
Dr. Vivek Chaitanya, C18870, Dr.Neeraj Shah, Dr.K S Siddharthan, Dr.Ingawale Ameya Rajas Deepak, Dr.Jagadeesh Kumar Reddy K
Purpose: The purpose of this study is to compare the effects of a single Subconjunctival Triamcinolone acetonide (SCTA) injection to tapering topical Loteprednol in patients undergoing phacoemulsification surgery under topical anesthesia.
Design: Randomized Prospective Interventional Study.
Methods:A total of400 patients were randomised into 2 groups; Group A (200 patients) received 5 mg SCTA at the end of surgery and topical Ketorolac Tromethamine (0.5%) with Ofloxacin (0.3%) for 3 weeks. Group B (200 patients) received tapering topical Loteprednol Etabonate (0.5%) along with Ofloxacin (0.3%) and Ketorolac Tromethamine (0.5%) for 3 weeks. Outcomes evaluated were Intraocular pressure (IOP), anterior chamber cells/flare and macular oedema post-operatively at 1, 6 and 12 weeks.
Results: Baseline parameters were almost similar in both the groups.NoStatistical difference was seen between the pre-op and post-op IOP values for Group A (P=0.82) and Group B (P=0.61) and post-op IOP values in between both groups (P=0.14) at 1 week. Incidence of cells/flare post-op was statistically not significant (P=0.82) in both groups at all follow up visits. Post-op macular oedema was not observed at any follow up visit.
Conclusion: SCTA appears to be an effective alternative to prolonged post-operative topical steroid use.
Key-words:Intraocular pressure, Subconjunctival Triamcinolone Acetonide, Phacoemulsification, Loteprednol, cells/flare.
Key messages:Single subconjunctival steroid injection post cataract surgery could be the long term solution instead of topical drops, reducing cost and the need for patient compliance.
Introduction:
Cataract surgery is one of the most common and most successful surgical interventions today. Yet, from intra and post-operative complications to patient compliance; it is not without issues. Like other types of surgeries, cataract surgery also induces an inflammatory response, commonly anterior segment inflammation and macular oedema.
Post-operative regimens to minimise inflammation vary widely among clinicians. Studies1,2 have evaluated the efficacy of alternative administrative routes of corticosteroids apart from topical to deliver higher and more stable intraocular concentrations and improve patient compliance. Injection of depot corticosteroids into sub-Tenon’s capsule is an established approach of treating various ocular inflammatory diseases.3,4 Post-operative topical drops such as NSAIDs (e.g. Ketorolac and Nepafenac)5,6 and steroids (e.g. Dexamethasone and Prednisolone)7 have been the mainstay for prophylaxis and treatment of inflammation. Unfortunately, adherence to topical medication regimens is less than ideal.8
The current study is designed to evaluate the effects of a single Subconjunctival Triamcinolone Acetonide injection (SCTA) to that of topical Loteprednol on IOP, anterior chamber inflammation and macular oedema post cataract surgery.
Methods:
This study was conducted at a tertiary eye care centre in Southern India. Institution Ethics committee approval was obtained before commencement of the study and informed consent taken from each participant. The study was performed in accordance with the tenets of the Declaration of Helsinki. It was designed as a Randomised Prospective Interventional Study and comprised of patients who underwent phacoemulsification surgery for cataract over duration of 6 months from July 1st 2016 to Dec 31st 2016.A consort flow diagram for recruitment and analysis of patients in this study is shown below [Fig. 1]. Patients were randomised 1:1 on the basis of simple coin flipping technique. Group A patients were to receive 5 mg SCTA at the end of surgery with topical ketorolac Tromethamine (0.5%) and Ofloxacin (0.3%) 4 times per day for 7 days followed by 2 times per day for 2 weeks. Group B patients were administered tapering topical Loteprednol (0.5%) 6-4-3-2-1 times per day for 7 days each with Ofloxacin (0.3%) and ketorolac Tromethamine (0.5%) 4 times per day for 1 week followed by 2 times per day for 2 weeks.Patients were followed up at 1 week (visit 1), 6 weeks (visit 2), and 12 weeks (visit 3) for evaluation of IOP, anterior chamber cells/flare and macular oedema and other adverse events if any.
