
Dr. Gaurav Gupta, G19315, Dr. Ramandeep Singh, Dr. Vishali Gupta, Dr. Jagat Ram
ABSTRACT:
Purpose: assess the post-operative inflammation using laser flare photometer, following phacoemulsification with or without single intraoperative intravitreal dexamethasone (DEX) implant in addition to standard of care, in patients of uveitis with cataract
Methods: 30 eyes of uveitic cataract were randomized into 2 groups (i)standard of care (SOC group) (ii)Dexamethasone implant (DEXA group).Both the groups underwent phacoemulsification with Intraocular lens implantation but DEXA group additionally received intraoperative intravitreal DEX implant. Patients were followed at least till 6 months
Results: DEXA group had significantly less (P<0.05) postoperative flare. Recovery of flare occurred early in DEXA group. Mean CMT (P<0.04) and BCVA (P=0.02) was significantly lower in DEXA group. 37.5% cases developed CME in SOC group but none in DEXA group
Conclusion: DEX implant is a safe and effective option for preventing and managing the postoperative inflammation in uveitic cataract cases
Keywords: laser flare photometer, phacoemulsification, intravitreal dexamethasone implant, uveitic cataract.
Introduction
Uveitis is not an uncommon disease in developing countries and is a common cause of blindness. About 25% of blindness in India and other developing countries is attributed to uveitis and its complications.1 Cataract is the most common complication (approx 35% of patients) of uveitis.2 In patient of uveitis with cataract, blindness can be easily prevented by doing cataract surgery, but performing cataract surgery in eyes with uveitis is a challenge. Cataract surgery in uveitis has high chances of postoperative flare up of inflammation and macular edema. As per guidelines, cataract surgery done after control of all inflammatory activity for at least a period of 3 months is associated with favorable outcomes3-5 and therefore regular perioperative monitoring of inflammation is important.
Traditionally, inflammation has always been monitored using slit lamp biomicroscopy, by assessing cellular reactions and flare in the preoperative and postoperative period.6 But this method of monitoring is subjective and results vary from observer to observer, so various methodologies have been tried for objective assessment.
Laser flare photometry (LFP) is an objective and quantitative method, developed in the late 1980s, by Kowa Company, Ltd., Electronics and Optics Division (Tokyo, Japan) that enables accurate measurement of parameters of inflammation with high reproducibility.7 It also allows detection of subclinical subtle pathological changes that could not have been recorded otherwise.8 It can be an important and valuable tool to remove the observer bias in grading flare in patients of uveitis. So, LFP is superior to traditional slit-lamp evaluation in monitoring anterior chamber inflammation in uveitis patients and has become a quantitative parameter.9-12
Patients of uveitic cataract are usually managed by phacoemulsification and intraocular lens (IOL) implantation, but managing such cases in the postoperative period is a challenge due to related complications like postoperative increase of inflammation, macular edema and recurrent uveitis.5,13-15 To control the inflammation postoperatively, oral steroids have been used since long time but they are associated with serious systemic as well as local side effects on long term use.16,17 So need for an alternative to systemic steroids for controlling postoperative inflammation, following cataract surgery in uveitis patients has been realized and various alternatives have been tried.
Triamcinolone acetonide (Kenacort) is a corticosteroid that was tried to be given by various routes, but its intravitreal injection was associated with raised intraocular pressure (IOP)18 and posterior sub-tenon injection was associated with lid ptosis.17,19. The sustained release intravitreal fluocinolone acetonide implant (RetisertÒ, Bausch and Lomb, Rochester, NY) was also tried but its use was associated with IOP rise in a significant number of patients.20
Dexamethasone Posterior Segment Drug Delivery System (Dexamethasone DDS – Ozurdex®, Allergan Inc, Irvine, California), a sustained release intravitreal implant containing 700µg Dexamethasone has been approved by the US-FDA (Food and Drug Administration) for treatment of diabetic macular edema, macular edema in retinal vein occlusions and non-infectious posterior uveitis.21 It has a longer duration of action (approx 6 months) and can provide a source of prolonged but steady drug delivery.22
Gupta et al,23 have used Ozurdex during cataract surgery in uveitis patients to control postoperative inflammation and showed it effective in controlling post cataract surgery inflammation but that study involved assessment of inflammation using slit lamp biomicroscopy examination, which is a subjective method and also randomization was lacking in their study.
In this prospective single masked randomized study we have compared intravitreal Dexamethasone implant (OzurdexÒ) in addition to standard of care (SOC) for uveitis and standard of care alone in controlling postoperative inflammation following phacoemulsification for uveitic cataract, which was measured using laser flare photometry. To the best of our knowledge, this is first of its kind, randomized controlled study in which LFP have been used to measure efficacy of dexamethasone implant in controlling inflammation in uveitis patients undergoing cataract surgery.
