
![]()
Dr. Shivani Nayak, N17084, Dr. Rekha Gyanchand, Dr. Kaustubh Mulay, Dr. Jyotirmay Biswas, Dr. Shivani Nayak
ABSTRACT:
PURPOSE:To analyze the presence of gross or microscopic metastatic cells in ocular tissue with systemic malignancy.
METHODS:A prospective study of 103 eyes from 52 donors who donated eyesto the Eye Bankand whose cause of death was malignancy with metastasis studied. Details pertaining to malignancy were checked from the hospital medical records of the donor.After gross and slit-lamp examination, the eyes were preserved in formalin for Histo-pathological study.
RESULTS: Most common primary cancer in our study was leukemia and CNS malignancies(11.53%).On gross/slit-lamp examination,1 pair of eyes from testicular carcinoma had abnormal infiltrates in uvea and 1 pair from promyelocytic leukemia had abnormal infiltrates in optic nerve.On microscopic examination,5 eyes(4.58%) had malignant cells of which 2(1.94%) were in choriocapillaris, 2(1.94%) in ciliary body and 1(0.97%) in choroid..
CONCLUSION:The incidence of corneal metastasis with active solid carcinoma is nil. The most common site of intra-ocular metastases is uvea.
KEY-WORDS:Ocular Metastases, Systemic Malignancy, Eye Donors.
INTRODUCTION :
In an eye-bank 30-40% of eye donations are procured from donors with cancer as the cause of death, especially in an urban setup.Most eye bank associations, due to the potential risk of transmission of diseases through corneal transplantation, consider malignancies to be a contraindication for keratoplasty1. There is a significant difference between the number of corneas needed for treating corneal blindness and the number of corneas procured2, especially in India. If eyes from patients dying of cancer can be used for transplantation without fear, then it can help to reduce the shortage of donor corneas and in turn number of corneal blindness. Hence this study was planned.
OBJECTIVES:
- AIM: Histopathological examination of ocular tissue to rule out ocular metastasis from donors with systemic cancer as cause of death.
To analyse the following:
- Presence or absence of tumor cells in ocular tissue by histopathologic examination in cancerous donors.
- To identify commonest site of microscopic malignant cell deposits in the eye.
METHODOLOGY:One year descriptive cross sectional study of 103 eyes of 52 patients with systemic malignancy
INCLUSION CRITERIA: Enucleated eyes from donors diagnosed with cancer, either solid or haematological , were accepted.
EXCLUSION CRITERIA:
- Keratitis
- Phthisis bulbi
- Disorganized globe
After enucleation, the eyes were subjected to gross examination, detailed slit lamp evaluation and histopathological analysis. Those that had a high index of suspicion of malignancy on microscopy were subjected to Immuno-Histo-Chemistry(IHC) for confirmation.
RESULTS:
The data obtained was analyzed and the final observations were tabulated as below. The statistical analysis was performed by STATA 11.2 (College station TX USA).
During the period of study , the total number of eyes collected in our Eye bank was 1398 and 103 eyes were obtained from donors with a history of systemic malignancy. This constituted 7.36% of the donated eyes. In this study most of the donors were of the age between 61 to 80 years (53.84%) and followed by 41 to 60 years (28.84%). The mean age was 61.43 ± 14.68 years (Range : 25 to 87 years).In the present study 51.93% of the donors were females and 48.07% were males. The male to female ratio was 0.92:1.
36 patients out of the 52(69.23%) had been diagnosed of cancer 1-5 years before their death. The mean duration of malignancy, i.e; the duration from diagnosis of malignancy to death was 2.37 ± 2.05 years. (Range: 15 days to 9 years).
51.92%(27) among the 52 donors had metastases to some organ. Among them, the most common site of metastases was to the lung in 11.54%, followed by liver in 9.61% and peritoneum (7.69%). Abdominalmetastasis in total was present in 9 donors (17.03%). 5 donors had multi-organ metastases which included 2 patients with a cervical lymph node involvement amongst them.25 donors (48.07%) did not have any metastases.In the present study among the 52 donors examined, 7 patients (13.46%) had head and neck region metastases of whichthe most common site of metastases was to the cervical group of lymph nodes in 6 donors (11.53%) and 1 patient (1.92%) had metastasis to the brain (primary-ovary).The most common primary malignancies causing the metastases to head and neck region were: brain(2) and 1 each from thyroid, lung, stomach, ovary and testis.
