
Dr. Durga Priyadarshini, D15392, Dr. Ambika
Abstract :
Aim :To retrospectively analyse and clinicoradiologically correlate atypical optic neuritis patients with optic nerve thickening on MRI brain and orbit . Materials and methods: Retrospective analysis of 22 patients (35 eyes) who presented to a tertiary eye centre between March 2015 and March 2017 was done.Results: In this cohort granulomatous etiology was most common (59.09%) followed by idiopathic (18.18%) and infiltrative (13.63%). MRI Brain and orbit with contrast showed optic nerve enhancement in 20 patients and brain lesions in 9 patients. All patients received systemic steroids.13 patients received anti tuberculosis treatment.88.5 %( 31 eyes) had profound vision loss at presentation and 54.28 %( 19 eyes) had visual recovery ranging from HM to 6/6 at 1 month follow-up. Conclusion: Most common etiology of atypical optic neuritis with optic nerve thickening and enhancement on MRI was granulomatous. Patients with poor response to treatment eventually were found to have infiltrative etiology.
Key words : Atypical optic neuropathy,Optic nerve thickening,Granulomatous optic neuropathy,Infiltrative and idiopathic optic neuropathy.
Introduction :
Optic neuritis is an inflammatory disorder of the optic nerve which can be due to various etiologies, the most common being multiple sclerosis (MS ) in western literature [1] . Other causes include granulomatous infections like tuberculosis, syphilis, Lyme disease or cryptococcal meningitis, viral infections, autoimmune diseases and idiopathic etiology[1-3 ]. The typical neuritis characteristic features include unilateral subacute painful diminished vision [4]. Lack of pain, profound vision loss with no improvement during disease course and bilateral involvement include the atypical features [5 ,6]. Developments which help in understanding the pathophysiology of optic neuritis and further treatment have occurred and magnetic resonance imaging is an essential investigation among them for optic neuropathies especially atypical [7]. Optic nerve thickening and enhancement has been noted in granulomatous optic neuropathies, optic perineuritis, infiltrative, and idiopathic causes [8,9,11]
Materials and Methods:
22 patients who presented to a tertiary care centre between March 2015 and March 2017 with suspected optic neuritis and Magnetic resonance imaging brain showing optic nerve thickening were included and analysed retrospectively. All patients with typical neuritis, traumatic, and compressive optic neuropathy was excluded.
Detailed medical history from all patients was noted with attention to onset, duration and type of vision loss, associated symptoms such as pain, associated neurological and systemic disorders and prior similar history. Comprehensive ophthalmic details such as visual acuity, colour vision with Ishihara pseudo- isochromatic plates, pupillary examination, intraocular pressure, slit-lamp examination , indirect ophthalmoscopy, stereoscopic disc evaluation with 78D/90 D lens and visual field analysis was recorded. All patients had Magnetic resonance imaging with gadolinium enhanced post contrast study .All patients had undergone blood workup for atypical optic neuropathy which included hemogram, Mantoux test ,Sarcoidosis work-up, autoimmune work-up, VDRL, Aquaporin antibody, and chest Xray . 5 patients had undergone HRCT chest and 3 patients had undergone PET scan. 18 patients had CSF analysis. All patients had received systemic steroids and had come for a follow-ups ranging from one month to 6 months.
Results :
Of the 22 patients (35 eyes ) , 11 patients were male (11%) and 11 patients were female (50 %).The mean age of presentation was 47.95 years ( range: 11 to 65 years ).The duration of presentation ranged from 5 days to 120 days (mean duration -36.59 days ).13 patients had bilateral presentation ( 59.1% ) and 9 patients had unilateral presentation ( 40.9% ) [Table 1]. All patients had presented with loss of vision and 14 patients had associated pain (63.64%) .Only 1 patient had presented with redness (scleritis) ,drooping of lids and double vision prior to vision loss, though all were not noted in the same patient. Significant past history noted in our cohort of patient was 3 out of the 22 patients had treated primary malignancy in the past, 1 patient had abdominal tuberculosis and 2 patients had tuberculosis exposure.
