
Dr. Seema Kumari, S19287, Dr. Ashok Kumar Meena, Dr. Parmar Gautam Singh
Chemical injuries result in extensive damage to ocular surface and may lead to permanent visual impairment due to persistent epithelial defects,vascularisation, scarring and keratinization.Early intervention includes therapy for removal of necrotic corneal epithelium, re-establishment of adequate limbal vascularity and replenishment of limbal stem cell loss .Limbal stem cell transplantation is currently the most preferred technique to re-establish a normal corneal phenotype for grade III/IV chemical injuries( which classification? ).But this only promotes epithelisation without achieving a tectonically stable cornea. Limbal allograft transplantation has a success rate of 70% to 80% for a mean follow-up of 1 to 2 yearsand 50% for 5 years1. Large diameter anterior lamellar corneal graft with in situ allogenic limbal stem cells is a single step procedure2.It aims to provide a more stable ocular surface and visual rehabilitation simultaneously in severe chemical injuries where anterior stromal layers of cornea are involved and associated corneal thinning is present.It also helps to provide a good tectonic support.
MATERIALS AND METHODS
.Retrospective review of clinical records of 10 eyes of 10 patients with severe chemical injuries (grade IV/VI) was done in the Department of Cornea and Refractive surgeries , Sadguru Netra Chikitsalaya, Chitrakoot,India from 2007-2016. All patients exhibited signs and symptoms consistent with chronic limbal stem cell deficiency: photophobia, ocular discomfort, decreased vision in the presence of corneal vascularization, conjunctivalisation, and chronic inflammation.Preoperative evaluation consisted of Snellen’s visual acuity testing, slit-lamp biomicroscopy that included fluorescein