Among the total number of 52 donors, 9 people had not received any form of treatment for their primary condition. Among the people who received treatment of some form, the mean duration of treatment received was 19.06 ± 16.92 months. (Range: 15 days-6 years). Only 5 (9.61%) among the donors had received some treatment for their primary malignancy in the previous 1 month.
TABLE-1 SHOWS THE DISTRIBUTION OF PRIMARY MALIGNANCIES IN EYE DONORS
| Primary Malignancy | Distribution (n=52) | |
| Number | Percentage | |
| Hematological Malignancies
Leukemias Hodgkin’s Lymphoma Non-Hodgkin’s Lymphoma Multiple Myeloma |
06 03 02 01 |
11.53 05.76 03.84 01.92 |
| CNS Malignancies
Brain umors |
06 |
11.53 |
| Breast Malignancies | 02 | 03.84 |
| Bone Malignancies | 01 | 01.92 |
| Gastrointestinal Malignancies
Esophageal Carcinoma Gall Bladder Carcinoma Pancreatic Cancer Stomach Cancer Colorectal Cancer |
04 01 02 02 02 |
07.69 01.92 03.84 03.84 03.84 |
| Urogenital Malignancies
Renal Cancer Testicular Cancer Prostate Cancer Uterine Cancer Ovarian Cancer |
02 04 02 01 03 |
03.84 07.69 03.84 01.92 05.76 |
| Lung Cancer | 03 | 05.76 |
| Laryngeal Cancer | 01 | 01.92 |
| Thyroid Cancer | 03 | 05.76 |
| Maxillofacial Cancer | 01 | 01.92 |
| TOTAL | 52 | 100.00 |
TABLE-2 SHOWING: DISTRIBUTION OF GROSS OCULAR ABNORMALITIES
| Gross Abnormalities | Distribution (n=103) | |
| Number | Percentage | |
| Iris-Choroid | 02 | 01.94 |
| Optic Nerve | 02 | 01.94 |
| No Gross Abnormality | 99 | 96.12 |
| TOTAL | 103 | 100.00 |
BAR-DIAGRAM-1 SHOWING DISTRIBUTION OF MICROSCOPIC OCULAR CHANGES
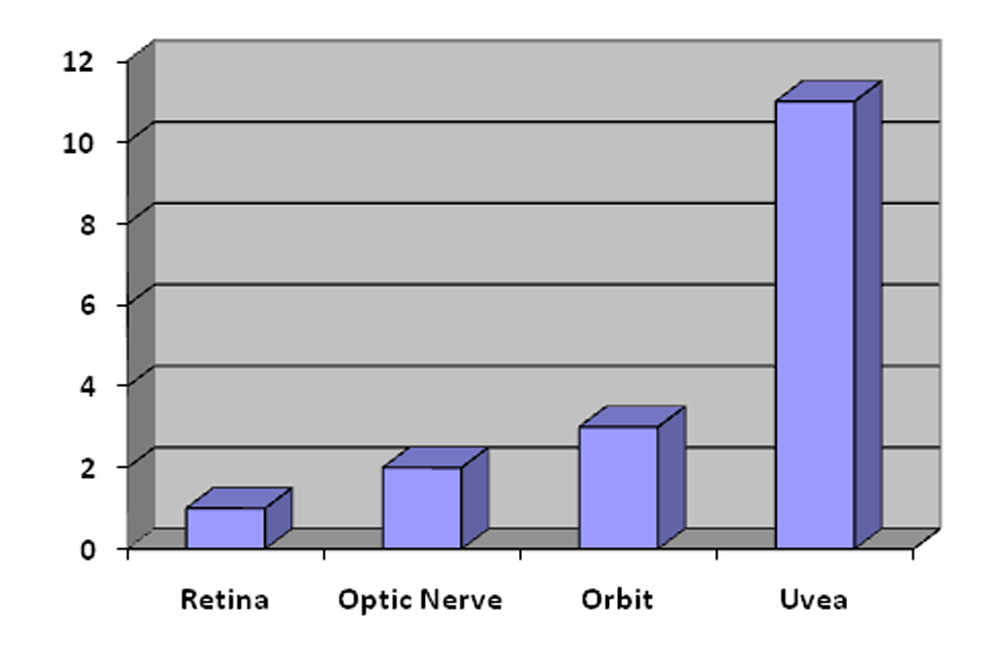
In 1 patient with a testicular cancer, only the retina of the left eye showed a peripheral retinal inflammatory infiltrate.