Methods:
This is a prospective study, which included 30 eyes of 30 patients with anterior, intermediate or posterior uveitis with visually significant cataract attending the Uveitis or Cataract and Refractive Surgery Clinic of ‘Advanced Eye Centre, PGIMER, Chandigarh’ between 1st July, 2015 and 31st March, 2016 after informed consent and ethical clearance from the Institutional Ethical Committee. All procedures adhered to the tenets of Declaration of Helsinki and were conducted in accordance with the approved research protocol. These 30 patients were randomized using randomization chart into the following two groups:
Group 1 (Standard of care group): comprised of patients, who underwent phacoemulsification with posterior chamber IOL implant and received standard of care for uveitis perioperatively
Group 2 (DEXA Implant group): comprised of patients, who underwent phacoemulsification with posterior chamber IOL implant and received intravitreal Dexamethasone implant during surgery, in addition to standard of care for uveitis perioperatively.
Here, standard of care for uveitis means ‘standard treatment which is usually given for uveitis, in the form of steroids (oral or topical) or any other form of immunosuppresive agents to control the inflammation preoperatively and on which ocular inflammation was controlled’.
The patients of either sex with age 15 yrs or more were included in our study. We enrolled the patient with either anterior, intermediate or posterior uveitis with visually significant cataract (BCVA<6/12) and control of uveitis (period of quiescence) for at least 3 months prior to cataract surgery with preoperative Laser flare photometer readings <50 photon units/msec
The study excluded: (i) Patients with active uveitis; (ii) Patients with history of steroid induced glaucoma or ocular hypertension (iii) Patients with scleritis; (iv) Patients with diabetes mellitus; (v) Intra-operative complications like posterior capsular rupture, hyphaema, etc; (vi) Pregnant or lactating mothers
Preoperative evaluation:
Detailed history was taken, including ocular and systemic complaints, from the patient followed by general physical examination and systemic evaluation to rule out any significant systemic illness. Then extensive ocular examination was done which included, recording the preoperative BCVA using the Snellen’s chart and the ETDRS chart. Intraocular pressure was recorded by Goldman Applanation Tonometry. Slit lamp biomicroscopic examination was done to evaluate anterior segment, to assess anterior chamber reaction, keratic precipitates or any other signs of inflammation. The presence of posterior or anterior synechiae was also noted. Laser flare photometry was done to estimate the flare in anterior chamber. The pupillary dilatation was done for grading of cataract and posterior segment examination. Posterior segment examination was done using 90D lens on slit lamp or 20D lens for indirect ophthalmoscopy. Intraocular lens power was calculated using IOL master or biometry (Carl Ziess, Meditech.)
Preoperative instructions:
Patients with visually significant cataract, posted for surgery, were instructed to instill moxifloxacin eyes drops (0.5%) 6 times one day prior to surgery. Pupillary dilatation (if possible) was achieved using tropicamide (0.8%), phenylephrine hydrochloride (5%), cyclopentolate (1%) and ketorolac (0.5%) eye drops, instilling three times half hourly before the surgery
Surgical procedure:
Patients were admitted one day prior to surgery (if needed) or surgery was done on day care basis or on outpatient basis. Same experienced surgeon (JR) performed all the surgeries, strictly adhering to principles of closed chamber technique in both the groups. Written informed consent was taken from every patient before the surgery. All surgeries were performed under local anesthesia using peribulbar or retrobulbar block. After adequate anesthesia, intravitreal 700µg Dexamethasone Implant was given 3.5mm away from the limbus inferotemporally in DEXA implant group patients only. Two side port incisions were created at 9 and 2 o’clock position using 150 disposable knife and main port was made using 2.2mm disposable keratome. The anterior chamber was formed using high viscosity viscoelastic (1.4% sodium hyaluronate). Small pupils were managed using Iris hooks or Malyugin’s ring. A 5-5.5mm continuous circular capsulorrhexis was made using Uttrata’s forceps. In cases of white cataract, trypan blue dye (0.06%) was used to stain anterior capsule. Cortical cleavage hydrodissection was performed with nuclear rotation. Lens nuclear emulsification was done by phacoemulsification. The cortical matter was removed by bimanual irrigation-aspiration (I/A). Foldable hydrophobic acrylic IOL was implanted in the capsular bag in all cases. A subconjuctival injection of gentamycin (20mg) and Dexamethasone (4mg) was given at the end of surgery.