staining for epithelial defects, forniceal status and slit lamp photography (iop? ).Data collected was related to primary outcome measures that included stability of ocular surface in terms of epithelisation, prevention of conjunctivalization, forniceal deepening, clarity of visual axis and BCVA
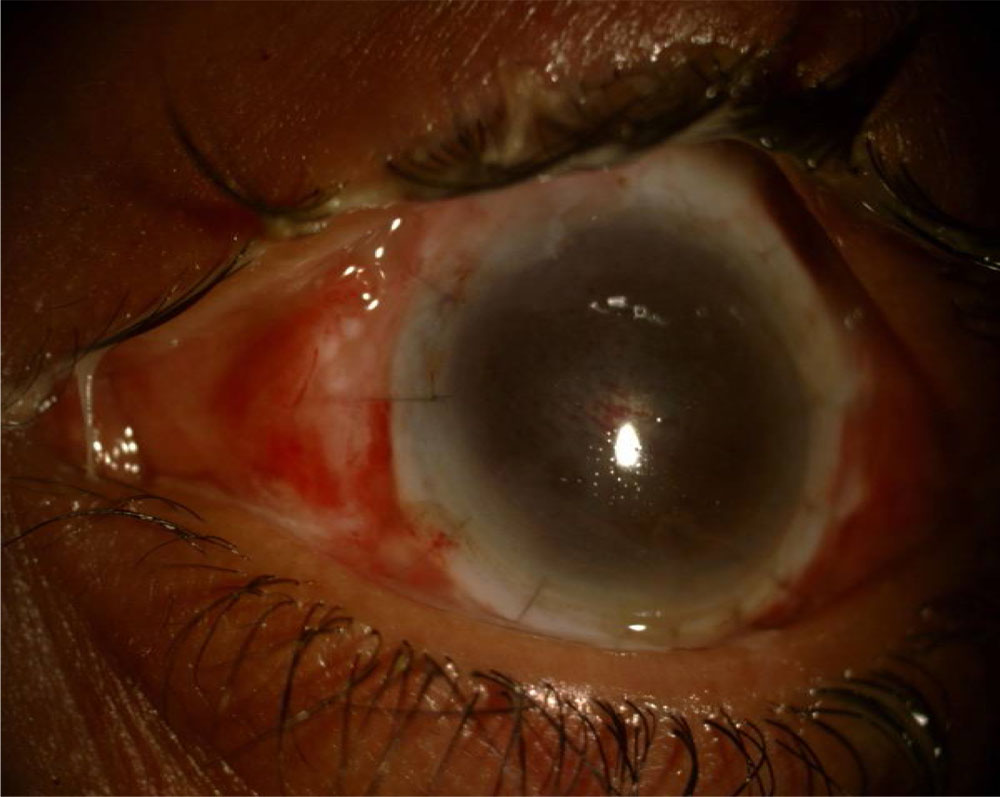
Fig ( not labelled ): Large diameter lamellar grafting with in situ limbal stem cells ,postoperative follow up 6 months
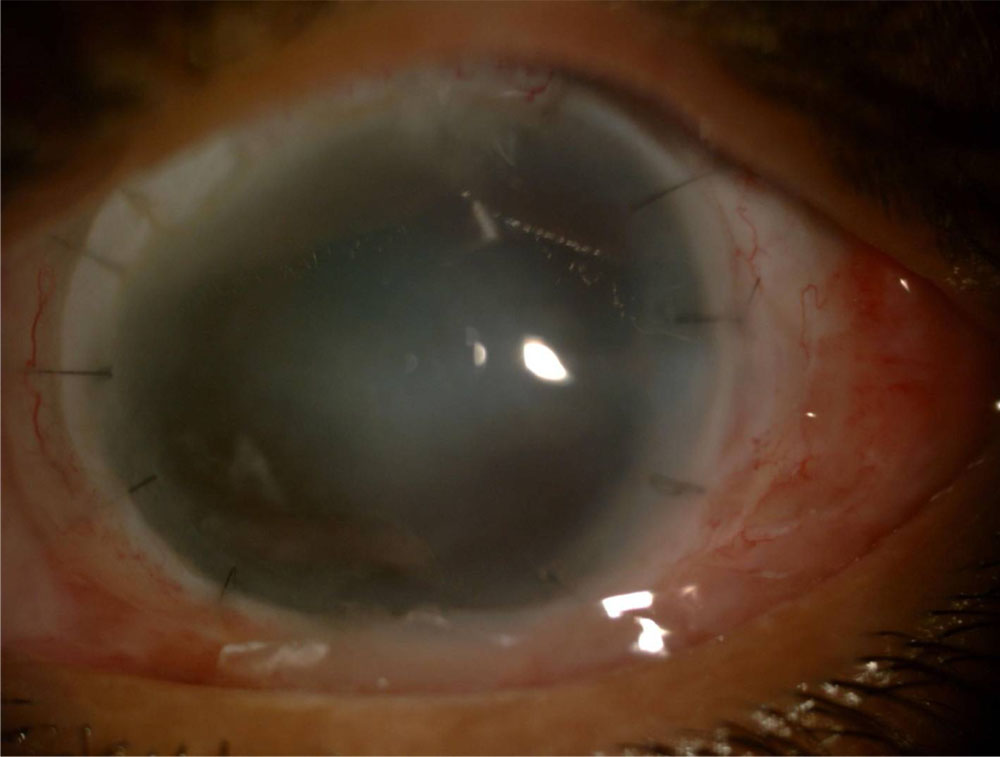
Fig ( not labelled ): Large diameter lamellar corneal graft postoperative
SURGICAL TECHNIQUE
Large diameter anterior lamellar corneal graft with in situ allogenic limbal stem cells was done in all cases. Most patients had already undergone amniotic membrane transplantation .The surgeries were done under both peribulbar and general anaesthesia as most patients were in pediatric age group.After preparation of the patient, 360-degree conjunctival peritomy was performed, and the conjunctiva was retracted posteriorly from the limbus. Any symblepharon present over the cornea was also released simultaneously.
A trephine, 11 mm in diameter was used to remove the host button. The recipient bed was kept moist with the viscoelastic while the donor button was being prepared. McCarey- Kaufman media–preserved corneoscleral tissue was used to harvest donor cornea using a trephine of 12 mm in diameter.The donor tissue consisted of at least 1.5 mm of the limbal frill 360 degrees around the cornea, ensuring the in situ limbal stem cells in the anterior lamellar graft. The lamellar button was dissected manually ensuring a mid stromal dissection .The graft was then sutured to the host with 24 interrupted radial 10-0 monofilament sutures. The conjunctiva was secured to the episclera with 6-0 Vicryl sutures.
