
Dr. Snehal Nikam, S20297, Dr Mahesh Kumar, Dr Nibha Mishra
Introduction:
Epiretinal membrane is a semitransparent membranous tissue that forms at vitreoretinal interface of the macula and cause abnormalities of macular function. Roth and Foss1 postulated that an idiopathic ERM proliferates as retinal tissue derived glial cells escape from mirodefects in ILM that occur during posterior vitreous detachment and migrate to the surface of retina. Another theory attributes the pathogenesis of ERM to the growth and fibrous metaplasia of vitreous cells that remain on the retinal surface after PVD.
The ERM that occurs after retinal reattachment surgery for treating rhegmatogenous retinal detachment is known as macular pucker. It is one of the most common causes of visual loss post RD surgery2,3.The reported prevalence of ERM is 3-8.5% after scleral buckling surgery and 6.1-12.8% after vitrectomy4
ERM is the most common complication of pars plana vitrectomy for retinal detachment. Unlike the idiopathic ERM, in these cases ERM develops due to migration of RPE cells to vitreous cavity through the break, which then settle on the macular surface forming the membrane, The ILM which corresponds to the basement membrane of muller cells is located at the innermost layer of the retina and acts as a scaffold for the development of ERM5-8. Thus, removing the macular ILM during a vitrectomy. Thus, removing the macular ILM during a vitrectomy for rhegmatogenous RD should help to remove any remaining posterior vitreous cells and other precursors of the ERM present on the retinal surface such as the RPE cells and in our study we will propspectivelyanalyse the correlation between ILM peeling and occurrence of a postoperative ERM in patients who will undergo vitrectomy for primary rhegmatogenous RD.
Peeling of the internal limiting membrane of the retina has become a very popular procedure by vitreoretinal surgeons. The combination of new microsurgical instrumentation with the availability of different dyes to stain this thin and transparent membrane has facilitated the performance of internal limiting membrane peeling, reducing the time and trauma associated with this maneuver. Internal limiting membrane peeling has been used to treat variety of retinal pathologies including full thickness macula hole,epiretinal membrane, macular edema,vitremacular traction syndrome, retinal detachment and tersonsyndrome, among others. Although it appears that peeling the internal limiting membrane in these retinal conditions may be associated with better anantomical and visual outcomes following surgery, further evidence through randomised controlled trials is still needed to guide the vitreoretinal surgeon on the appropriate use of this surgical manever10
Martinez –Castillo et al 9 reported that ERM developed in 32.1 % and 57.15 of the patients at 1 month and 3 months respectively after vitrectomy for primary pseudophakic or aphakicrhegmatogenous RD and the removal of ERM was required in 78.5% patients who developed a significant visual loss due to postoperative ERM. Postoperaive ERM tend to occur within 3 months of vitrectomy for rhegmatogenous RD. Odrobina et all11 reported that retinal pucker occurred in 17.8 % of non ILM peeling group but no retinal pucker occurred in ILM peeling group in eyes undergoing vitrectomy for severe proliferative vitreoretinopathy. Nam et al12 reported that no ERM occurred in ILM peeling group whereas ERM occurred in 21.5% of patients who underwent vitrectomy without ILM peeling for primary rhegmatogenous retinal detachment.
Aras et al 13 in their study concluded that ILm peeling at macula for the complicated rhegmatogenous RD prevents epimacular membrane formation without negatively affecting distance visual acuity
In another study conducted by Rajesh C Rao et al 14 in patients undergoing surgery for primary rhegmatogenousRD, 34.4% patients who did not undergo ILM peeling developed macular pucker whereas only 3.3% patients in ILM peeling group developed macular pucker
Aims and objectives: In this study, we assess the change in Best corrected visual acuity after surgery in both the groups. Development of ERM as seen by clinical examination and documented by OpticalCoherence Tomography.