In 1 patient with Acute Promyelocytic Leukemia, the optic nerve of 1 eye showed the presence of abnormal mononuclear cell infiltrates.At the same time the orbital tissue of the same patient showed perivascular infiltration of similar looking mononuclear cells.
In a patient with a Non-Hodgkin’s Lymphoma, there were atypical lymphoid cell aggregates noted in the peri-orbital fat tissue as well as the optic nerve of the left eye. But immunohistochemistry studies in all 3 cases confirmed that none of the cellular infiltrates in neither the retina, optic nerve nor the orbital tissue were malignant cells.
Image 1 (left) shows the Microscopic photograph of atypical lymphoid aggregates and Image 2 (right) shows Immunohistochemistry negative for malignant cells
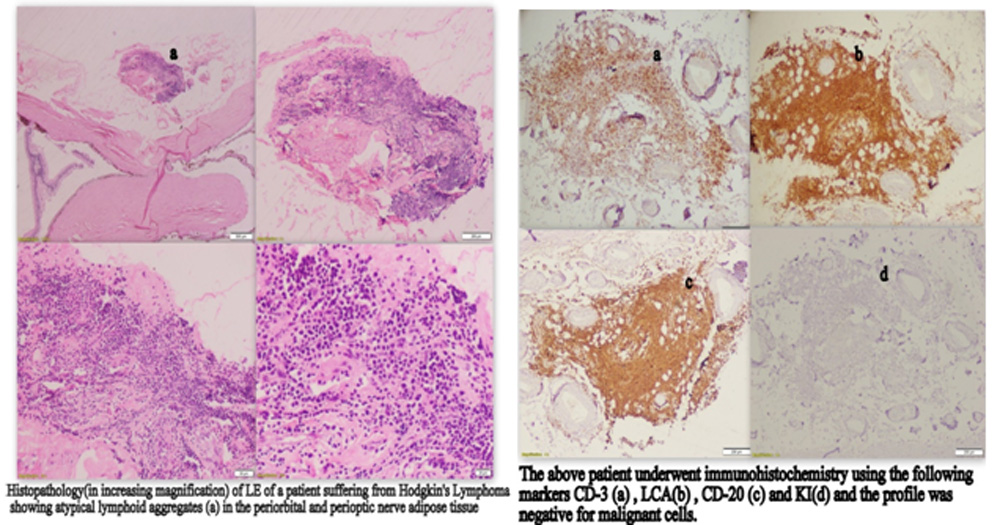
TABLE-3 SHOWS THE DISTRIBUTION OF CHANGES IN THE UVEA NOTED ON MICROSCOPIC EXAMINATION.
| Microscopic Changes in the Uvea | Distribution (n=103) | |
| Number | Percentage | |
| Abnormal infiltrates in blood vessels | 02 | 1.94 |
| Autolytic changes in the choroid | 01 | 0.97 |
| Inflammatory infiltrates in the iris | 02 | 1.94 |
| Inflammatory cells in the cilia | 01 | 0.97 |
| Malignantcells in thechoriocapillaris | 02 | 1.94 |
| Malignant cells in Iris | 01 | 0.97 |
| Malignant cells in the ciliary body | 02 | 1.94 |
| No abnormality | 92 | 89.32 |
| TOTAL | 103 | 100.00 |
On microscopic examination of the uvea , abnormal infiltrates in blood vessels was seen in 2 eyes (1.94%) , abnormal spindle shaped cells were seen 2 eyes (1.94%), inflammatory cells in the iris were found in 2 eyes (1.94%) and a single eye showed autolytic changes in choroid (0.97%). 5 eyes showed malignant cells in the uvea.
BAR- DIAGRAM-2 SHOWS THE DISTRIBUTION OF MALIGNANT CELLS AMONG THE DONOR SPECIMENS.