Postoperative care:
After the surgery, patients of both the groups were given moxifloxacin eye drops (0.5%), 6 times per day initially and then tapered over a period of 4 weeks; betamethasone (0.1%), 10-12 times per day initially, which was tapered according to the postoperative inflammatory response of the eye; topical cycloplegic agents like atropine (1%) or homatropine (2%) was also given. The patients in both groups received standard of care treatment for uveitis.
Postoperatively, all the patients of both the groups were followed on day 1, day 3, 1 week, 2 weeks, 4 weeks, 6 weeks, 12 weeks and 24 weeks. All patients were followed up atleast for 24 weeks. Following parameters were assessed in each group at every follow up visits: (i) Best corrected visual acuity (with Snellen’s and ETDRS chart at every visit); (ii) Intraocular pressure by Goldmann applanation tonomery; (iii) Central macular thickness at 6wks, 12wks, 24wks (using 7 line-Raster Scan of Spectral Domain OCT); (iv) Anterior chamber reaction clinically using slit lamp biomicroscopy; (v) Inflammatory response using laser flare photometer; (vi) Anterior and posterior segment photographs as and when required.
Statistical Analysis
All the data was tabulated in an excel sheet.
Commercially available software (SPSS 17.0, SPSS Inc, Chicago, IL) was used for statistical analysis. We compared the intraocular pressures, best corrected visual acuity, flare and the central macular thickness between the two groups.
The parameters were analyzed using the Kolmogrov-Smirnov test for normality. The unpaired T-test was used to compare the parameters of the two groups at the various follow up periods and the paired T-test was used to compare the data within the group.
Results
30 eyes of 30 patients with cataract and uveitis were included in the study and were then randomized into 2 groups using randomization chart; Group A (16 patients): those receiving standard of care treatment for uveitis perioperatively with cataract surgery (SOC group) and Group B (14 patients): those receiving intravitreal dexamethasone implant with cataract surgery in addition to perioperative standard of care treatment for uveitis (DEXA group).
In our study population, out of these 30 patients, 10 were males and 20 were females with a mean age of 49.36 ± 12.46 years (ranging from 26 to 72 years). 16 patients were of anterior uveitis, 5 of intermediate uveitis and 9 of panuveitis. 17 operated eyes were left and remaining 13 were right. Preoperatively, all eyes were quiet and had no cellular reaction and mean flare readings on LFP were 17.9 ± 12.9 photon units/msec. Intraoperatively, in 5 cases there was no synechia and pupil was fully dilated; in 8 patients Malyugin’s ring was used; in 5 patients iris hooks were used and in remaining 12 cases viscosynechiolysis was done for pupillary dilatation.
Both the groups were age and sex matched. Preoperatively, mean logmar BCVA in SOC group was 0.56±0.21 and in DEXA group was 0.48±0.20; mean IOP in SOC group was 15.5±3.3 mm of Hg and in DEXA group was 14.7±3.3 mm of Hg; mean LFP readings in SOC group was 21.0±14.1 photon units/msec and in DEXA group was 14.4±10.6 photon units/msec (Table 1).
Visual Acuity
Mean LogMar BCVA at various postoperative follow up visits is shown in Table 2.
In between these groups, there was no significant difference in BCVA at immediate postoperative period i.e. at day 1, day 3, 1 week and 2 week, but there was a statistically significant difference in late visual outcome i.e. at 1 month, 3 month and 6 months and DEXA group achieved significantly better visual outcome (fig 1). In DEXA group all patients achieved vision better than or equal to 6/12 but in SOC group 4 patients had vision worse than 6/12; 2 patients had persistent CME and 2 had epiretinal membrane (ERM).
Intraocular Pressure (IOP)
Postoperative mean IOP at various follow up visits is shown in Table 3.
Postoperative IOP was within normal limits in both the groups and in between these groups, there was no statistical difference in mean IOP at any visit. There was high IOP in 3 cases (2 in SOC group and 1 in DEXA group) on postoperative day 1 (IOP > 21mm of Hg), which was managed and controlled using tablet acetazolamide for 3 days. There was no need of any long term anti glaucoma therapy in any patient. There was no IOP spike in any case on any other follow up visit.
Laser Flare Photometry (LFP)
Postoperative mean LFP readings at various follow up visits is shown in Table 4.