31 out of the 35 eyes (88.57 % ) had presented with profound visual loss .4 (18.18 % ) patients had associated ophthalmoplegia. 10 eyes (28.57% ) had presented with retrobulbar neuritis ,11 eyes (31.42 %) had papillitis and 14 eyes (40 % ) had pale discs. 7 out of 22 patients (31.81% ) had associated retinal findings like vessel occlusion, macular exudates and vitritis [Table 1].
MRI Brain and orbit post gadolinium enhanced study was noted to have optic nerve enhancement in 13 patients (59.09%) , optic nerve sheath enhancement in 7 patients (31.81%) and 2 patients had optic nerve signal with associated orbital apex soft tissue (9.09%) .Imaging showed associated chiasmal involvement in 5 patients, orbital apex involvement in 6 patients, extraocular muscle involvement in 2 patients and CNS involvement in 9 patients [Table 2].9 out of22 patients had positive Mantoux test, 2 patients had positive sarcoid workup ,4 patients noted to have positive autoimmune workup and 1 patient had aquaporin antibody positive.CSF analysis was normal in 9 patients (50 % ) and the most common finding noted was elevated glucose and protein level in 5 and 6 patients respectively.1 patient had malignant cells and 1 patient had positive pus cells and gram negative bacilli though culture was negative. All were negative for MTB-PCR.
Based on the clinicoradiological and biochemical grounds the most common etiology among our cohort was granulomatous optic neuropathy, in 13 patients (59.09 %) followed by idiopathic and infiltrative optic neuropathy in 4 (18.18% ) and 3 patients (13.63 %) respectively. One patient had giant cell arteritis and the other neuromyelitis optica spectrum disorder (4.54% each ).
All patients were treated with intravenous methylprednisolone 1gm/day for 5 days followed by oral weekly taper 1mg/Kg/body weight.13 patients received anti tuberculosis cover .1 patient who was diagnosed with NMOSD received immunosuppressant therapy and 1 patient with infiltrative optic neuropathy received intrathecal chemotherapy. Visual outcome at 1month follow up showed improvement by atleast 1 line in 19 eyes (54.28%),no improvement in 7 eyes (20%) and worsening in 6 eyes (17.14%). Recurrence was noted in 1 eye (2.85%).
Discussion :
We included the 22 patients with optic neuropathy and magnetic resonance imaging post contrast showing optic nerve thickening and soft tissue thickening around the optic apparatus .There was no sex predilection noted in our cohort and the mean age of presentation was 47.75 years . Bilateral presentation was noted in 59.1% which was similar to data reported in eastern population [3,11,12] .
All patients had vision loss out of which 31 eyes (88.57%) had presenting visual acuity of 6/60 to no perception of light and 4 eyes (11.42%) had 6/60-6/9. Associated pain on ocular movements were noted in 14 patients ( 63.64% ) which was significantly lower than western population [3,5]. 14 eyes (40 % ) had optic atrophy, 11 eyes (31.42%) had papillitis and 10 eyes(28.57%) had presented with retrobulbar neuritis [Figure 1]. The incidence of optic atrophy was more as we had included patients who presented late in course with poor spontaneous recovery. 7 patients (31.81%) had associated retinal findings in the form of intraocular inflammation in addition to optic neuropathy. Only a minority of the patient gave past history of tuberculosis and exposure (n=13.63% ) and past history of malignancy was noted in 3 patients (13.63%). In general the clinical condition resembled atypical optic neuritis .
On imaging all patients had either optic nerve or optic sheath enhancement [Figure 2] .5 patients (22.72%) had chiasmal enhancement, soft tissue around orbital apex in 6 patients (27.27%) and extra ocular muscle enhancement in 2 patients (9.09%) . Brain involvement was noted in 9 patients (40.9%) among the 9 patients 3 had dural enhancement and 3 patients had infratentorial and pterygopalatine fossa soft tissue. 2 patients had cranial nerve enhancement, 2 patients had medulla and pontine lesion 1 patient with involvement of infundibulum .Majority of the neuroimaging findings were in favor of granulomatous or infiltrative etiology [8,13].