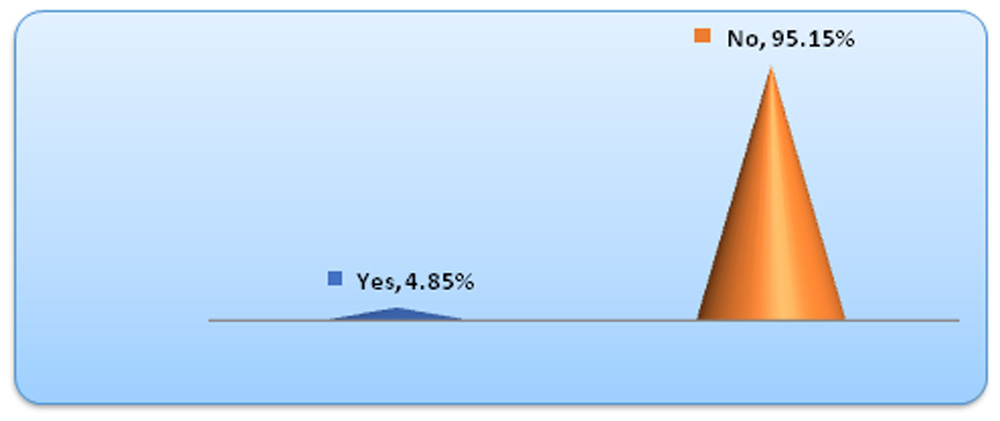
4.85%(5) of the total of 103 eyes examined were showing presence of malignant cells. Among them 2 eyes belonged to a patient having an astrocytoma of the brain, 2 belonged to a patient having adenocarcinoma of the uterus and a 1 single left eye from a patient with testicular cancer showed the presence of malignant cells.All the malignant cells were seen in the uvea of the specimen eyes.
DISCUSSION :
Cancer is the second leading cause of death in developed countries like United States of America[3] and it accounts for 20-25% of all deaths[4][5][6]. With the increasing number of deaths associated with cancer, there is a large pool of donors which can be used for corneal transplantation but are not being used at present. Literature in the past has shown transmission of malignancy in the recipient after corneal transplantation[7][8] which has caused a dilemma amongst corneal surgeons about the safety of using corneas obtained from donors dying of cancer.
But newer studies where corneas from patients dying of cancer have been used for transplantation and the recipients followed up for a long duration of time show no evidence of occurrence of the malignancy in the recipients[1][9][10]. In a developing country like India, with a very large number of cases of corneal blindness and the donor corneas being a scarce resource, every possible attempt to increase the size of the donor pool should be made.This present study was thus aimed at expanding the inclusion criteria of the eligible donor corneas.
In this present study, the histopathological examination showed that 05 (4.85%) of the total of 103 eyes examined were showing presence of malignant cells. Among them 2 eyes belonged to a patient having an astrocytoma of the brain, 2 belonged to a patient having adenocarcinoma of the uterus and a 1 single left eye from a patient with testicular cancer showed the presence of malignant cells. All the malignant cells were seen in the uvea of the specimen eyes. In a study conducted by Nelson et al, microscopic metastatic intraocular lesions were found in at least one eye in 5–10% of people dying of malignancy [11].
These microscopic examination findings were consistent with previous studies which said the percentage of ocular metastases was between 4-7% (present study was 4.85%). The most common site for metastases noted in this study like previous studies was the uveal tract. Among the uveal tract we found that the most common sites were the choroid and ciliary body (40% each) followed by iris (20%). Other studies have noted that the choroid was the commonest site among the uvea in as many as 88% of cases[12][13].
TABLE-4 SHOWING COMPARISON OF SIMILAR STUDIES
| No.of donors with cancer | Most common primary malignancy | Ocular metastasis(No. of Eyes) | Most common site | |
| Eliassi-Rad etal14(1976-80) | 1043 (9.02%) | Lung(21.86%) | 128(12.2%) | ___ |
| Nelson et al15 (1973-1983) | 358 | Leukemia(32.68%) | 66(9.3%) | ___ |
| Lopez-Navidad et al1 (1999-2003) | 204(34.7%) | Lung(18.8%) | 4(1%) | Choroid(88%) |
| Present study(Dec. 2015- Dec 2016) | 52(7.36%) | Leukemia(11.53%)
Brain Tumor (11.53%) |
5(4.85%) | Choroid (40%)
Ciliary body (40%) |
In the present study we found 4.85% of eyes with microscopic malignant cells infiltration. This is lower than reported in literature. Various studies have shown no transmission of cancer cells from donor to recipient. Barring lymphoproliferative disorders and primary malignancies of the eye, eyes obtained from other malignancies may be considered for transplantation as there are very few proven studies on cancer transmission from donor to recipient.Some limitations in our study were that specular study of the corneas obtained were not done .Ultrasound Bio-Microscopy of the angle was not done to look for any abnormal infiltrates.