Postoperatively, all patients received 1%prednisolone along with moxifloxacin eyedrops four times a day for 1 month, and preservative- free artificial tears every hour. No systemic or topical immunosuppressive agents were given in any of the cases. The topical corticosteroid drops were tapered over 3 to 4 months time, and the artificial tears were tapered after complete epithelialization.The patients were followed up weekly for the first month and monthly thereafter for the next 6 months. subsequent surgeries like amniotic membrane grafting or SLET were done to treat residual conjunctivalisation and vascularization, lid deformities.
RESULTS
Mean age was 12.2 years.There were six females and four males . Mean follow up was 15.9 months. Mean duration between injury and surgery was 10.5±1.2 months. Mean pre-operative and post-operative LogMAR BCVA was 1.77 and 1.5 respectively .Vision improved in seven cases (70%) where as remained unchanged in one case (10%). However, vision deteriorated in two cases(20%). All patients noted improvement in symptoms of watering, pain, and photophobia .Complete epithelisation occurred in 6 out of 10 cases (60%). 4 eyes had persistant epithelial defects which were treated with bandage soft contact lens. Healing occurred with subsequent scar formation .Recurrence of vascularization was seen in four cases (40%).Graft clarity was +2 or better in six cases(60%) where as it was +4 in two cases (20%) and +3 in one case(10%).In one case(10%) graft clarity was+1in which optical penetrating keratoplasty was done later on.
| GRADE | DETAILS |
| 0 | Cornea opaque, pupillary margin not visible
|
| 1 | Cornea hazy, pupillary margin just visible, iris not seen clearly |
| 2 | Cornea hazy, pupil and iris well seen, iris details not well seen
|
| 3 | Cornea slightly hazy, pupil and iris well seen, iris details clear |
| 4 | Cornea clear, pupil and iris well seen, iris details clear |
Table 1. Central Corneal Clarity Grading for LamellarKeratoplasty
| GRADE | DETAILS |
| 0 | Cornea opaque, pupillary margin not visible
|
| 1 | Cornea hazy, pupillary margin just visible, iris not seen clearly |
| 2 | Cornea hazy, pupil and iris well seen, iris details not well seen
|
| 3 | Cornea slightly hazy, pupil and iris well seen, iris details clear |
| 4 | Cornea clear, pupil and iris well seen, iris details clear |
| PATIENT NO. | AGE
(YEARS) |
SEX | DURATION BETWEEN INJURY AND SURGERY(months) | PRE-OP VISUAL ACUITY | POST-OP VISUAL ACUITY | GRADE-CORNEAL CLARITY |
| 1 | 19 | F | 22 | 1.8 | 0.6 | +4 |
| 2 | 16 | F | 09 | 1.7 | 1.5 | +2 |
| 3 | 15 | M | 11 | 1.9 | 1.8 | +2 |
| 4 | 10 | M | 07 | 2.2 | 1.7 | +2 |
| 5 | 03 | F | 10 | 1.8 | 1.8 | +1 |
| 6 | 11 | F | 11 | 1.8 | 0.6 | +4 |
| 7 | 02 | F | 03 | 1.8 | 1.9 | 0 |
| 8 | 10 | M | 06 | 1.8 | 1.5 | +2 |
| 9 | 18 | M | 10 | 1.7 | 1.5 | +2 |
| 10 | 18 | F | 24 | 2.2 | 1.9 | +2 |
.DISCUSSION
Chemical injuries especially alkali burns result in extensive damage to ocular surface due to limbal stem cell deficiency which results in a triad of conjunctivalisation ,vascularisation and chronic inflammation.Amniotic membrane transplantation or Limbal stem cell ttransplantation remains a viable option for ocular surface reconstruction .This procedure is feasible only in cases with superficial scarring and opacification.Moreover long term results of this procedure are not yet available. Rejection following limbal stem cell transplantation is common resulting in recurrence of conjunctivalization .FruchtPery et al studied nine cases of limbal autograft transplantation, of which three required penetrating keratoplasty6 .Generally in such cases a second surgery either a penetrating or a lamellar keratoplasty becomes inevitable for visual rehabilitation3.This is usually delayed by 6 months to 1 year in various studies6,7.In cases of chemical injuries in pediatric population, this visual rehabilitation needs to be done a bit earlier to avoid setting in of amblyopia with an early tectonic support. Large diameter anterior lamellar corneal graft with in situ allogenic limbal stem cells is a single stage surgery in which we target to achieve ocular surface stability and visual rehabilitation at the same time especially in chemical injuries associated with corneal thinning where a deeper corneal scarring and opacification is present.Kenyon and Ttseng performed lamellar or penetrating keratoplasty in 8 of 21 eyes with chronic chemical injury, over a follow-up of 18 months1.
