
Dr. Sameera.V.V, S19235, Dr. Guruprasad Ayachit, Dr. Shrinivas M Joshi, Dr. Apoorva A G
Purpose
To assess the clinical efficacy of 577-nm micropulse laser therapy (MPLT) for the treatment of chronic central serous retinopathy (CSR)
Methods
19 eyes of 17 patients with chronic CSR (>4 month duration) subjected to ophthalmic examination, fundus fluorescein angiography(FFA),fundus autofluorescence (FAF) & Spectral domain optical coherence tomography(SD-OCT). All eyes subjected to MPLT (IQ 577 laser)& followed up at 4 weeks, 2& 3 months. Areas of focal &diffuse leaks were treated with multiple laser spots(Grid 5×5,duty cycle 5%) with no spot spacing. Primary outcome studied change in subretinal fluid (SRF)height& central macular thickness(CMT).Secondary outcome measured change in best-corrected visual acuity(BCVA)
Results
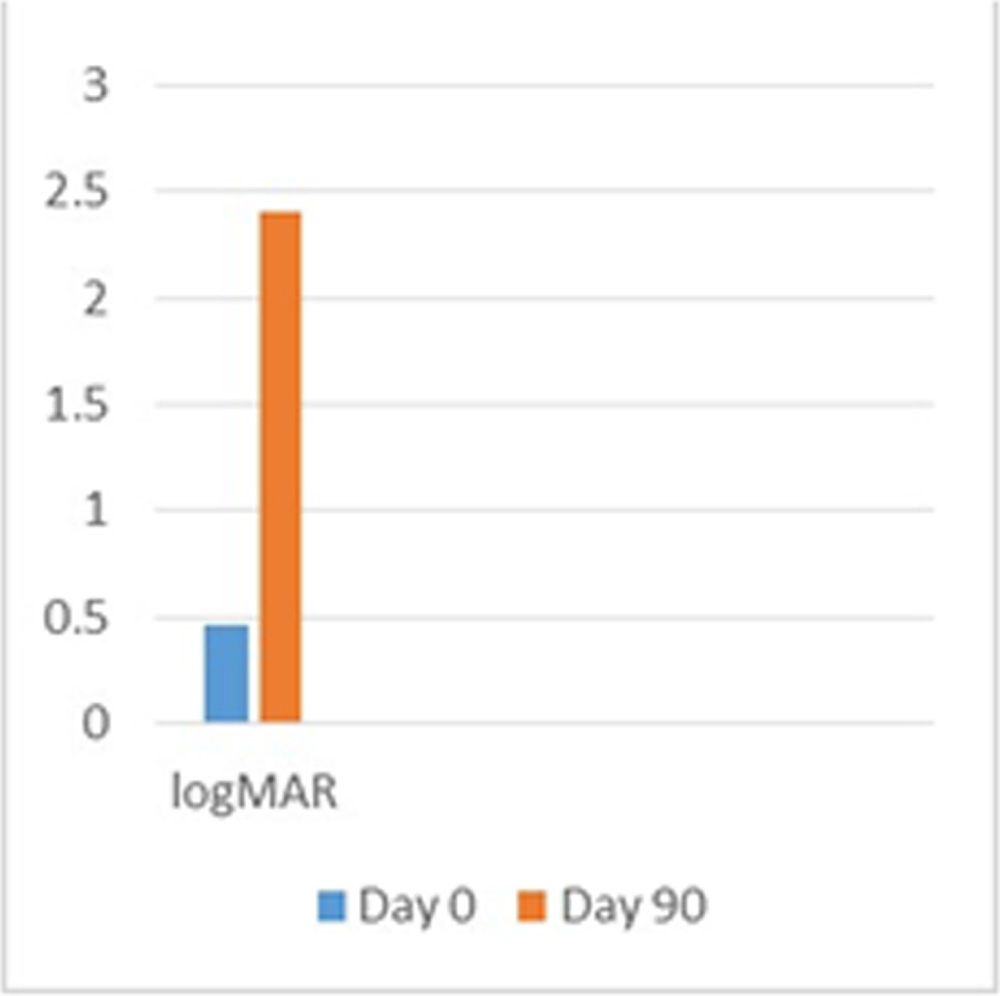
The average age of the patients was 40.3 years and the mean duration of leak 7 months. 15 patients were males & 2 females. 3 patients were on Rifampicin for 12 weeks but never responded .All 19 eyes responded to the treatment. The mean pretreatment SRF height was 340.25μm & post treatment showed a mean reduction to 102.75μm ( Day 30) & 38.25μm (3 months) respectively(P =0.0002) .The mean CMT too improved from 428 μm to 268 μm in 3 months (p=0.006)There was no evidence of retinal or retinal pigment epithelium damage on SD-OCT or FAF . No visible laser marks could be detected by clinical observation,SD-OCT& FAF. The mean BCVA improved 3 months after laser treatment from 0.46 (in logMAR) to 0.26 (P=0.009)
Conclusion
Subthreshold MPLT is a cost effective and safe treatment option in chronic CSR
Introduction
Central serous chorioretinopathy (CSC) is a disease that causes vision loss characterized by serous detachment of the neurosensory retina.1Clinical evidence from multimodal imaging, such as choroidal congestion and thickening and hyperpermeability of the choroid, suggests that choroidal dysfunction is an important underlying cause for retinal pigment epithelium (RPE) dysfunction and subretinal fluid (SRF) leakage in CSC .2 Two main subtypes of CSC can be distinguished: acute and chronic CSC (cCSC). In acute CSC, the detachment is caused by a focal leak (‘hot spot’) in the RPE. The SRF usually resolves spontaneously within few weeks and visual acuity (VA) recovers to (near-) normal in acute CSC .3Considerable visual impairment occurs if the fluid persists for more than 3 months as in cCSC which can lead to permanent structural damage and often pronounced loss of central vision.4 These patients show irregular mildly atrophic RPE changes and choroidal abnormalities which often occur without a single focal ‘hot spot’ but with more diffuse leakage .Stress and corticosteroid intake are well-known precipitating factors.