Blood workup though were not confirmatory they were supporting the diagnosis. Erythrocyte sedimentation rate was raised in all with mean ESR being 40 mm at 1 hr. Mantoux was positive in 40.90 %, Angiotensin converting enzyme was raised in 9.1%. Patients with positive supportive blood workup and raised ESR with optic neuropathy with enhancing optic apparatus on imaging was to be presumed granulomatous etiology [14, 15]. PET scan was done in all 3 patients with past history of malignancy and only one among them had optic nerve uptake .In CSF analysis only minority of the patients had raised proteins (6 patients) and the rest had normal analysis (50%) and few had raised glucose (5 patients) and one had malignant cells. All were negative for MTB PCR.
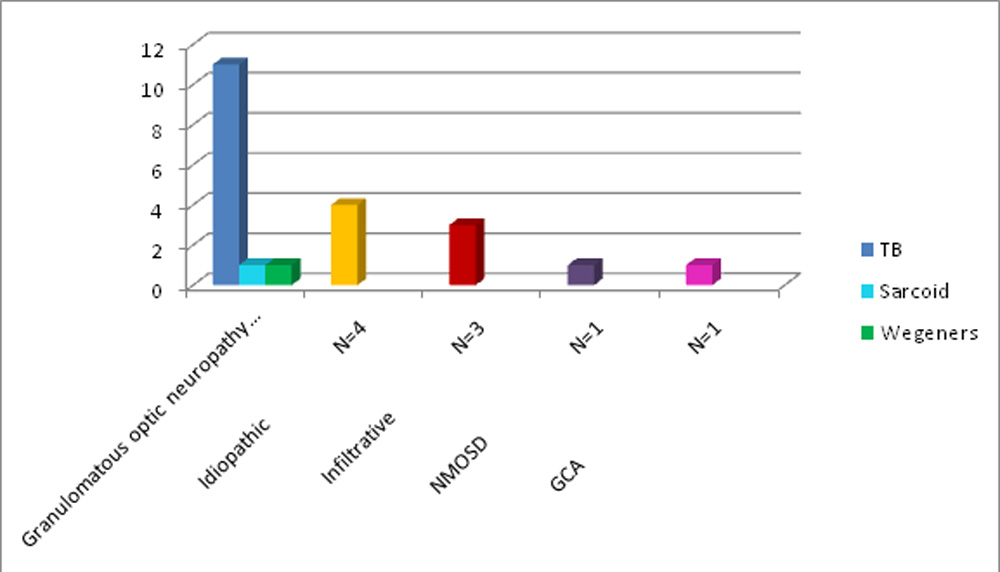
Based on clinicoradiological and supportive blood workup patients were diagnosed and treated. The most common etiology among our cohort was noted to be granulomatous followed by idiopathic and infiltrative etiology.The granulomatous etiology included tuberculous (n=11,50 %) in majority of the patient, sarcoid and Wegener’s granulomatosis in 1 patient each [Figure 3]. All patients had received intravenous followed by oral steroids and 13 patients received anti tuberculosis cover. 1 patient with positive malignant cells in CSF had received intrathecal chemotherapy and 1 patient with suspected NMOSD had received immunosupresants. Visual improvement at 1 month follow-up was noted in 34.37% to 6/18 to 6/9 and 25% had improved to 6/60 to hand movements vision. Worsening was noted in 18.75% (6 eyes ). The 3 patients who had worsening in follow up were suspected NMOSD, infiltrative optic neuropathy out which one was biopsy proven optic nerve germinoma. The 7 eyes who had no improvement where presumed probably secondary to late presentation. One patient who had recurrence in our cohort after 2 months of onset and stopping steroids recovered completely after slow steroids taper with anti tuberculosis cover.