Materials and methods: It is a prospective interventional randomized controlclinical study. This study was conducted at NethradhamaSuperspeciality Eye Hospital,Jayanagar, Bangalore with well equipedVitreo Retina services from September 2015 to December 2016. All male and female patients visiting Vitreoretina department and diagnosed as primary Rhegmatogenous retinal detachment were included in the study. Thirty-five eyes of 35 patients were assessed on indirect ophthalmoscopy. Inclusion criteria was age above 18 years, clear media with primary rhegmatogenous retinal detachment with Proliferative Vitreoretinopathy (PVR) Grade 3 and below. Patients less than 18 years of age, traumatic and complicated RD, Patients with history of uveitis or infectious retinitis, previous ERM or RD surgery, Proliferative vitreoretinopathy(PVR), cryo or laser retinopexy, pan retinal photocoagulation, choroidal detachment or retinal dialysis,tractional retinal detachment were excluded from the study.
After taking detailed written informed consent patient will be examined in detail including determination of best corrected visual acuity (BCVA), slit lamp bio microscopy, indirect ophthalmoscopy,applanationtonometry,biomicroscopicexamination, based on the the inclusion and exclusion criteria, the patients were assigned to two groups – group 1, the ILM peeling and group 2, non ILM peeling group. Their age, BCVA was recorded. For retinal detachment with macular involvement, the location, number and shape of the break (s), extent of RD was recorded. An ERM was defined as a case in which the inner retinal surface of macula is covered by highly reflective membrane on OCT.ERM was classified in 3 grades 1) grade 0 – translucent membrane not associated with any retinal distortion 2) grade 1 – membrane causing an irregular wrinkling of inner retinal surface 3) grade2 – full thickness puckering of macula. All eyes underwentstandard three port pars planavitrectomy (23 gauge), posterior vitreous detachment induction, with or without ILM peeling, fluid air exchange, endolser and intraocular gas or silicon oil tamponade and were scheduled for follow up examinations 1week, 1,3 and 6 months postoperatively. OCT was done 1,3 and 6 months. Effect of treatment was evaluated clinically, by fundus photograph and by OCT. BCVA was measured using Snellen charts and convert to logarithm of minimum angle of resolution (LogMAR`1)
Optical coherence tomography (OCT) is an invaluable tool in the diagnosis and management of different retinal disorders including ERM. It is a non-contact, micron level, high resolution diagnostic method that uses infrared light in the 800 – 840 nm wavelength range to provide real time noninvasive imaging of the retina and is based on the principal of Michaelson interferometry. It is widely used because it provides objective measurement unlike the subjectivity of fundus biomicroscopic assessment. In present study OCT scans were performed with the Optical Coherence Tomograph(Heidelberg SD-OCT)
Surgical Technique
A 23G vitrectomy was performed under peripbulbaranaesthesia. The surgery was performed using a DORC vitrectomy machine (Dutch Ophthalmic Research Center). After taking all the aseptic precautions,360 degree conjunctival peritomy was done.360 degree encirclage was done with 240 silicon band sutured to sclera around 14 mm from the limbus with the help of (4-0) ethibond suture. Sclerotomies were made 4mm, 3.5mm and 3mm from the corneoscleral limbus in phakic, pseudophakic and aphakic eyes respectively in the inferotemporal, superonasal and superotemporal sclera. Infusion cannula was secured in inferotemporal quadrant. After performing the core vitrectomy with vitreous cutter, posterior vitreous detachment was induced with using intravitreal triamcinolone acetate for staining the hyaloid. A wide field non-contact visualization lens (OFFISS lens) was be used for wide peripheral viewing and contact lens was used for visualization and removal ofILM, it was stained with 0.05% brilliant blue dye and then removed using ILM forceps either on detached retina or under PFCL. After fluid gas exchange, endolaserretinopexy was performed and C3F8 gas / silicon oil was injected. Intraocular pressure was checked at the end of the surgery. The surgery was finished after closing the sclerotomy ports and conjunctiva with 6-0 vicryl sutures.
