.7, 8 Despite the location, management is excision of the mass along with histopathological confirmation.
The aim of our study was to report our series of patients with dirofilariasis with periocular involvement.
Materials and Methods
We performed a retrospective analysis of nineteenpatients with ocular dirofilariasis over past seven years (2010-2016) at a tertiary eye care centre in South India. Retrospective chart analysis was performed to evaluate the clinical features, microbiological and / or histopathological aspects and management of the patients.
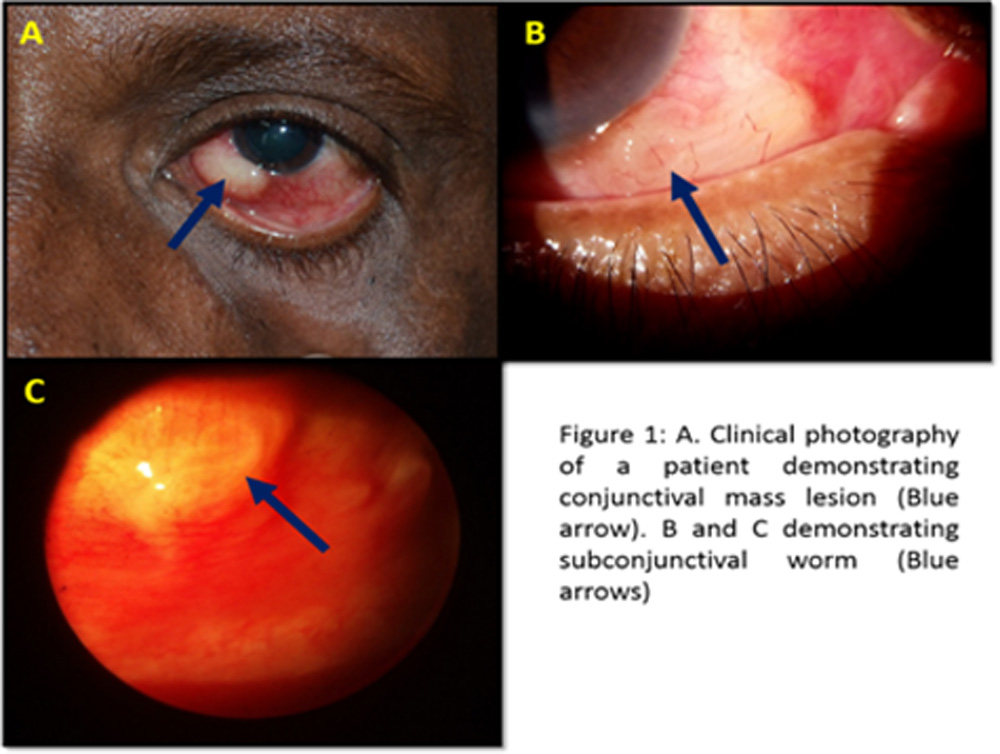
In the clinical features, analysis was performed including the presenting symptoms and signs, location of the worm (Figure 1).
All patients with a live worm, underwent worm removal through a conjunctival incision under topical anesthesia after worm immobilization with topical atropine eye drops. The remaining patients underwent cyst excision with biopsy under local or general anesthesia. Postoperatively the patients with live worm were treated with systemic albendazole whereas the patients undergoing cyst excision were given systemic antibiotics & steroids.