Inclusion/Exclusion Criteria:
Patients eligible for inclusion were all those who had a cataractous lens according to Lens Opacities Grading System III (LOCS III).9 Patients excluded were those who had cataract with grade 5, 6 nuclear colour/opalescence, a prior history of uveitis or evident intraocular inflammation, suffering from glaucoma, high myopes (axial length>25 mm), known steroid responders, previous ocular surgeries, corneal diseases. Also excluded were patients with diabetes, hypertension and asthma or on any systemic anti-inflammatory therapy. In addition, those who developed any intra-operative complications such as posterior capsule rupture, zonular dialysis or those who could not complete the required follow up visits were also to be excluded.
Baseline Evaluation:
Patients were advised not to take any systemic anti-inflammatory drugs during the study period. Pre-operative parameters measured were IOP in mm Hg by Non-contact Tonometry (NCT) (Topcon CT-80, Topcon Corp, Japan). Slit lamp Biomicroscopy examination (Topcon SL 1E, Topcon Corp, Japan) was used to rule out the presence of cells/flare in the anterior chamber and macular edema. Best corrected visual acuity (BCVA) using Snellen visual acuity was noted for every patient.
Study medication
A vial of Triamcinolone Acetonide injection (Tricort 10, Cadila Pharmaceuticals) of 1 mL containing 10 mg/mL was used. A 1 cc syringe with 26 Gauge needle was utilised to withdraw 0.5 mL (5 mg) which was subsequently injected subconjunctivally at the end of surgery.
Surgical Technique:
Routine phacoemulsification under topical anaesthesia and implantation of a foldable hydrophobic acrylic monofocal 1 piece posterior chamber intraocular lens (Technis 1, Santa Ana, California, AMO Inc.) was performed by a single surgeon. After the conclusion of surgery, 5 mg SCTA was injected under the superior or inferior bulbar conjunctiva in patients of Group A [Fig. 2].
Outcome measures:
Follow up visits were advised at 1, 6, 12 weeks and BCVA was recorded. Primary outcomes evaluated were IOP, anterior chamber inflammation and cystoid macular oedema. IOP was measured with the help of NCT with the mean of two measurements used for analysis; patients with IOP>21 mm Hg were started on anti-glaucoma medication (Dorzolamide eye drops 2%, 2 times/day for 30 days) and managedaccordingly. Anterior chamber cells/flare were evaluated on slit lamp andgraded according to Standardization of Uveitis Nomenclature Working Group criteria (SUN).10Macular oedema was assessed clinically and using Spectralis Optical Coherence Tomography (Cirrus HD OCT 4000).
Secondary outcomes evaluated were the size of SCTA depot in millimetres (mm) at every visit and also local adverse effects like subconjunctival haemorrhage (SCH), chemosis, congestion or necrosis, if any.
Statistical analysis:
Data was analysed using commercial software (SPSS version 14.0 Inc., Chicago, Illinois, USA). Paired-t test (within group) and unpaired-t test (between groups) were used to compare the IOP values. Pearson chi-square test was used to analyse patient demographics and the presence of anterior chamber cells/flare and development of macular oedema. P value less than 0.05 was considered statistically significant (95% confidence interval) for all variables. Secondary outcomes except size of SCTA depot were analysed qualitatively.
Results:
This study enrolled 400 patients. Each treatment group comprised of 200 patients. There was no loss to follow up for any patient in either group. The demographics of the study population have been presented in Table 1.