So far, there is no ‘gold standard’ treatment for CSC. Treatment options include conventional focal laser, photodynamic therapy (PDT), and intravitreal drugs like bevacizumab.5,6,7 These treatments have had variable outcomes, but not without associated risks and adverse effects. The conventional focal photocoagulation can cause central or paracentral scotomas, contrast sensitivity loss, accidental foveal damage, retinal distortion, or choroidal neovascularization. 8 A subfoveal or juxtafoveal leak precludes treatment as well. Although focal laser can potentially seal the leak seen on fluorescein angiography (FFA) and resolve the subretinal fluid, it does not alter the choroidal hyperpermeability and leakage, thus the risk of recurrence remains.9
Newer photocoagulation modalities for retinal diseases include subthreshold micropulse diode and yellow lasers. They offer the advantage of precise control and spatial confinement of laser lesions to the RPE layer. In micropulse laser therapy (MPLT), the laser energy is delivered in short pulses.The whole pulse duration is called a pulse envelope, which is divided into 100 micropulses, and each micropulse has “on” time and “off” time with a ratio depending on the duty cycle (the ratio between the on time and the whole micropulse on and off time). For example, for a 200 ms envelope which is divided into 100 micropulses, the micropulse duration on time will be 0.1–0.3 ms for a 5% and 15% duty cycle, respectively. This will produce an invisible reaction which is detectable only with microscopy and histology (subthreshold), which will be sufficient to produce an RPE-confined photothermal effect with sparing of the neurosensory retina.10 The inner retina will remain transparent and not involved as the temperature rise will be below the threshold for coagulation, in contrast to the conventional continuous-wave laser which leads to coagulation of the inner retina; thus, subthreshold micropulse laser can permit confluent therapeutic applications to the entire area of CSC.
Yellow laser (577 nm) is poorly absorbed by xanthophyll pigment, so it could be used for treatment over the fovea. Being absorbed by both melanin and oxyhemoglobin, 577 nm laser causes less scatter during treatment and allows use of less power and shorter pulse durations. It induces a biological response that promotes the recovery and restoration of the outer blood–retinal barrier and ultimately, the resorption of the subretinal fluid .11Hence, MPLT unlike conventional laser does not heal with coagulation and scarring, but by stimulation and repair.
The purpose of this study was to report the efficacy and safety of micropulse 577 nm yellow laser in the treatment of chronic CSC cases.