Patients with optic neuropathy with or without previous history of granulomatous pathology systemically, clinically having atypical features and imaging characteristically having enhancing optic apparatus and brain lesions differing from typical optic neuritis should be identified early[16,17] .Delayed identification and treatment might have poor recovery.Treatment warrants slow tapering of steroids watching for relapse. In suspicious cases of tuberculosis especially in endemic country like India anti tuberculosis cover in addition to steroids therapy is essential [18,19]. High index of suspicion of infiltrative pathology is made in patients with slowly progressive vision loss without pain and enhancing optic nerves [20] and modern investigation like PET scan may help in identification of such cases and to avoid invasive procedures .
The study is limited by its small sample size and poor follow up .A larger study cohort and longer follow up will give more details of the association between optic neuropathy and thickened optic nerves on imaging.
Conclusion:
Most common etiology of atypical optic neuritis with optic nerve thickening and enhancement on MRI was granulomatous. Patients with poor response to treatment eventually were found to have infiltrative etiology. It’s essential to identify such cases early as delayed treatment cause poor response for treatment.
References:
- Ebers GC. Optic neuritis and multiple sclerosis .Arch Neurol . 1985; 42-702-704.
- 2.Froozon et al.Acute Demyelinating Optic neuritis. Current Opinion ophthalmology . 2002; 13(6): 375-80.
- Rohit Saxena et al.Clinical Profile and short term outcomes of optic neuritis patients in India .Indian J Ophthalmology 2014 ;62(3):265-67.
- Kale. Optic neuritis as an early sign of multiple sclerosis. Eye and Brain 2016:8 195–202
- Malik a, ahmed m, golnik k.treatment options for atypical optic neuritis .indian j ophthalmol 2014; 62:982-4
- Warren, Flyod A MD.Atyical optic neuritis. Journal of Neuro-Ophthalmology: December 2014 – Volume 34 – Issue 4 – p e12–e13
- .SM Al Eajailat,MV Al Madani Senior. The role of Magnetic Resonance Imaging and Visual Evoked Potential in management of optic neuritis. Pan African Medical Journal. 2014; 17:54.
- DP Kidd ,B J Burton,E M Graham,Gordan T Plant.Optic neuropathy associated with systemic sarcoidosis. Neurol Neuroimmunol Neuroinflamm 2016; 3: e270
- Purvin V, Kawasaki a, Jacobsn DM.Optic perineuritis –Clinical and Radiographic features .Arch Ophthalmol.2001 Sep; 119(9):1299-306.
- . D.Pickuth ET al.Neurosarcoidosis: Evaluation with MRI .Journal of Neuroradiology Nov 2000, Vol 27 (3) pg 185
- Wang JC, Tow S, Aung T, Lim SA, Cullen JF. The presentation, aetiology, management and outcome of optic neuritis in an Asian population.Clin Experiment Ophthalmol.2001; 29:312–5.
- Lim S A, Goh K Y, Tow S, Fu E, Wong T Y, Seah A, Tan C, Cullen J F. Optic neuritis in Singapore. Singapore Med J.2
- ..fj lexa ,ri grossman . mr of sarcoidosis in the head and spine: spectrum of manifestations and radiographic response to steroid therapy. american journal of neuroradiology may 1994, 15 (5) 973-982.
- update. surv ophthalmol 52:561–587.\
- . arsava em, uluc¸ k, kansu t, et al. granulomatous hypophysitis and bilateral optic neuropathy. j neuroophthalmol 2001;21(1):34–6.
- .krohel gb,charles h,smith rs.granulomatous optic neuropathy .arch ophthalmol.1981 jun;99(6):1053-5.
- .ej davis,sr rathinam,aa okada et al.clinical spectrum of tuberculous optic neuropathy .j ophthal inflamm infect.2012 dec;2(4) :183-9.
- gupta v, gupta a, rao na (2007) intraocular tuberculosis—anforam gala.magnetic resonance imaging of optic nerve.indian j of radiol imaging.2015 oct –dec;25(4) :421-38.ali, raghibi & hazabbah, wan & wan hitam, wan hazabbah & azmi, raja & noor, mohd & zunaina, embong. optic perineuritis secondary to tuberculosis: a rare case presentation. asian pacific journal of tropical biomedicine.feb 2012;2(2):1206-1208.