Fig. 3 depicts the mean IOP and their standard deviations (SD)at baseline, post-op 1, 6, 12 weeks in Group A receiving SCTA and Group B receiving topical Loteprednol. The mean IOPvalues at each post-op visit were not statistically significant between Group A and Group B (P=0.14) at visit 1, (P=0.06) at visit 2 and (P=0.12) at visit 3. 9 patients in group A had an IOP>21mm Hg on visit 1, which reduced to 3 patients on visit 2 and to 2 patients on visit 3. There was also no statistical difference in the mean pre-op and post-op IOP values within group A (P=0.82) and within group B (P=0.61) at visit 1. Similar findings were noted at visit 2 where the difference in IOP values were not significant for both Group A (P=0.57) and Group B (P=0.33) compared to baseline values. Visit 3 also revealed similar results for Group A (P=0.65) and Group B (P=0.39). 2 patients who had consistent IOP values of greater than 25 mm Hg at all visits underwent excision of SCTA after 12 weeks follow up.
5% patients among Group A developed anterior chamber cells/flare by visit 1 compared to 6% among Group B. The incidence of cells/flare reduced to 1% and 1.5% of total patients in Groups A and B respectively by visit 2. There was complete resolution of cells/flare in both groups by visit 3 as seen in the data given in Table 2. The difference in anterior chamber cells/flare scores between both the groups were not statistically significant at both visit 1 and visit 2 (P=0.82).
Among both the groups receiving treatment, there was no evidence of post-operative macular oedema on slit lamp examination which was then confirmed on OCT. There weren’t any other abnormal clinically significant ophthalmic findings.
Mean size of the SCTA depot at the time of injection was 6.5 mm. On follow up the mean sizes were 3.5 mm at visit 1, 2.25 mm at visit 2 and 1.15 mm at visit 3. Minimal SCH was noted in 5 patients on visit 1 which completely resolved by visit 2. No other local adverse effects like chemosis, congestion, necrosis or ulceration were seen in any of the follow up visit.
Discussion:
With improvement in cataract surgical techniques, the incidence of post-operative inflammation has declined but still persists. To counter it, various modalities are being tested one of which is the subconjunctival injection of steroids immediately after cataract surgery. With increasing incidence of cataracts in recent times, lack of compliance to post-op topical medications from patients, increasing cost, and patient inconvenience etc, a single subconjunctival injection of steroid could be a viable alternative to post-operative topical steroid use. Our study shows that a single injection of SCTA at the end of an uneventful cataract surgery is equally effective if not more to prolonged topical steroid use.
Weijtens et al.11 suggested that periocular injections of corticosteroids induce a higher concentration of the steroidal agent than topical administration. Of particular concern, is the increase in IOP after administration of systemic corticosteroids.12 But changes in IOP, our main outcome measure were not significant in the group receiving SCTA in comparison to the baseline values. 9 patients had an IOP>21 mm Hg on visit 1 (among those 4 had an IOP>30 mm Hg). Follow up visits showed improvement in IOP values and by visit 3, IOP values of almost all patients returned to their baseline levels, except only 2 patients among Group A who had an IOP>25 mm Hg. Surgical excision of depot injection has been suggested and may be required in patients who have received sub-Tenon’s capsule injections of corticosteroids and are not responding to maximal anti-glaucoma therapy.13 Considering the above, those 2 patients underwent excision of SCTA under topical anaesthesia , the indication being uncontrolled IOP. Post excision, the IOP in these patients promptly reduced to the normal range without requiring any further topical anti-glaucoma therapy.
Coming to anterior chamber cells/flare, which were graded on the basis of SUN for reporting clinical data; the results showed almost equal distribution with no statistical difference in patients having cells/flare post-operatively in between both Group A and B during visit 1 and visit 2 (P=0.82). Complete resolution of cells/flare was noted by visit 3. Study conducted by Shah et al.14 showed similar course in resolution of cells/flare to almost nil by 12 weeks. Laser flare meter has been used for the objective assessment of anterior chamber inflammatory activity.15 Studies conducted by Tan et al.16 and Negi et al.17 using the above mentioned methodshowed similar results. The post-operative cells/flare counts in our study were clinically insignificantand thus did not warrant any extra treatment in both groups.