Methods:
This isa prospective study conducted at at M M Joshi Eye Institute, Hubli, India between May 2016 and March 2017. The study was approved by the local Ethics Committee. All study participants gave written informed consent before enrolment. The study enrolled 19 eyes of 17 patients. The inclusion criteria included any age, any sex, and history of non- resolving CSC lasting for more than 3 months confirmed by fundus fluorescein angiography and optical coherence tomography (OCT).Exclusion criteria included use of exogenous corticosteroids, diabetic retinopathy, uveitis, any hereditary retinal or macular disease. Primary outcome studied change in subretinal fluid (SRF) height & central macular thickness (CMT).Secondary outcome measured change in best-corrected visual acuity (BCVA).
The medical history of the patients were noted and clinical data such as visual acuity, ophthalmoscopic findings, SD-OCT, fundus autofluorescence (FAF) imaging, fluorescein angiography (FA), and enhanced depth imaging (EDI) findings were recorded. SD-OCT, FA were performed using the Spectralis HRA-OCT system (Heidelberg Engineering, Heidelberg, Germany). Snellen visual acuity was converted to logarithm of the minimum angle of resolution (logMAR) units for statistical analysis. 3 patients were on Rifampicin for 12 weeks but never responded to the course.
The characteristics of the patients are expressed as mean ± standard deviation. Pre- and post-laser BCVA, CMT,were analysed using paired Student’s t-test.
All the eyes were subjected to IQ 577 (577 nm) subthreshold MPLT. The Area Centralis lens (laser spot size magnification 0.94) was used for all eyes. The parameters were individualized for every patient accordingly. The titration power, which is the power that gives a just-visible reaction on the nonedematous retina temporal to macula was first estimated, starting with 50 mW in continuous wave and then gradually increasing the power by increments of 10 mW, moving to a new area each time, until a barely visible reaction was seen. After that, the mode was switched to micropulse and the power used in the treatment was quadrupled from the titration power. With a 200 µm spot size, the pulse envelope duration was 200 ms and the micropulse duration was 0.2 ms (10% duty cycle). Variable numbers of confluent zero-spacing high-density shots guided by the TxCell pattern system were applied to the whole area of leakage according to each case using the 5×5 grid pattern derived from the TxCell pattern system. Retreatment was done for eyes with persistent leakage after 3 months.
The eyes were followed up after 4 weeks, 2 and 3 months
Results:
Nineteen eyes of 17 patients (15 males and 2 females) were included in the analysis. The mean age of the patients was 40.3 years (range 25-53 years). The mean duration of leak was 7 months (range 5 months – 12 months). There were eight eyes (42%) with focal leaks and eleven (58%) with areas of diffuse leak. Of the patients with focal leaks, 3 eyes had a ‘smoke stack’ pattern and fiveeyes showed an ‘inkblot’ pattern (Figure 1).
The mean pre-treatment SRF height was 340.25μm & post treatment showed a mean reduction to 102.75μm ( Day 30) & 38.25μm (3 months) respectively(P =0.0002) .The mean CMT too improved from 428 μm to 268 μm in 3 months (p=0.006)
The laser power used in our study ranged from 240 to 480 mW. All patients showed a significant decrease in the subretinal fluid on SD-OCT. Persistent sub-macular fluid was present in 3 eyes (15%) after 3 months, for which retreatment was done. The mean BCVA improved 3 months after laser treatment from 0.46 (in logMAR) to 0.26 (P=0.009) There `was no evidence of retinal or retinal pigment epithelium damage on SD-OCT or FAF. No visible laser marks could be detected by clinical observation,SD-OCT& FAF at 4 weeks ,2 and 3 months.No patients had any other complications during the treatment or follow-up period.
Discussion:
Subthreshold micropulse laser emission without a visible burn endpoint appears to reduce the risk of structural and functional retinal laser damage, allowing treatment of foveal lesions without post-laser scotomas. It has been successfully used for diabetic macular edema and seems to be comparable to conventional argon laser.12 In 2003, Bandello et al were the first to propose subthreshold diode micropulse (SDM) photocoagulation for the treatment of CSC, showing positive results in a series of five cases.13 Ricci et al showed that SDM can provide therapeutic benefits similar to those obtainable with standard-threshold continuous-wave laser photocoagulation, but without causing discernible chorioretinal lesions, allowing almost confluent therapy and retreatment of persistent or new leaking points.14
Post MPLT, Lanzetta et al,15 reported that subretinal fluid improved in approximately 67% of cases after 1 month and in 75% at the end of follow-up. Chen et al 16 treated 26 eyes having persistent CSC with a minimum follow-up of 6 months with complete disappearance of subretinal fluid in 55% of eyes and partial resolution in 45% of the eyes. Yadav et al11 used MPLT in treating 15 eyes and reported complete resolution of subretinal fluid in 40% of the patients and partial resolution in 60% of the eyes after a follow-up period of 2 months.