Statistical methods: Data was entered into Microsoft excel data sheet and was analyzed using SPSS 22 version software. Categorical data was represented in the form of Frequencies and proportions. Chi-square test was used as test of significance for qualitative data. Continuous data was represented as mean and standard deviation. Independent t test was used as test of significance to identify the mean difference between two quantitative. p value (Probability that the result is true) of <0.05 was considered as statistically significant after assuming all the rules of statistical tests. Statistical software: MS Excel, SPSS version 22 (IBM SPSS Statistics, Somers NY, USA) was used to analyze data.
Results:
The mean age of the patients was 52.5± 18.93 years in group 1 and 57.2 ± 14.43 years in group 2 (p = 0.89). There were no significant differences between the 2 groups with regard to, number of retinal breaks, macula status, duration from diagnosis to surgery, mean follow-up time.
Figure 1: Gender distribution in two groups
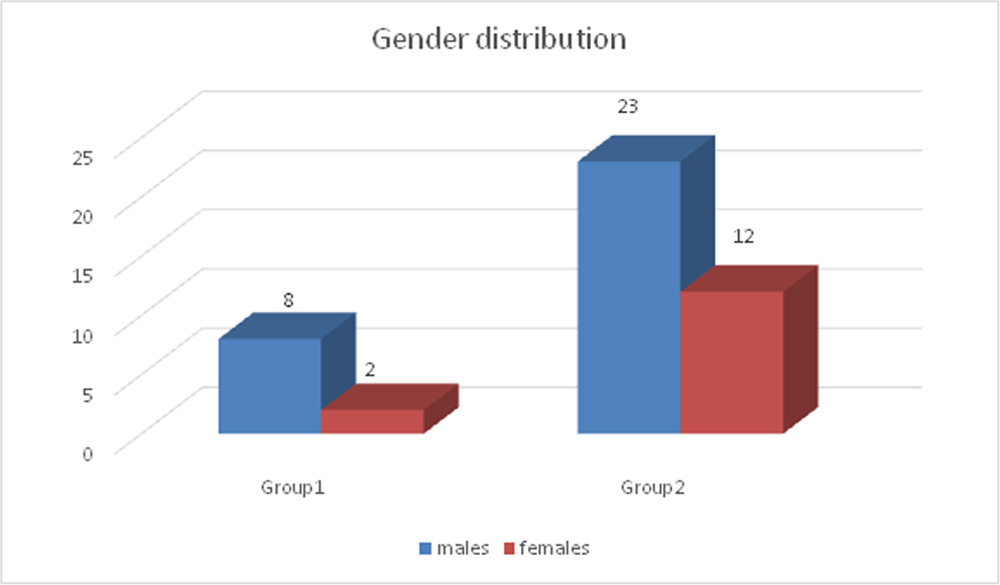
Figure 2: Incidence of ERM in two study groups
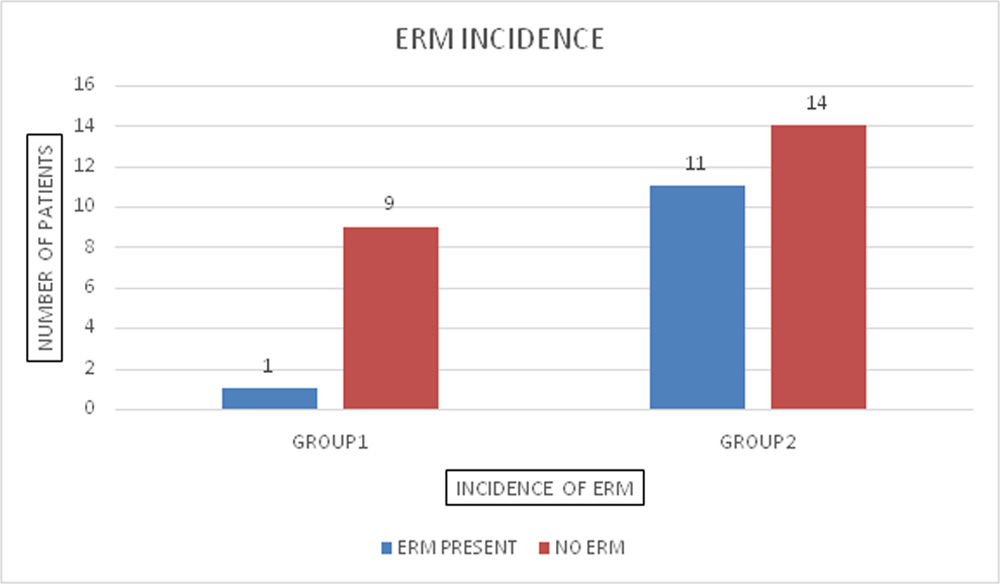
In group 1(ILM peeling group) out of 10 patients only 1 patient developed ERM with macular hole. In group 2 (non ILM peeling group) out of 25 patients 11 patients developed ERM.