Macular oedema, a common complication of cataract surgery is best detected using OCT and in particular using the center point thickness parameter.18,19 Since OCT can achieve a high-resolution measurement of retinal thickness of up to 10 mm, it may be able to detect subtle changes in retinal thickness which is not clinically evident.20 Macular oedema mostly peaks at around 4 to 6 weeks after cataract surgery and can also develop several months post-operatively.21Macular oedema has been defined as a relative increaseddiffuse thickening, presenting with or without cystoid abnormalities and with or without visual loss. Among both groups, No patient developed post-operative macular oedema at any follow up visit.
Size of SCTA depot at the time of injection was around 6-7 mm. By visit 3 the depot had completely disappeared in greater than 95% patients and the rest had a depot of less than 2mm. Location and size of the depot was cosmetically acceptable. Conjunctival ischemia and necrosis following periocular/intraocular injection of triamcinolone acetonide had been reported in adult patients.22,23In our study, minimal SCH was noted in 5 patients at visit 1 which completely resolved by visit 2. Apart from SCH, no other local adverse effects like chemosis, congestion or necrosis/ulceration were noted at any follow up visits. Limitations of our study include lack of laser flare meter measurements for assessment of flare post-operatively, need for longer follow up especially for analysing macular edema. Wider group of patients not assessed in this study e.g. patients falling in our exclusion criteria; for us to confidently advocate safety and efficacy in various scenarios. An evaluation of subjective patient satisfaction or comfort score to assess the patient’s perspective regarding the therapeutic modalities could have added value to this study. Advantage of this study included large sample size with a proper follow up of each and every patient.
Conclusion:
In our opinion, a single subconjunctival injection of Triamcinolone acetonide at the end of a routine uneventful phacoemulsification surgery can be a useful alternative to prolonged tapering topical steroid use in preventing intraocular inflammation and macular oedema. Since the number, frequency and duration of instilling eye drops is significantly reduced in the SCTA group it definitely contributes to faster rehabilitation coupled with greater patient comfort. Further studies are needed for detailed analysis and to cover a broader spectrum of patients.
References:
- Watson D, Noble MJ, Dutton GN, Midgley JM, Healey TM. Penetration of topically applied dexamethasone alcohol into human aqueous humor. Arch Ophthalmol 1988; 106:686–687.
- Chang DF, Wong V. Two clinical trials of an intraocular steroiddelivery system for cataract surgery. Trans Am OphthalmolSoc 1999; 97:261–276. discussion 276–279.
- HelmCJ, HollandGN. The effects of posterior subtenon injection of triamcinolone acetonide in patients with intermediate uveitis. Am J Ophthalmol. 1995;120:55–64.
- ZamirE, ReadRW, SmithRE, et al. A prospective evaluation of subconjunctival injection of triamcinolone acetonide for resistant anterior scleritis. Ophthalmology. 2002;109:798–805.
- Flach AJ, Jaffe NS, Akers WA. The effect of ketorolac tromethaminein reducing postoperative inflammation: double-mask parallel comparison with dexamethasone. Ann Ophthalmol 1989; 21:407–411.
- Cervantes-Coste G, S_anchez-Castro YG, Orozco-Carroll M,Mendoza-Schuster E, Velasco-Barona C. Inhibition of surgically induced miosis and prevention of postoperative macular edema with nepafenac. Clin Ophthalmol 2009; 3:219–226.
- Diestelhorst M, Aspacher F, Konen W, Krieglstein GK, Hilgers RD. Effect of dexamethasone 0.1% and prednisolone acetate 1.0% eye drops on the blood-aqueous barrier after cataract surgery: a controlled randomized fluorophotometric study. Graefes Arch Clin Exp Ophthalmol 1992; 230:451–453
- Tsai JC. A comprehensive perspective on patient adherence totopical glaucoma therapy. Ophthalmology 2009; 116(11 suppl):S30–S36
- Hall N, Lempert P, Shier R, Zakir R, Phillips D. Grading nuclear cataract: reproducibility and validity of a new method. The British Journal of Ophthalmology. 1999;83(10):1159-1163.