CONCLUSION :
Results suggest that ocular metastatic involvement in patients dying from active solid carcinoma is very low and transmission of malignancy is highly unlikely when there is no tumour infiltrate to the eye. Corneal donors with cancer represent a high percentage of corneas viable for transplantation. The results also suggest that the most common site of intraocular metastasis is uvea.
RECOMMENDATIONS:
In the selection of corneas for transplantation from donors dying of malignancy the following recommendations are suggested
- Absolute contraindication if malignancy is due to known viral etiology, blood and lymphatic system. Chemotherapy or radiation within 1 month of death.
- Enucleation must be the procedure of choice in eye donors where the cause of death is cancer
- After cutting the optic nerve look for any visible abnormality in the nerve such as thickness and grittiness of the nerve.
- Eyes with macroscopic tumour masses should be rejected.
- Cornea , iris and the anterior chamber of the eyes should be carefully evaluated on slit lamp to look for any gross tumour infiltrates or suspicious lesions such as patchy depigmentation
- Vascularized cornea with or without scarring should be avoided as these have higher chances of having
- The corneoscleral button may be preserved in optisol and the rest of the eye ball subjected to histopathological examination.
- If the cornea is used for transplantation, the corneoscleral rim must be subjected to histopathological examination and the recipient should be followed up for atleast 2 years.
- Do not use the corneas in children or for keratolimbal grafts.
REFERENCES :
- López-Navidad A, Soler N, Caballero F, Lerma E, Gris O. Corneal transplantations from donors with cancer. Transplantation. 2007 May 27;83(10):1345-50.
- Understanding donation [Internet].Banjarahills,Hyderabad,India: www.ebai.org.Welcome to E.B.A.I – Eye Bank Association of India [Internet].2015[cited 30 December 2015. Available from: https://ebai.org/understanding -donation.php
- Longo DL. Approach to the patient with cancer. In:Kasper DL , Fauci AS, Hauser SL, Longo DL, Jameson JL,Loscalzo J , editors. Harrison’s Principles of Internal Medicine. 19th New York : McGraw Hill;2015.p.467.
- Kumar V, Abbas A K, Aster J. Pathologic Basis of Disease. 9th Philadelphia : Saunders Elsevier;2015.p.266-329.
- Augsburger JJ, Guthoff R, Correa ZM. Metastatic Cancer to the Eye. In :Yanoff M , Duker JS. Ophthalmology. Philadelphia: Elsevier;2014.p.810.
- Parker SL, Tong T, Bolden S, Wingo PA. Cancer statistics, 1997. CA Cancer J Clin.1997 Jan-Feb; 47(1):5-27.
- Yao X, Lee M, Ying F, Huang L, Qi W, Zhao P, et al. Transplanted corneal graft with metastatic cholangiocarcinoma to the donor eye. Eye Contact Lens. 2008 Nov;34(6):340-2.
- Campanelli M, Mistò R, Limongelli A, Valente MG, Cuttin MS, Tóthová JD. A donor cornea with metastatic cells from a cutaneous malignant melanoma. Cornea. 2013 Dec;32(12):1613-6.
- Salame N, Viel JF, Arveux P, Delbosc B. Cancer transmission through corneal transplantation. Cornea. 2001 Oct;20(7):680-2.
- Wagoner MD, Dohlman CH, Albert DM, Lavin P , Murphy A, O’Neill-Dryja M. Corneal donor material selection. Ophthalmology. 1981 Feb;88(2):139-45.
- Nelson CC, Hertzberg BS, Klintworth GK: A histopathologic study of 716 unselected eyes in patients with cancer at the time of death. Am J Ophthalmol.1983 Jun; 95(6):788-93.
- Longo DL. Approach to the patient with cancer. In:Kasper DL , Fauci AS, Hauser SL, Longo DL, Jameson JL,Loscalzo J , editors. Harrison’s Principles of Internal Medicine. 19th New York : McGraw Hill;2015.p.467.
- Das C, Shields CL. Radiotherapy for iris metastasis from esophageal carcinoma: A series of three cases. Oman J Ophthalmol. 2016 May-Aug;9(2):93-6.
- Eliassi-Rad B, Albert DM, Green WR. Frequency of ocular metastases in patients dying of cancer in eye bank populations. Br J ophthalmol. 1996 Feb ;80(2):125-8.
- Nelson CC, Hertzberg BS, Klintworth GK: A histopathologic study of 716 unselected eyes in patients with cancer at the time of death. Am J Ophthalmol.1983 Jun; 95(6):788-93.
Leave a Comment