Figure 3: Percentage wise ERM distribution in two groups
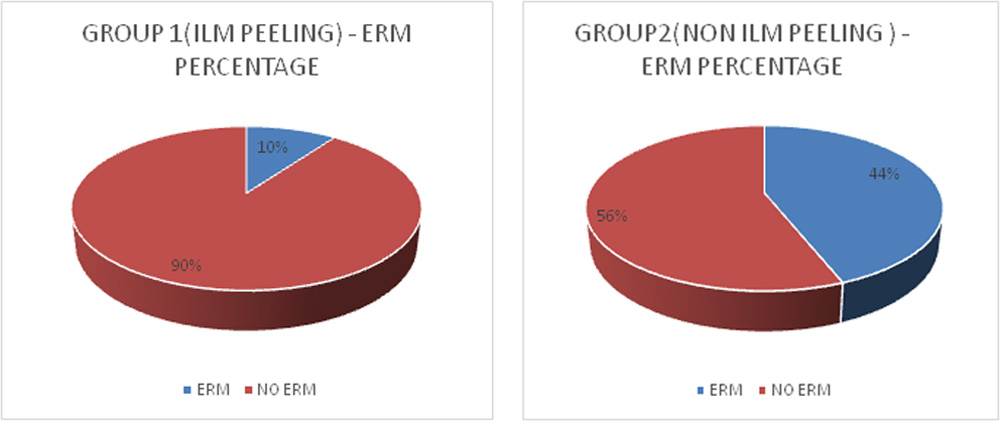
Figure 4: Incidence of ERM according to grading
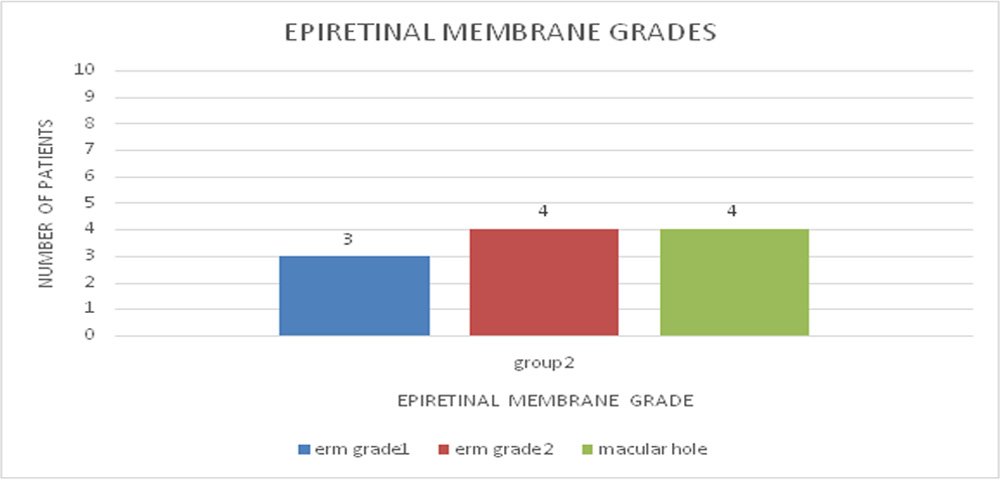
Out of 11 patients in group 2(non ILM peeling),4 patients developed grade 2 ERM which was removed at the time of silicon oil removal, 4 patients developed ERM with macular hole,3 patients developed patients developed ERM grade 1 for which no intervention was done.