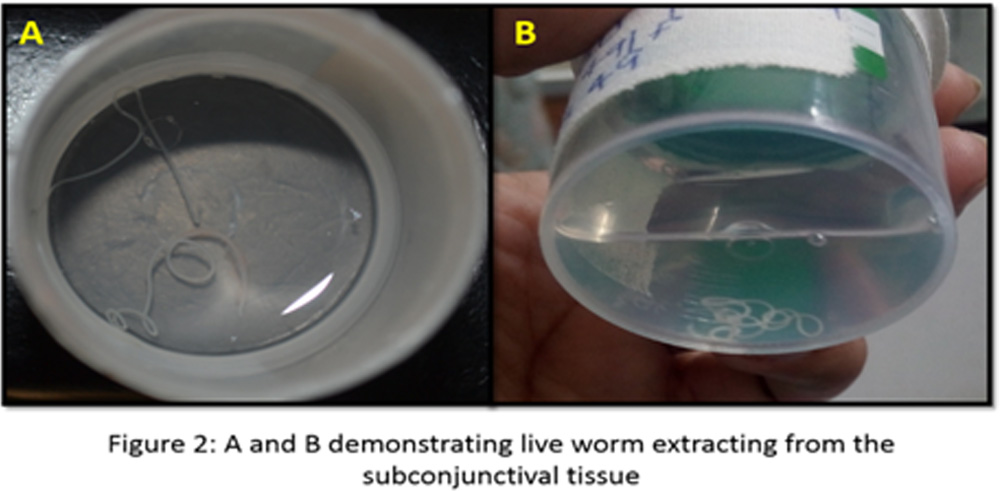
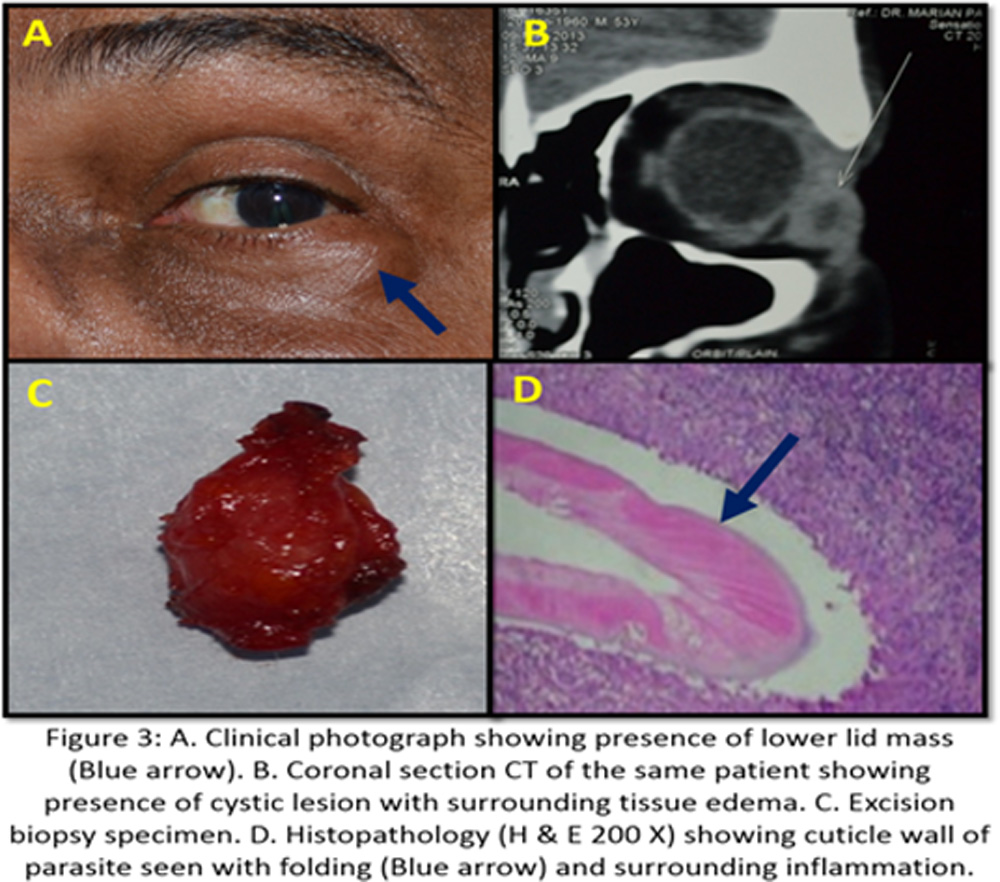
The patients in whom the live worm was retrieved, the samples were preserved in distilled water (Figure 2) and sent to the laboratory for microbiological analysis whereas patients in whom they presented with cystic lesions, the diagnosis was confirmed by histopathological analysis (Figure 3).
Results
The mean age of the patients was (range 9 months to 75 years). There were 9 males and 10 females in the study group.