Flare as recorded by LFP increased suddenly on immediate postoperative day 1 of surgery and then started decreasing in the subsequent follow up visits. On postoperative Day 1, flare spike was low in DEXA group as compared to SOC group but was not statistically significant. On subsequent visits on postoperative Day 3, 1 week, 2 week, 4 week, 12 weeks and 24 weeks; the flare was significantly lower in DEXA group as compared to SOC group. Interestingly, in both the groups final flare came down to the preoperative value. In DEXA group, it came down to preoperative value within 4 weeks whereas it took 3 months in SOC group to come down to preoperative value, i.e. settling down of inflammation occurred very early in DEXA group as compared to SOC group (Fig 2). The maximum recorded flare in DEXA group was 188.2 photon units/msec whereas it was 492.3 photon units/msec in SOC group.
Central Macular Thickness (CMT)
The values of mean CMT at various postoperative follow-up visits are shown in Table 5.
Central macular thickness was significantly lower in DEXA group as compared to SOC group at postoperative 6 weeks and 24 weeks. At 12 weeks also, CMT was lower in DEXA group than SOC group but it was not statistically significant, this might be due to starting of rescue treatment in patient developing CME at 6 weeks, thereby decreasing their CMT. 6 patients in the SOC group developed CME, out of which 5 patients developed CME at 6 weeks follow up and 1 patient developed it at 24 weeks follow up. No patient in DEXA group developed CME.
Complications
In SOC group, 6 patients (37.5%) developed CME during follow up visits, which were treated with either oral steroids or topical NSAIDs, depending upon severity; 1 (6.25%) patient had fibrin in the anterior chamber on postoperative day 1; 1 (6.25%) patient developed postoperative hypotony (IOP<10mm Hg), which was managed with high potent topical steroids. No patient in DEXA group had any CME, hypotony, fibrin, IOP rise (after 1 week of surgery) in follow up visits but 1 patient had vitreous hemorrhage after injecting the implant, which was noticed postoperatively and resolved spontaneously and without any surgical treatment. 2 patients in SOC group and 1 patient in DEXA had flare of inflammation during follow up visits, which was managed with topical steroids. This flare up of inflammation occurred at 3 months in DEXA group but occurred as early as 2 weeks and 6 weeks respectively in SOC group. Steroid induced ocular hypertension or glaucoma did not occur in any of the groups and no patient required laser capsulotomy.
Discussion
Sustained release Dexamethasone implant (OzurdexÒ) is FDA approved for Diabetic Macular edema, non-infectious posterior uveitis and macular edema related to retinal diseases. Its role and efficacy in treating recalcitrant macular edema in posterior uveitis is well established,24 but its role in controlling inflammation after cataract surgery in uveitis patients is not proven. There is only one report, evaluating its efficacy during cataract surgery in patients of uveitis, which was not a randomized study and they measured inflammation clinically (no objective method was used to measure postoperative inflammation).23 Our study is a first of its kind, which is a single masked randomized control study, evaluating the viability of simultaneously implanting a dexamethasone drug delivery system intraoperatively in combination with phacoemulsification and IOL to treat the patients with visually significant cataract and severe, chronic, uveitis and compare it with standard of care for uveitis. Moreover, in our study, inflammation was measured objectively with the help of Laser Flare Photometry (LFP), thereby removing observer bias. Visual outcomes, flare, IOP, CMT and other postoperative sequelae were assessed and evaluated over a period of 6 months. In the DEXA group, there was early and excellent control of postoperative inflammation over an extended period, with better visual outcomes and less complications.
Inflammation is the main culprit in causing unfavorable surgical outcome in uveitic cataract patients. Inflammation is usually measured clinically, but LFP is an objective method of quantification of inflammation. To the best of our knowledge, LFP has been used for the first time in our study for measuring the outcome of cataract surgery in uveitis patients. In our study we found that in both the groups initially in the immediate postoperative period, there was spike of flare, which was as high as 492.3 photon units/msec in SOC group and 188.2 photon units/msec in DEXA group, which then started decreasing and then came back to its preoperative value in the follow up period. The flare rise was significantly lower in DEXA group than SOC group in majority of the visits and the rate at which the flare came back to its preoperative value was much faster in DEXA group (within 4 weeks) than SOC (3 months) i.e. early and better recovery occurred in DEXA group. This suggests that Dexamethasone implant is efficacious in controlling postoperative inflammation in cases of uveitic cataract undergoing phacoemulsification.
In our study, 75% patients in SOC group achieved vision better than or equal to 20/40, which is comparable with the previous studies showing visual acuity outcome better than 20/40 in 67% to 74% cases.25,26 These visual acuity results in our study compare favorably with few other studies, where phacoemulsification was done for uveitic cataract without dexamethasone implant, in which visual acuity better than 20/40 was observed in 36% to 41% cases.27,28 This might be due to the fact that these studies had more number of posterior uveitis cases. In DEXA group, 100% patients achieved vision better than or equal to 20/40 after 6 months of follow up (although 28.57% has vision between 20/30 and 20/40), suggesting that this group has significantly better visual outcome than SOC and that its use results in better and favorable outcome in most of the cases as a result of better inflammation control in early postoperative period and less complications in this group.