In comparison to the above studies, our study demonstrated complete resolution of subretinal fluid in sixteen eyes (84%) and partial resolution in three eyes (16%) after 3 months.The complete resolution was achieved in all eyes after 5 months.
The Mean BCVA in our studyimproved similarly in comparison to reports fromAbd Elhamid et al .17Compared to the other studies(800–1,740 mW by Koss et al18 ,1,000–2,000 mW was used by Lanzetta et al15, 70–200 mW by Yadav et al11) we used less power in the range of 240 to 480 mW. This may indicate that yellow laser is better absorbed by RPE and hemoglobin thus producing the desired effects at a much lesser power. Higher pigmentation in our study population of Indian eyes also could be attributable for the less power required.
Based on the available largely retrospective literature on half-dose PDT and other PDT strategies using reduced settings, PDT may be able to achieve a faster and a complete resolution in a larger proportion (60–100%) of cCSC patients .19,20 However, there are benefits of MPLT over PDT treatment in CSC. Unlike PDT, which uses the intravenously administered light-activated verteporfin, there is no need after MPLT to be protected from bright light in the first days after treatment. In addition, choroidal neovascularization and RPE atrophy have been described in a small subgroup of PDT-treated CSC patients. MPLT presumably can be repeated more often in a safe manner. This difference is possibly due to the fact that the effect of PDT treatment leans on a suprathreshold effect on the choriocapillaris that may result in structural changes, whereas MPLT is by definition subthreshold and is aimed at the RPE.
Majority of our cases showed a diffuse leakage pattern in comparison to other studies, which had a higher proportion of focal leakages. Despite this, a good proportion of eyes responded to treatment and this is probably owing to stimulation of the RPE pump by the low-threshold confluent laser burns placed over the entire diseased RPE.
Our study had limitations with the absence of a control group, and a relatively short follow-up time and short number of cases. Another greatest limitation of MPLT is the difficulty of titrating the treatment without observing a visible reaction with a risk of under treatment.
Conclusion:
This study provides evidence that MPLT can lead to early resolution of serous retinal detachment in chronic CSC, with significant functional improvement and without leaving any sign of laser-induced lesions. The safety of this non-invasive procedure enables treatment closer to the fovea over extensive areas of RPE decompensation and retreatment over the same area as needed.There is significant anatomical and functional improvement in the treated eyes.
As the response to treatment is rapid it may be possible to offer it to patients with a significant drop in vision, in those requiring early visual rehabilitation, in those with a massive SRF, or for ‘one-eyed’ patients at the first episode itself with cost effectiveness. Treatment at an early stage may prevent recurrences and irreversible visual loss.
References:
1.Gass J: Pathogenesis of disciform detachment of the neuroepithelium. II. Idiopathic centralserous choroidopathy. Am J Ophthalmol1967;63:587–615
- Liew G, Quin G, Gillies M, FraserBell S: Central serous chorioretinopathy: a review of epidemiology and pathophysiology. Clin Experiment Ophthalmol 2013;41:201–214
- Klein ML, Van Buskirk EM, Friedman E, Gragoudas E, Chandra S: Experience with nontreatment of central serous choroidopathy. Arch Ophthalmol 1974;91:247–250.
- Gilbert CM, Owens SL, Smith PD, Fine SL: Long-term follow-up of central serous chorioretinopathy. Br J Ophthalmol 1984; 68: 815–820.
5.Khosla PK, Rana SS, Tewari HK, Azad RU, Talwar D. Evaluation of visual function following argon laser photocoagulation in central serous retinopathy. Ophthalmic Surg Lasers 1997; 28: 693–697.
6.Ober MD, Yannuzzi LA, Do DV, Spaide RF, Bressler NM, Jampol LM et al. Photodynamic therapy for focal retinal pigment epithelial leaks secondary to central serous chorioretinopathy. Ophthalmology 2005; 112: 2088–2094 30.