Our study revealed encouraging results taking into view the poor prognosis of chronic chemical injuries.In our study, majority patients were in pediatric age group so early visual rehabilitation was a pre-requisite. There was a significant visual improvement in seven out of ten cases as visual axis was freed of all deep scarring and vascularisation with the help of lamellar corneal graft. One case showed deterioration of visual acuity due to interface scarring9, recurrent vascularisation and recurrent symblepheron formation.( repeated already in results ).This was because of complete epithelisation owing to the initial replenishment of corneal epithelial stem cells from corneoscleral rim of the large size lamellar graft.Sundmacher et al, in a 3-year retrospective case( study/ series?) showed visual deterioration due to presence of residual stromal haze and interface analysisreported failure of 14 of 18 grafts over a follow-up of 22 months attributing it to the presence of severe ocular surface disorders and endothelial immune reactions5.The same authors successfully performed large-diameter lamellar keratoplasty in a case of congenital aniridia.8. Large diameter anterior lamellar corneal graft with in situ allogenic limbal stem cells also aided in an early tectonic supporting thinned corneas in chemical injuries. A thin host bed would make wound closure and astigmatic control difficult in case a future penetrating keratoplasty is required.Our study showed that large-diameter lamellar keratoplasty with in situ allolimbal stem cells is a useful therapeutic option in cases of severe ocular alkali burns.Long-term clinical studies are required to assess and compare the results of large-diameter lamellar keratoplasty with in situ limbal stem cells and limbal stem cell transplantation with a subsequent additional lamellar or penetrating keratoplasty.
CONCLUSION
Large diameter anterior lamellar keratoplasty with in situ limbal stem cells is a reliable singlestep procedure for stabilisation of ocular surface,visual rehabilitation and early tectonic support in chemical injuries.
REFERENCES
- Tseng SC, Pradhasawat P, Barton K, et al. Amniotic membrane transplantation with or without limbal allografts for corneal surface reconstruction in patients with limbal stem cell deficiency. Arch Ophthalmol 1998;116:431– 41
- Sundmacher R, Reinhard T. Homologe lamellare zentrale Limbokeratoplastik bei schwerer Limbusstammzellinsuffizienz. Klin Monatsbl Augenheilkd 1998;213:254 –5
- Thoft RA. Conjunctival transplantation. Arch Ophthalmol 1977;95:1425–7.
- ( not quoted anywhere )5. Sundmacher R, Reinhard T, Althaus C. Homologe zentrale Limbokeratoplastik bei Limbusstammzellscha den. Retrospecktive auf 3 Jahre Erfahrung. Ophthalmologe 1997; 94:897-901
- Frucht-Pery J, Siganos CS, Solomon A, et al. Limbal cell autograft transplantation for severe ocular surface disorders.Graefes Arch Clin Exp Ophthalmol 1998;236:582–7
- Kenyon KR, Tseng SC. Limbal autograft transplantation for ocular surface disorders. Ophthalmology 1989;96:709 –22;discussion 722–3
- Sundmacher R, Reinhard T. Homologe lamellare zentrale Limbokeratoplastik bei schwerer Limbusstammzellinsuffizienz. Klin Monatsbl Augenheilkd 1998;213:254 –5
- 9 Sugita J, Kondo J. Deep lamellar keratoplasty with complete removal of pathological stroma for vision improvement [see comments]. Br J Ophthalmol 1997;81:184 – 8. Comment in:Br J Ophthalmol 1997;81:178 –9, 1998;82:205
( not quoted anywhere )
References 4 and 10 are not quoted anywhere
Leave a Comment