CME is considered as one of the commonest cause of postoperative low vision following cataract surgery in cases of uveitic cataract. In our study also 37.5 % patients developed CME in SOC group, which correlates with the incidence of postoperative CME described in literature, ranging from 18 to 56%, in various studies for post cataract surgery in uveitic cataract patients.28,29 Majority of the patients, who developed CME, developed at 6 weeks of postoperative follow up, which may be due to high inflammation in the early postoperative period in this group causing CME. In DEXA group, no patient developed CME. So, we believe that standard of care treatment, which is usually given for control of inflammation in uveitis cases and on which inflammation is controlled preoperatively, is not sufficient to control inflammation postoperatively and additional steroids or immunosuppresive agents are needed for postoperative control. In SOC group, no hike of steroids or additional immunosuppresion was given preoperatively, so there were more inflammation and more chances of CME postoperatively. In DEXA group, a sustained releasing dexamethasone implant released small doses of dexamethasone slowly and steadily thereby controlling postoperative inflammation and also reducing chances of CME. This suggests that dexamethasone implant is efficacious in controlling the postoperative inflammation and there was good postoperative inflammation control in this group.
Usually systemic steroids are given for treating postoperative CME or are given prophylactically by some surgeons to prevent postoperative CME, but giving systemic steroids although effective in reducing inflammation and treating CME in most cases, is associated with lot of side effects and comorbities. So local therapy has always been in demand to overcome this problem and lot of things were also tried and studied like triamcinolone injection,30 introperative fluocinolone implant20 and posterior sub-tenon steroid injections, etc but results were not promising. Our study provides solution for this problem. Intravitreal Dexamethasone implant is a sustained release implant, which releases dexamethasone in very low doses directly into the vitreous cavity very slowly, thereby controlling the inflammation directly at its site and not exposing the whole body to steroids. It has a unique drug delivery system providing longer duration of action.31 Dexamethasone implant has already shown to be effective for recalcitrant macular edema associated with posterior uveitis.24,32
IOP rise (IOP>21 mmHg) occurred in 3 eyes in our study, all of which belonged to the SOC group and occurred on the immediate postoperative day one, which might be due to retained viscoelastic during surgery and was managed with oral acetazolamide and did not require any long term medical or surgical treatment. No patient in DEXA group had raised IOP during 6 months of follow up visits. Hence, Dexamethasone implant is not associated with any IOP rise as occurred in previously used steroid implants like fluocinolone acetonide implant.20 In our study, no patient developed any steroid induced ocular hypertension or glaucoma in either group.
In our study, the SOC group was associated with lot of complications like CME in 37.5% cases, 12.5 % had flare up of inflammation in the early postoperative period (≤6 weeks) and 6.25% had postoperative hypotony. In DEXA group, none had CME and IOP rise and only 7.1% cases had flare up of inflammation postoperatively which occurred at the 3 months follow up visit.
Our study suggests that dexamethasone implant is a safe and effective solution to the problem of postoperative inflammation following cataract surgery in uveitis patients and its use can result in better visual outcomes and early recovery of patients.
Strengths of our study: It is a first study of its kind comparing the efficacy of intraoperative intravitreal injection of dexamethasone implant with standard of care treatment of uveitic cataract, in which inflammation was measured objectively using LFP, thereby removing investigator bias.
Limitation of our study was its small sample size and non documentation of preoperative CME.
Conclusions
Our study shows that, use of intraoperative intravitreal dexamethasone implant while doing phacoemulsification with IOL implantation in cases of uveitis with cataract, results in less postoperative inflammation and faster recovery, better visual outcome, less incidence of CME and minimal adverse effects. So we conclude that, dexamethasone implant is a safe and effective option for preventing and managing the postoperative inflammation in uveitic cataract cases and is also useful in preventing the complications of cataract surgery in uveitic cases.
Conflict of interest and source of funding – Nil
Acknowledgement – None
What was known:
Dexamethasone implant has already shown to be effective for recalcitrant macular edema associated with posterior uveitis but not in uveitic cataract patients undergoing phacoemulsification with IOL implantation
What this paper adds:
Use of intraoperative intravitreal dexamethasone implant during phacoemulsification with IOL implantation in cases of uveitic cataract, results in less postoperative inflammation and faster recovery, better visual outcome, less incidence of CME and minimal adverse effects.