7.Chung YR, Seo EJ, Lew HM, Lee KH. Lack of positive effect of intravitreal bevacizumab in central serous chorioretinopathy: meta-analysis and review. Eye(Lond) 2013; 27(12): 1339–1346
- Shatz H, Yannuzzi LA, Gitter KA. Subretinal neovascularization following argon laser photocoagulation treatment for central serous chorioretinopathy: complication or misdiagnosis? Trans Sect Ophthalmol Am Acad Ophthalmol Otolaryngol 1977; 83: 893–906.
- Maruko I, Iida T, Sugano Y, Ojima A, Ogasawara M, Spaide RF. Subfoveal choroidal thickness after treatment of central serous chorioretinopathy. Ophthalmology 2010; 117: 1792–1799
- Luttrull JK, Spink CJ. Serial optical coherence tomography of subthreshold diode laser micropulse photocoagulation for diabetic macular edema. Ophthalmic Surg Lasers Imaging. 2006;37(5):370–377
- Yadav NK, Jayadev C, Rajendran A, Nagpal M. Recent developments in retinal lasers and delivery systems. Indian J Ophthalmol2014; 62: 50–54.
- Joondeph BC, Joondeph HC, Blair NP. Retinal macroaneurysms treated with the yellow dye laser. Retina. 1989;9:187–192.
13 Bandello F, Lanzetta P, Furlan F, Polito A. Non visible subthreshold micropulse diode laser treatment of idiopathic central serous chorioretinopathy. A pilot study. Invest Ophthalmol Vis Sci. 2003;44:4858.
- Ricci F, Missiroli F, Regine F, Grossi M, Dorin G. Indocyanine green enhanced subthreshold diode-laser micropulse photocoagulation treatment of chronic central serous chorioretinopathy. Graefes Arch Clin Exp Ophthalmol. 2009;247(5):597–607.
- Lanzetta P, Furlan F, Morgante L, Veritti D, Bandello F. Nonvisible subthreshold micropulse diode laser (810 nm) treatment of central serous chorioretinopathy. A pilot study. Eur J Ophthalmol. 2008;18(6):934–940
- Chen SN, Hwang JF, Tseng LF, Lin CJ. Subthreshold diode micropulse photocoagulation for the treatment of chronic central serous chorioretinopathy with juxtafoveal leakage. Ophthalmology. 2008;115(12):2229–2234
17.Abd Elhamid, Ahmed Hosni. “Subthreshold Micropulse Yellow Laser Treatment for Nonresolving Central Serous Chorioretinopathy.” Clinical Ophthalmology (Auckland, N.Z.) 9 (2015): 2277–2283
18.Koss MJ, Beger I, Koch FH. Subthreshold diode laser micropulse photocoagulation versus intravitreal injections of bevacizumab in the treatment of central serous chorioretinopathy. Eye (Lond) 2012;26(2):307–314
- Fujita K, Imamura Y, Shinoda K, Matsumoto CS, Mizutani Y, Hashizume K, Mizota A, Yuzawa M: One-year outcomes with half-dose verteporfin photodynamic therapy for chronic central serous chorioretinopathy. Ophthalmology 2015;122:555–561.