Clinically, all patients presented with unilateral involvement. Our study showed 42.10 % (8 eyes) of the cases involving the sub-conjunctival space and lids each. Other sites included orbit 5.26% (1 eye) and sub-tenons space 10.53 % (2 eyes). The most common presentation was redness (52.63%) followed by lid edema (42.10%), conjunctival nodule (36.84%), ocular pain (26.32%) and foreign body sensation (26.32%). On blood investigations, none of the patients had presence of eosinophilia.
10 eyes with worm in the subconjunctival and sub-tenons space underwent worm immobilization and removal through a conjunctival incision. All 10 live worm samples were sent for microbiological evaluation which confirmed presence of Dirofilarial worm. The live worm were sent for evaluation in distilled water. For the remaining 9 eyes, who presented with cystic lesion, underwent cyst excision and biopsy under local or general anesthesia. The specimen was sentin 10% buffered formalin solution. Histopathological analysis of all these samples also confirmed the diagnosis of Dirofilariasis.
Discussion
Dirofilariae are nematodes with a long, thin, and filariform appearance.9 They are natural parasites of a wide variety of canine and feline hosts.The animal hosts are infected after being bitten by arthropods, such as Anopheles, Aedes, and Culex. Man becomes infected as an accidental host via the same route.There are over 20 documented species of Dirofilaria, of which Dirofilariaamities(or “canine heartworm”), which inhabits the heart and vascular system of their hosts, and D. repens, which has predilection for the subcutaneous tissues commonly infects the human species.9
A fixed or migratory, often painless nodule may appear anywhere in the body; however, for reasons that are not entirely clear, the parasite has a strong tendency to localize on the face, near the orbit or in the conjunctivae.10, 11 Eosinophilia and increased serum IgE levels are not commonly observed.11 Even in our series of 19 eyes, we did not observe eosinophilia in any of our cases.
Periocular dirofilariasis is rarely reported in the literature. The first case of human ocular dirofilaria was reported by Addario in 1885 from Milan, Italy.12 These worms were earlier referred to as Filaria conjunctiva and later as D.conjunctiva because of their frequent association with orbit.12 Dirofilariasis is often reported from European countries surrounding the Mediterranean region.
Four species within the genus Dirofilaria have been found to cause zoonotic disease in humans: D. immitis, D. repens, D. tenuis, and D. ursi.13 The epidemiology depends on the prevalence of canine dirofilariasis, presence of mosquito vectors and human activities leading to the exposure. In India, most of the documented cases are caused by D. repens and D. immitis, especially from the southern states and are mainly ocular infections affecting eyelid, orbit and conjunctiva.14 In these cases, it mimicked tumours in initial assessment.
Dirofilariasis has been described in adult population in European countries while it has primarily been described in children in Sri Lanka.15, 16 This may primarily be due differences in species along with variable social and geographical factors.
In the current study, around 42.10% of eyes had presence of worm in the sub-conjunctival space and lids respectively. This is consistent with worldwide literature where it has been documented to involve the region of head, especially the conjunctiva, in around 47% of the patients.17 Researchers have shown a higher rate of detection of parasites on histopathological evaluation of the specimen as compared to live worm detection.17 However, in our series of 19 eyes, 10 eyes (52.63%) had live worm detection as compared to 9 eyes (47.37%) in whom there was histopathological confirmation of diagnosis.
In literature, the diagnosis of dirofilariasis in patients presenting with cystic or nodular lesions has been based on histopathological evaluation of the excised specimen and identification of the nematode. Molecular diagnostic tests including PCR has also been utilized for identification of worm-specific DNA.18, 19 However, the sensitivity of this modality is limited due to inadequate detection of worm DNA. This occurs because of DNA fragmentation secondary to paraffin or formalin fixation of the biopsy specimen.19To overcome this limitation of PCR analysis, we performed the gold standard histopathological confirmation for all our biopsy specimens.
Excision biopsy is the treatment of choice for dirofilariasis.9, 14 Mostly cases are being diagnosed retrospectively, thus biopsy is diagnostic as well as therapeutic. Concurrent use of oral anti-helminthic therapy has been advocated by many workers.9 In our series, postoperatively, the patients with live worm were treated with systemic albendazole whereas the patients undergoing cyst excision were given systemic antibiotics & steroids.