- Jabs DA, Nussenblatt RB & Rosenbaum JT (2005): Standardization of uveitis nomenclature for reporting clinical data. Reports of the First International Workshop. Am J Ophthalmol 140: 509–516.
- Weijtens O, Schoemaker RC, Romijn FP et al. (2002): Intraocular penetration and systemic absorption after topical application of dexamethasone disodium phosphate. Ophthalmology 109: 1887–1891.
- Increased intraocular pressure induced by repository corticosteroids. Am J Ophthalmol. 1976;82:90–93.
- AkdumanL, KolkerAE, BlackDL, et al. Treatment of persistent glaucoma secondary to periocular corticosteroids. Am J Ophthalmol. 1996;122:275–277.
- Shah SM &Spalton DJ (1994): Changes in anterior chamber flare and cells following cataract surgery. Br J Ophthalmol 78:91–94.
- El-Maghraby A, Marzouki A, Matheen TM, Souchek J, Van der Karr M. Reproducibility and validity of laser flare/cell meter measurements as an objective method of assessing intraocular inflammation. Arch Ophthalmol 1992; 110:960–962.
- Tan DTH, Chee S-P, Lim L, Lim ASM. Randomized clinical trial of a new dexamethasone delivery system (Surodex) for the treatment of post-cataract surgery inflammation. Ophthalmology 1999; 106:223–231
- Negi AK, Browning AC, Vernon SA. Single perioperative triamcinolone injection versus standard postoperative steroid drops after uneventful phacoemulsification surgery; randomized controlled trial. J Cataract Refract Surg 2006; 32:468–474
- Kim SJ, Belair M-L, Bressler NM, Dunn JP, Thorne JE, Kedhar SR, Jabs DA. A method of reporting macular edema after cataract surgery using optical coherence tomography. Retina 2008; 28:870–876
- Kim SJ, Equi R, Bressler NM. Analysis of macular edema after cataract surgery in patients with diabetes using optical coherence tomography. Ophthalmology 2007; 114:881–889
- Hee MR, Puliafito CA, Wong C, Duker JS, Reichel E, Rutledge B et al. Quantitative assessment of macular edema with optical coherence tomography. Arch Ophthalmol 1995; 113: 1019–1029
- Rotsos TG, Moschos MM. Cystoid macular edema. Clin Ophthalmol 2008; 2:919–930.
- Rubinstein A, Hanson RJ, Chen SD, Porter N, Downes SM. Conjunctival ischaemia subsequent to posterior subtenon’s triamcinolone acetonide injection. Eye (Lond) 2006;20:388–9.
- Agrawal S, Agrawal J, Agrawal TP. Conjunctival ulceration following triamcinolone injection. Am J Ophthalmol. 2003;136:539–40.