- Lim JI, Glassman AR, Aiello LP, Chakravarthy U, Flaxel CJ, Spaide RF; Macula Society CSC Collaborative Study Group, Research and Education Committee and Website Committee: Collaborative retrospective macula society study of photodynamic therapy for chronic central serous chorioretinopathy. Ophthalmology 2014;121:1073–1078
- Figure captions:
Figure 1: Ink blot leak in a case of cCSC
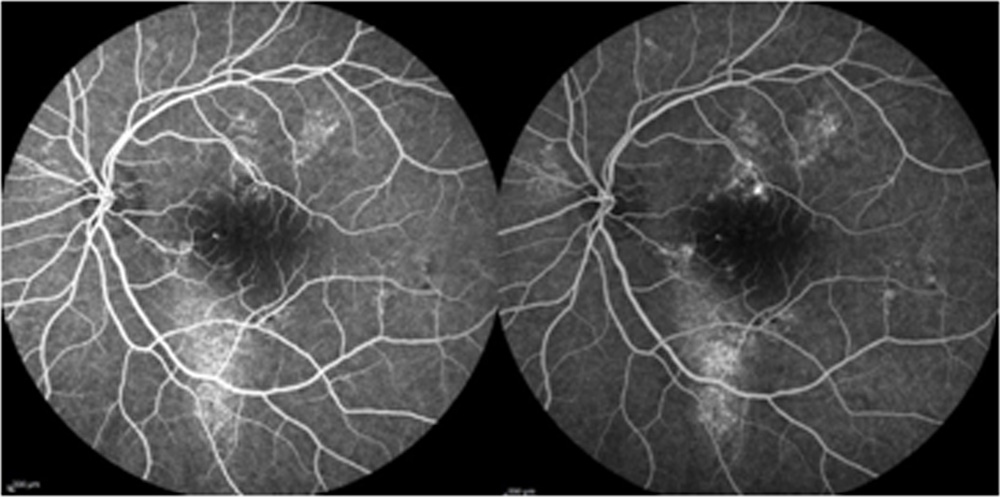