Conclusion
Dirofilariasis should be considered as an important differential diagnosis in subcutaneous migratory swellings, conjunctival nodules & periocular inflammatory lesions, especially in endemic regions such as South India.
References:
- Sunayana Bhat, May Saldanha, Norman Mendonca. Periocular dirofilariasis: A case series. Orbit, 35:2, 100-102.
- Magi, M., Calderini, P., Gabrielli, S., Dell’Omodarme, M., Macchioni, F., Prati, M.C. & Cancrini, G. (2008) Vulpes vulpes: a possible wild reservoir for zoonotic filariae. Vector Borne and Zoonotic Diseases 8, 249–252.
- G. Hrckova, H. Kuchtova, M. Miterpa ´kova, F. Ondriska, J. Cibı ´c ˇek, S ˇ. Kovacs. Histological and molecular confirmation of the fourth human case caused by Dirofilaria repens in a new endemic region of Slovakia. Journal of Helminthology (2013) 87, 85–90.
- Tse BC, Siatkowski R, Tse DT. A technique for capturing migratory periocular worms: A case series and review of literature. OphthalPlastReconstrSurg 2010;26:323–326.
- Mahesh G, Giridhar A, Biswas J, et al. A case of periocular dirofilariasis masquerading as a lid tumour. Ind J Ophthalmol 2005;53(1):63–64.
- Angunawela RI, Ataullah S, Whitehead KJ, et al. Dirofilarial infection of the orbit. Orbit 2003;22(1):41–46.
- Gorezis S, Psilla M. Intravitreal dirofilariasis: a rare ocular infection. Orbit 2006;25(1):579.
- Sangit VA, and Haldipurkar SS. Subconjunctival dirofilariasis mimicking scleritis: First report from Western India. Ind J Ophthalmol 2012;60(1):76–77.
- Siepmann K, Wannke B, Neumann D, Rohrbach JM. Subcutaneous tumor of the lower eyelid: a potential manifestation of a Dirofilariarepens infection. Eur J Ophthalmol. 2005 Jan-Feb;15(1):129-31.
- Rouhette H, Marty P, Zur C, et al. Ocular filariasis: not strictly tropical. Ophthalmologica 1999; 213: 206-8.
- Arvanitis PG, Vakalis NC, Damanakis AG, et al. Ophthalmic dirofilariasis. Am J Ophthalmol 1997; 123: 689-91.
- Addario C. Su un nematode dell’occhio umano. Ann Ottalmol 1885;13:135–137.
- Kersten RC, Locastro AJ, Eberhard ML, et al. Periorbital dirofilariasis. OphthalPlastReconstrSurg 1994;10:293–6.
- Marian Pauly, Jyotirmay Biswas, Rameez N. Hussain, GiridharAnantharaman. Periocular Dirofilariasis Mimicking Lacrimal Sac Mucocoele. Orbit. 2013 Oct;32(5):324-6.
- Marty, P. Human dirofilariasis due to Dirofilaria repens in France: A review of reported cases. Parassitologia1997: 39, 383–386.
- Dissanaike,A.S.,Abeyewickreme,W.,deS.Wijesundera, M., Weerasooriya, M.V. & Ismail, M.M. Human dirofilariasis caused by Dirofilaria (Nochtiella) repens in Sri Lanka. Parassitologia 1997: 39, 375–382.
- Pampiglione, S., Canestri-Trotti, G. & Rivasi, F. Human dirofilariasis due to Dirofilaria (Nochtiella) repens: a review of world literature. Parassitologia 1995: 37, 149–193.
- Ondriska, F., Lengyel, D., Miterpa ´kova ´, M., Lengyelova ´, B., Streha ´rova ´, A. & Dubinsky ´, P. Human dirofilariosis in the Slovak Republic – a case report. Annals of Agricultural and Environmental Medicine2010: 17, 169–171.
- Favia, G., Lanfrancotti, A., Della Torre, A., Cancrini, G. & Coluzzi, M. Polymerase chain reactionidentification of Dirofilaria repens and Dirofilaria immitis. Parasitology 1996:113, 567–571.
Leave a Comment