Tables:
| Table 1. Patient characteristics | |||
| Group A (200) | Group B (200) | ||
| P value | |||
| Mean Age (range) | 65 years (55-78) | 67 years (59-80) | |
| Male Patients | 102 | 105 | 0.76 |
| Female Patients | 98 | 95 | |
| Right Eyes | 98 | 101 | 0.76 |
| Left Eyes | 102 | 99 | |
| Table 2.Number of Patients having anterior chamber cells/flare | |||||||
| Visit 1 (1 week) | Visit 2 (6 weeks) | Visit 3 (12 weeks) | |||||
| SUN Grading-> | 1+ | 2+ | 1+ | 2+ | 1+ | 2+ | |
| Group A | 6 | 4 | 1 | 1 | – | – | |
| Group B | 8 | 4 | 2 | 1 | – | – | |
*SUN: Standardization of Uveitis Nomenclature
Figures:
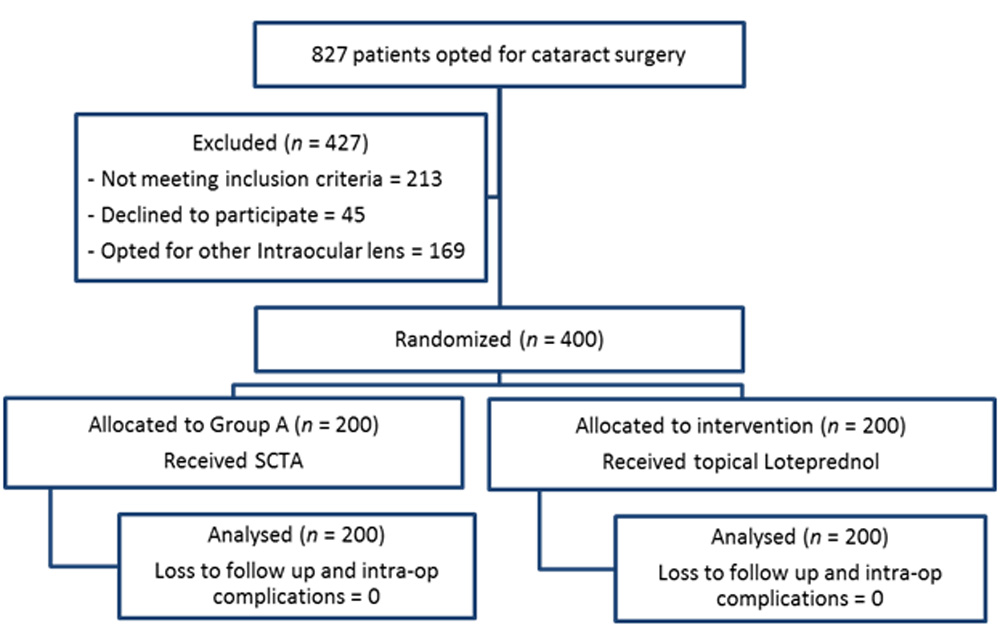
Figure 1: Study profile of patient flow

Figure 2: A peri-operative subconjunctival injection of Triamcinolone Acetonide
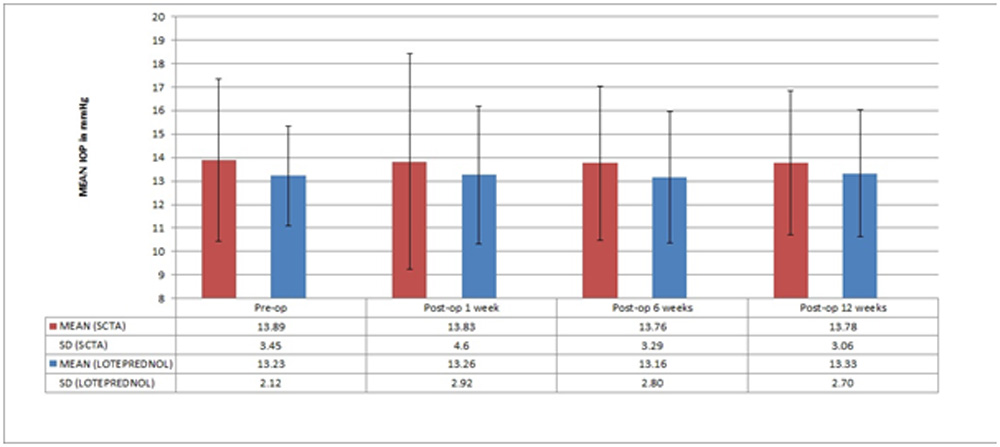
Figure 3: Comparison of IOP values between patients who received peri-operative SCTA (Group A) and patients receiving post-operative topical Loteprednol (Group B)
Leave a Comment