Figure 2: Residual SRF in a cCSC post MPLT 3 months
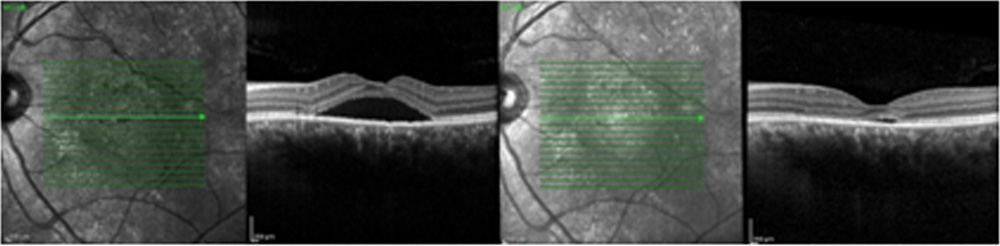
Figure3: Smoke stack in a cCSC
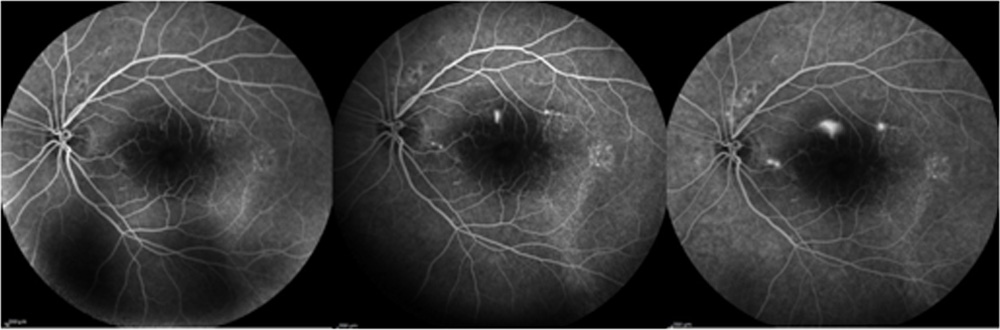
Figure 4: Complete resolution of SRF

Figure :5 Resolution of SRF following confluent MPLT to the diffuse leaks
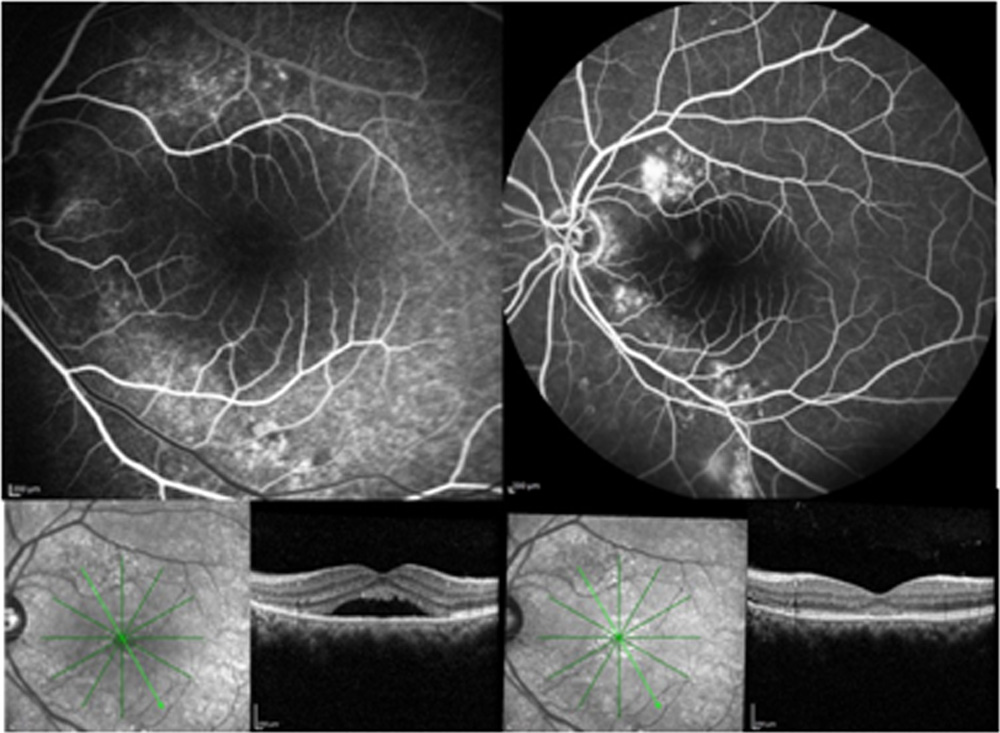
Table :1 Resolution of SRF post MPLT at 3 months
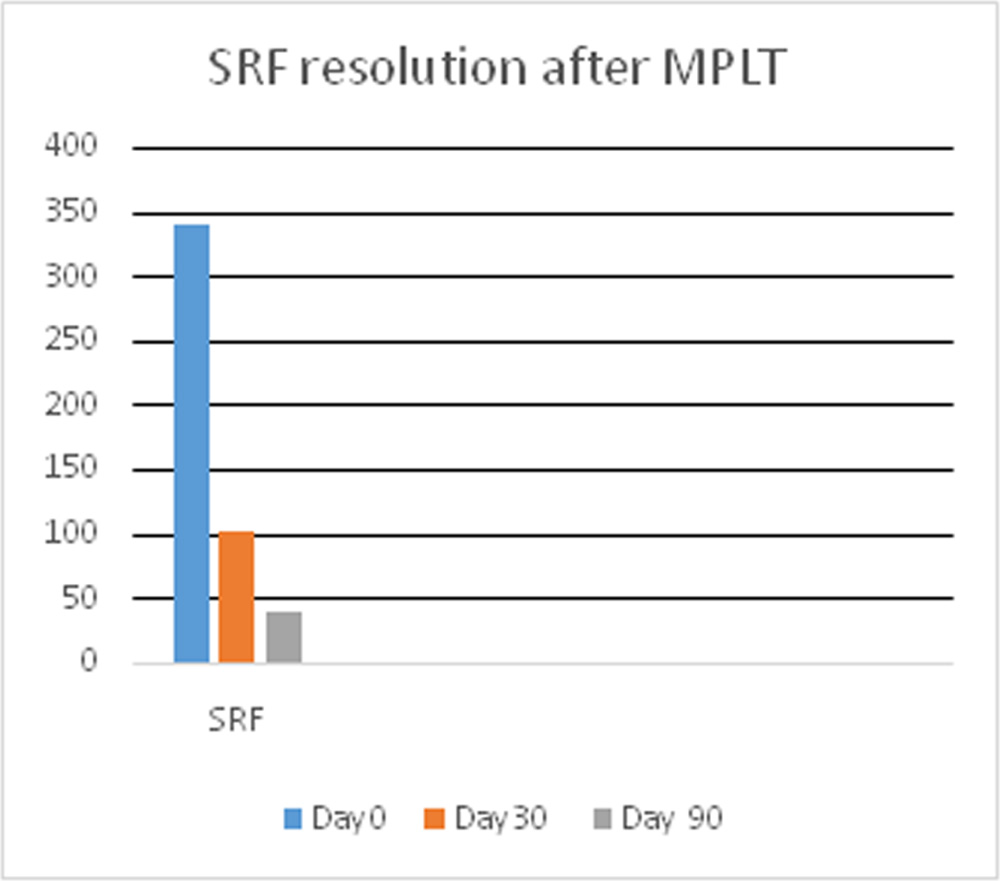
Table :2 logMAR post MPLT
Leave a Comment