Table 1: Comparison of mean preop and post op BCVA in two groups
| Group 1 | Group 2 | P Value | |
| Preop BCVA | 1.20 +/- 1.03 | 1.46 +/- 1.19 | 0.29 |
| Post Op BCVA | 0.32 +/-0.11
|
0.67 +/-0.39
|
0.010 |
| P value of pre and post op BCVA | 0.019 | 0.0004 |
The preoperative mean best corrected visual acuity in group 1 was1.20 +/- 1.03and in group 2 was 1.46 +/-1.19. There was no significant difference between the two (p=0.29). In each group, there was a clinically and statistically significant improvement in visual acuity after RRD repair (group 1 p value = 0.019, group 2 p value =0.0004). The mean BCVA in group 1 was significantly better than mean BCVA in group 2 (p=0.010). One patient is group 1 had amblyopia and in group 2, one patient was amblyopic and one patient had one year old history. These patients failed to show any improvement in visual acuity
Discussion:
An ERM is one of the most common complications of rhegmatogenous RD after a vitrectomy, and ILM may play a role of scaffold on various cells that develops ERM. The ILM is composed of the basement membrane of Muller cells, proteoglycans, and type IV collagen and is an important structure in the formation of the vitreoretinal interface. Astrocytes and myofibroblasts migrate to the surface of the ILM and invade the deep layer, thereby causing an ERM. The ERM that occurs after retinal reattachment surgery for treating rhegmatogenous RD is caused by retinal pigment epithelial cells that migrate to the surface of the posterior pole retina by diffusing into the vitreous cavity through the break or through fibrosis and the proliferation of precursor cells that remain on the retinal surface after the vitrectomy. Therefore, removal of the ILM can remove the ERM precursor cells from the retinal surface. In addition, in cases of severe bullous RD, a mild ERM might not be diagnosed in the fundus examination or with OCT. Therefore, an ERM that was not diagnosed before the surgery would also be removed by removal of the ILM. These provide a rationale for ILM peeling as a method of preventing the occurrence of a postoperative ERM in vitrectomy for rhegmatogenous RD.
In our study, In group 1, out of 10 patients ERM with macular hole developed in 1 patient (10%) whereas in In group 2, Out of 25 patients ERM developed in 11 patients (44%). So, the incidence of ERM was significantly higher in non ILM peeling patients.In group two, 4 patients (16%) developed ERM with macular hole and 4 (16%) patients developed grade 2 ERM. Patients in both these categories required a second surgery with ERM + ILM peeling. Three patients in group two developed grade 1 ERM which didn’t require any surgical intervention
We also studied the effects of the postoperative ERM on visual acuity. Best corrected visual acuity was recordedpostoperatively at 3 months. In patients who underwent surgery for ERM removal BCVA measured just before the ERM removal surgery was used for analysis. As a result, the overall visual acuity was better in the group with ILM peeling than that without ILM peeling. This showed that the visual acuity was affected by the ERM that occurred after primary vitrectomy for rhegmatogenous RD, implying that removal of the ILM results in better visual acuity by preventing the occurrence of a postoperative ERM compared with patients who do not undergo ILM peeling.