Dexamethasone implant is a safe and effective option for preventing and managing the postoperative inflammation in uveitic cataract cases and is also useful in preventing the complications of cataract surgery in uveitis cases.
References:
- Rao NA. Uveitis in developing countries. Indian J Ophthalmol 2013;61:253-4
- Jones NP. The Manchester Uveitis Clinic: The first 3000 patients, 2: Uveitis Manifestations, Complications, Medical and Surgical Management. Ocul Immunol Inflamm 2014:1-8
- Baheti U, Siddique SS, Foster CS. Cataract surgery in patients with history of uveitis. Saudi J Ophthalmol 2012;26:55-60
- Okhravi N, Lightman SL, Towler HM. Assessment of visual outcome after cataract surgery in patients with uveitis. Ophthalmology 1999;106:710-22
- Foster CS, Fong LP, Singh G. Cataract surgery and intraocular lens implantation in patients with uveitis. Ophthalmology 1989;96:281-8
- Hogan MJ, Kimura SJ, Thygeson P. Signs and symptoms of uveitis. I. Anterior uveitis. Am J Ophthalmol 1959;47:155-70
- Ladas JG, Wheeler NC, Morhun PJ, Rimmer SO, Holland GN. Laser flare-cell photometry: methodology and clinical applications. Surv Ophthalmol 2005;50:27-47
- Tugal-Tutkun I, Herbort CP. Laser flare photometry: a noninvasive, objective, and quantitative method to measure intraocular inflammation. Int Ophthalmol 2010;30:453-64
- Wakefield D, Herbort CP, Tugal-Tutkun I, Zierhut M. Controversies in ocular inflammation and immunology laser flare photometry. Ocul Immunol Inflamm 2010;18:334-40
- Bernasconi O, Papadia M, Herbort CP. Sensitivity of laser flare photometry compared to slit-lamp cell evaluation in monitoring anterior chamber inflammation in uveitis. Int Ophthalmol 2010;30:495-500
- Herbort CP, Guex-Crosier Y, de Ancos E, Pittet N. Use of laser flare photometry to assess and monitor inflammation in uveitis. Ophthalmology 1997;104:64-71
- Guex-Crosier Y, Pittet N, Herbort CP. Evaluation of laser flare-cell photometry in the appraisal and management of intraocular inflammation in uveitis Ophthalmology. 1994;101:728-35
- Tran VT, Guex-Crosier Y, Herbort CP. Effect of cataract surgery with intraocular lens implantation on inflammation in chronic uveitis: a longitudinal laser flare photometry study. Can J Ophthalmol 1998;33:264-9
- Shah SM, Spalton DJ. Changes in anterior chamber flare and cells following cataract surgery. Br J Ophthalmol 1994;78:91-4
- Agrawal R, Murthy S, Ganesh SK, Phaik CS, Sangwan V, Biswas J. Cataract surgery in uveitis. Int J Inflam 2012;2012:548453
- Barton K, Hall AJ, Rosen PH, Cooling RJ, Lightman S. Systemic steroid prophylaxis for cataract surgery in patients with posterior uveitis. Ocul Immunol Inflamm 1994;2:207-16