- voss e ,raab p, trebst c,stangel mclinical approach to optic neuritis: pitfalls, red flags and differential diagnosis. ther adv neurol disord. 2011 mar;4(2):123-34.
Table 1 :Demographics and Clinical Characteristics ,N=22 patients (35 eyes)
| Characteristics | Data |
| Mean age of Presentation
Range |
47.95 years
11-65 years |
| Female :Male | 1:1 |
| Laterality
Bilateral Unilateral |
59.1% 40.9% |
| Duration of presentation (Range) | 5-120 days |
| Vision loss | 100% |
| Pain | 63.64% |
| Disc appearance
Papilitis Retrobulbar neuritis Optic atrophy |
31.42% 28.57% 40% |
| Associations
Intraocular inflammation Ophthalmoplegia |
31.81% 18.18% |
Table 2: Imaging findings noted, N=22 patients
| Characteristics-MRI post contrast study | Data |
| Optic nerve enhancement | 59.09% |
| Optic nerve sheath enhancement | 31.81% |
| Optic nerve signal with orbital apex soft tissue | 9.09% |
| Associations -Ophthalmic
Chiasmal involvement Orbital apex Extraocular muscle |
22.72% 27.27% 9.09% |
| Associations-CNS
Dural involvement Pterygopalatine and Infratentorial fossa Crania nerve Midbrain and pons Infundibulum |
13.63% 13.63% 9.09% 9.09% 4.54% |
Figure 1: Disc appearance in our cohort
Retrobulbar neuritis Optictrophy Papillitis 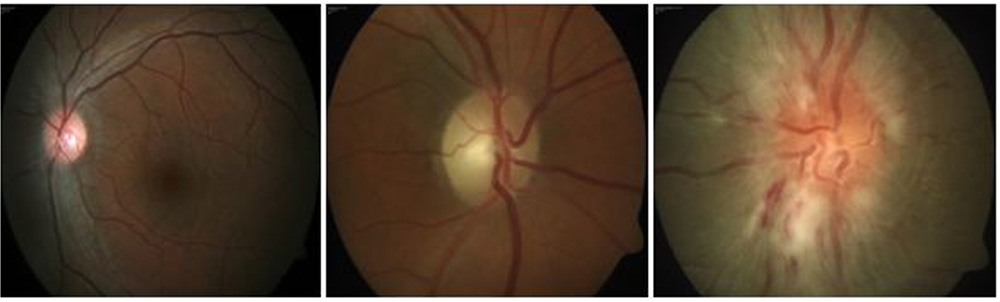
Figure 2 : A) MRI post contrast study axial section showing right optic nerve sheath enhancement.B)Coronal section showing chiasmal enhancement.C)Coronal section showing bilateral optic nerve and sheath enhancement with perioptic haziness. 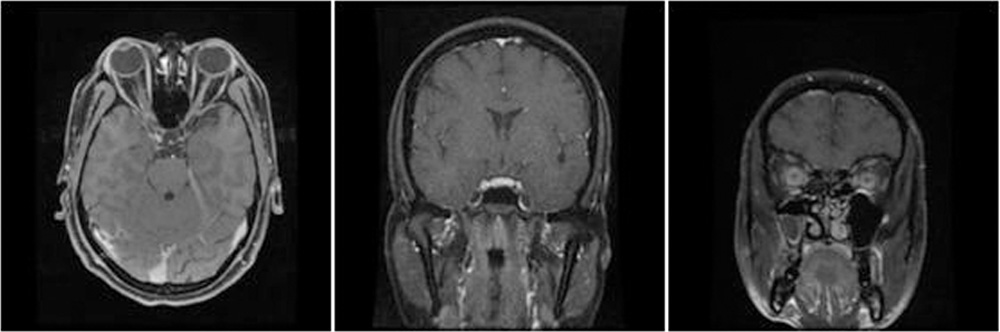
Figure 3 : Etiology of optic neuropathy with optic nerve enhancement ,N=no of patients.
Leave a Comment