In a prospective study of patients who required silicone oil filling and underwent retinectomy during a vitrectomy due to accompanying proliferative vitreoretinopathy upon diagnosis of RD, Odrobina et al reported that retinal pucker occurred in 17.8% of the non-ILM peeling group (33 patients), but no retinal pucker occurred in the ILM peeling group (51 patients). Although there were a few cases with fibrous proliferation in the patients who underwent ILM peeling, its progression was limited to the margin of ILM peeling11. However, our study is meaningful in that it enrolled patients with primary rhegmatogenous RD, who are expected to have a relatively good postoperative prognosis in the case of successful retinal adhesion. In this study, ILM peeling during vitrectomy for rhegmatogenous RD was shown to help to prevention of the formation of a postoperative ERM.
The safety of ILM peeling when there is no macular lesion is controversial. Peeling the internal limiting membrane of the retina has become a very common procedure performed by vitreo-retinal surgeons. The combination of new microsurgical instrumentation with the availability of different dyes to stain this thin and transparent membrane has facilitated the performance of internal limiting membrane peeling, reducing the time and trauma associated with this maneuver.
Conclusion:
In conclusion, ILM peeling during vitrectomy for primary rhegmatogenous RD is useful for preventing postoperative ERM formation and provides a better visual prognosis. However, we have to consider whether ILM peeling for all patients is beneficial. This should be confirmed in a further long-term prospective study with a greater number of patients.
Bibliography:
1.Roth am, Foos RY. Surface wrinkling retinopathy in eyes enucleated at autopsy.Trans Am AcadOphthalmolOtolaryngol 1971;75:1047-1058
2.Lobes LA Jr,BurtonTC.The incidence of macular pucker after retinal reattachment surgery . Am J Ophthalmol1978;85:72-77
3.Wilkinson CP.Visual results following scleral buckilng for retinal detachment patients sparing macula.Retina 1981;1:113-116.
4.Tanenbaum HL,schepensCL,Elzeneiny I et al. Macular pucker following retinal detachment surgery.archophthalmol 1970;83:286-293
5.De bustrosS,ThompsonJT,Michels RG et al. Vitrectomy for idiopathic ERM causing macular pucker.Br J Opthalmol 1988;72:692-695
De bustros,Rice TA, Michels RG at al. Vitrectomy for macular pucker .Use after treatment of retinal tears or retinal detachment. Arch Ophthalmol1988;106:758-760
7.Uemura A,IdetaH,Nagasaki H et al.macular pucker after retinal detachment surgery .Ophthalmic Surg 1992;23:116-119
8.Heo MS Kim HW ,Lee JE et al.The clinical features of macular pucker formation after pars plana vitrectomy for primary rhegmatogenous retinal detachment repair.Korean J Ophthalmol 2012;26:355-361
9.Martinez-castillo V, Boixadera A ,istefanoL,et al Epiretinal membrane after pars plana vitrectomy for primary pseudophakic or aphakicrhegmatogenous retinal detachment.incidence and outcomes .Retina 2012;32:1350-1355
10.Amdelkader ,etal.Internal limiting membrane peeling in vitreoretinal surgery .Surv Ophthalmol.2008;53,368-396.
11.Odrobina D,BednarksiM,Cisiecki S et al.Internal limiting membrane peeling as a prophylaxis of macular pucker formationin eyes undergoing retinectomy for severe proliferative retinopathy
Nam K Y et al.effect of internal limiting membrane peeling on the development of Epiretinal membrane after pars plana vitrectomy for primary rhegmatogenous retinal detachment. Retina 2015;35:880-885
13.Aras C et al.peeling of internal limiting membrane during vitrectomy for complicated retinal detachment repair prevents epiretinal membrane formation.Grafes Arch ClinExpOphthal 2009.247(5):619-23
14.Rajesh c et al, of internal limiting membrane peeling for primary rhegmatogenous retinal detachment repair.Ophthalmology 2013;120:1101-1102
Leave a Comment