- Taylor SR, Isa H, Joshi L, Lightman S. New developments in corticosteroid therapy for uveitis. Ophthalmologica 2010;224 Suppl 1:46-53
- Habot-Wilner Z, Sallam A, Pacheco PA, Do HH, McCluskey P, Lightman S. Intravitreal triamcinolone acetonide as adjunctive treatment with systemic therapy for uveitic macular edema. Eur J Ophthalmol 2011;21 Suppl 6:S56-61
- Ferrante P, Ramsey A, Bunce C, Lightman S. Clinical trial to compare efficacy and side-effects of injection of posterior sub-Tenon triamcinolone versus orbital floor methylprednisolone in the management of posterior uveitis. Clin Experiment Ophthalmol 2004;32:563-8
- Chieh JJ, Carlson AN, Jaffe GJ. Combined fluocinolone acetonide intraocular delivery system insertion, phacoemulsification, and intraocular lens implantation for severe uveitis. Am J Ophthalmol. 2008;146:589-94
- Haller JA, Bandello F, Belfort R, et al. Randomized, sham-controlled trial of dexamethasone intravitreal implant in patients with macular edema due to retinal vein occlusion. Ophthalmology. 2010;117:1134-46 e3
- Pleyer U, Klamann M, Laurent TJ, et al. Fast and Successful Management of Intraocular Inflammation with a Single Intravitreal Dexamethasone Implant. Ophthalmologica 2014;232:223-229
- Gupta A, Ram J, Gupta A, Gupta V. Intraoperative dexamethasone implant in uveitis patients with cataract undergoing phacoemulsification. Ocul Immunol Inflamm. 2013;21:462-7
- Kuppermann BD, Blumenkranz MS, Haller JA, et al. Randomized controlled study of an intravitreous dexamethasone drug delivery system in patients with persistent macular edema. Arch Ophthalmol. 2007;125:309-17
- Kawaguchi T, Mochizuki M, Miyata K, Miyata N. Phacoemulsification cataract extraction and intraocular lens implantation in patients with uveitis. J Cataract Refract Surg. 2007;33:305-9
- Mehta S, Linton MM, Kempen JH. Outcomes of cataract surgery in patients with uveitis: a systematic review and meta-analysis. Am J Ophthalmol. 2014;158:676-92 e7
- Estafanous MF, Lowder CY, Meisler DM, Chauhan R. Phacoemulsification cataract extraction and posterior chamber lens implantation in patients with uveitis. Am J Ophthalmol. 2001;131:620-5
- Tranos PG, Wickremasinghe SS, Stangos NT, Topouzis F, Tsinopoulos I, Pavesio CE. Macular edema. Surv Ophthalmol. 2004;49:470-90
- Foster CS, Rashid S. Management of coincident cataract and uveitis. Curr Opin Ophthalmol. 2003;14:1-6
- Dada T, Dhawan M, Garg S, Nair S, Mandal S. Safety and efficacy of intraoperative intravitreal injection of triamcinolone acetonide injection after phacoemulsification in cases of uveitic cataract. J Cataract Refract Surg. 2007;33:1613-8
- Chang-Lin JE, Attar M, Acheampong AA, et al. Pharmacokinetics and pharmacodynamics of a sustained-release dexamethasone intravitreal implant. Invest Ophthalmol Vis Sci. 2011;52:80-6
- Lowder C, Belfort R, Jr., Lightman S, et al. Dexamethasone intravitreal implant for noninfectious intermediate or posterior uveitis. Arch Ophthalmol. 2011;129:545-53
Figures:
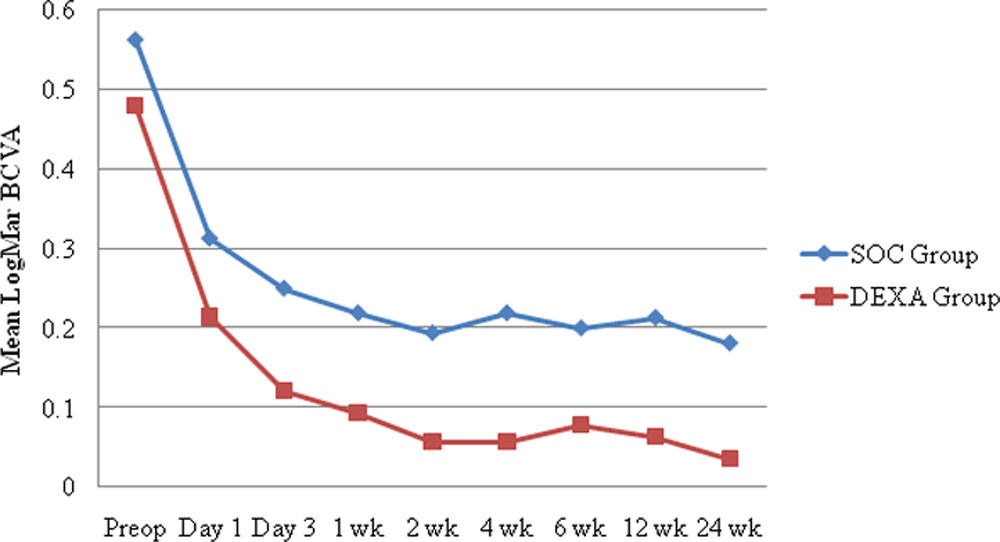
Fig 1: Graph showing trend of mean BCVA from preoperative to various postoperative follow-up visits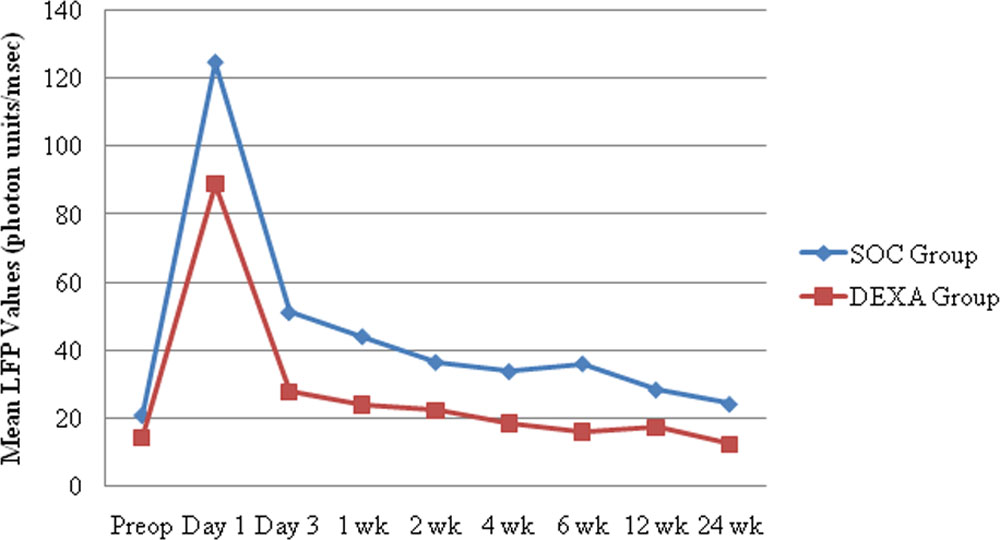
Fig 2: Graph showing trend of flare from preoperative to various postoperative follow-up visits
Tables:
Table 1: Preoperative characteristics of both the groups
| Preoperative characteristics | SOC group | DEXA group | P-Value |
| Logmar BCVA | 0.56±0.21 | 0.48±0.20 | 0.285 |
| IOP (mm of Hg) | 15.5±3.3 | 14.7±3.3 | 0.527 |
| LFP (photon units/msec) | 21.0±14.1 | 14.4±10.6 | 0.163 |
(BCVA- Best Corrected Visual Acuity, IOP- Intraocular Pressure, LFP- Laser Flare Photometry)
Table 2. Postoperative LogMar BCVA at various visits in follow up period.
|
GROUP |
Postoperative Mean LogMar BCVA ± SD | ||||
| 1 week | 1 month | 6 weeks | 3 months | 6 months | |
| SOC group | 0.229±0.225 | 0.219±0.234 | 0.200±0.236 | 0.213±0.257 | 0.181±0.225 |
| DEXA group | 0.093±0.143 | 0.057±0.093 | 0.079±0.089 | 0.064±0.092 | 0.036±0.063 |
| P- value | 0.077 | 0.020 | 0.072 | 0.045 | 0.024 |
(BCVA- Best Corrected Visual Acuity)
Table 3: Postoperative Mean IOP at various visits in follow-up period.
|
Groups |
Mean IOP ± SD (mm of HG) | ||||||
| Day 1 | 1 week | 2 weeks | 4 weeks | 6 weeks | 12 weeks | 24 weeks | |
| SOC group | 18.63±6.96 | 14.00±3.05 | 14.25±3.66 | 14.31±2.62 | 14.56±3.63 | 14.44±3.28 | 15.06±3.31 |
| DEXA group | 18.86±6.73 | 14.29±2.40 | 14.93±3.45 | 15.43±1.74 | 14.07±2.01 | 14.29±2.30 | 13.86±1.95 |
| P-value | 0.927 | 0.780 | 0.607 | 0.155 | 0.657 | 0.886 | 0.244 |
(IOP-Intraocular Pressure)
Table 4. Postoperative Mean LFP readings over the follow-up period.
|
Group |
Mean LFP reading ± SD (photon units/msec) | |||||||
| Day 1 | Day 3 | 1 week | 2 weeks | 4 weeks | 6 weeks | 12 weeks | 24 weeks | |
| SOC group | 124.95±118.05 | 51.25±
41.96 |
44.20±
30.56 |
36.625±30.47 | 33.91±
25.70 |
36.20±
25.56 |
28.53±
20.74 |
24.300±
17.62 |
| DEXA group | 88.91±
61.97 |
27.75±
20.56 |
23.92±
18.67 |
22.11±
17.86 |
18.47±
13.85 |
15.98±
11.68 |
17.18±
17.35 |
12.29±
11.78 |
| P-value | .346 | .047 | .040 | .119 | .048 | .010 | .114 | .035 |
(LFP-Laser Flare Photometry)
Table 5. Mean central macular thickness over the postoperative follow-up period.
|
Group |
Mean CMT (mm) ± SD | ||
| 6 weeks | 12 weeks | 24 weeks | |
| SOC Group | 376.35±151.66 | 336.35±85.73 | 306.50±53.55 |
| DEXA Group | 286.36±34.93 | 289.54±43.38 | 267.81±34.26 |
| P-value | .04 | .09 | .03 |
(CMT- Central macular thickness)
Leave a Comment