
Dr. Gaurav Gupta, G19315, Dr.Sushmita Kaushik, Dr. Pandav Surinder Singh, Dr.Surishti Raj
Abstract:
Purpose: to study the outcome of glaucoma drainage devices (GDD) in post penetrating keratoplasty glaucoma (PPKG) and comparing efficacy of Ahmed glaucoma valve (AGV) with Aurolab aqueous drainage implant (AADI)
Methods: retrospectively, 56 patients who underwent GDD for PPKG and had minimum followup of 6 months, were analysed and type of GDD used, Intraocular pressure (IOP), Visual acuity (VA), graft clarity and complications were studied
Results: preoperatively, mean IOP was 27.80±11.74. 76.78% were on ≥3 topical and 96.43% were on oral antiglaucoma. After GDD, significant reduction of IOP noted at postoperative 6, 12, 24 weeks(p<0.001) and last followup (p<0.001). Mean followup duration was 23.46±29.10 months. Mean IOP on last followup was 13.89±7.23. No significant difference found in final mean IOP and VA between AGV and AADI
Conclusion: GDD results in good IOP control in PPKG. AGV and AADI are equally effective, so AADI being cheaper can be cost effective solution to PPKG
Keywords: Secondary Glaucoma; Ahmed Glaucoma Valved Implant; Aurolab aqueous drainage implant;
INTRODUCTION
Post penetrating keratoplasty glaucoma terminology signifies an elevated intraocular pressure (IOP) greater than 21 mmHg, after penetrating keratoplasty (PKP), with or without associated visual field loss or optic nerve head changes1. Exact PKKG definitions used in the literature could be classified in to three subgroups: I, ocular hypertension (>21mmHg) after PK; II, I plus>4 weeks medical treatment required; III, II plus treatment escalation among patients with preexisting glaucoma. The incidence varied according to different definitions. The highest incidence value was found when only studies using Goldman tonometer were included (22.5%), while the lowest incidence was found when a strict definition was used and steroid-induced PPKG was excluded (12.1%)2. Aphakic and pseudophakic bullous keratopathy, anterior mesenchymal dysgenesis, irido-corneal-endothelial syndrome, pre-existing glaucoma, perforated corneal ulcer, adherent leucoma, previous PK, posttraumatic cases, combined PK and intracapsular cataract extraction, anterior chamber intraocular lenses, presence of vitreous, and performance of an anterior vitrectomy during PK are important risk factors for glaucoma in patients who are undergoing PK3-10. Pathophysiology of post-PK glaucoma is multifactorial and may be related to distortion of the angle with collapse of the trabecular meshwork, suturing technique, post-operative inflammation, use of corticosteroids, PAS formation and pre-existing glaucoma.11
Since surgical management of glaucoma after PKP is still controversial so administration of therapeutics is the initially preferred method of treatment. Trabeculectomy (TRAB) and the implantation of a glaucoma drainage device such as Ahmed glaucoma valve (AGV) are two commonly performed procedures in such patients12. There have been studies comparing the clinical outcomes of Ahmed glaucoma valve in post-penetrating-keratoplasty glaucoma1, trabeculectomy vs. Ahmed glaucoma valve implantation in patients with penetrating keratoplasty13. Another study states that early Ahmed Glaucoma Valve implantation after penetrating keratoplasty leads to better outcomes in an asian population with preexisting glaucoma14. L. Budenz et al studied the five year treatment outcomes in the Ahmed Baerveldt comparison study. There has been no study to compare the outcome of different glaucoma drainage devices (GDD) in post penetrating keratoplasty. The aim of our study is to study the outcome of glaucoma drainage devices (GDD) in post penetrating keratoplasty glaucoma (PPKG) and comparing efficacy of Ahmed glaucoma valve (AGV) with Aurolab aqueous drainage implant (AADI)
METHODS
Retrospectively, 57 eyes of 55patients who underwent GDD for PPKG (post penetrating keratoplasty glaucoma) and had minimum followup of 6 months were analyzed.Parameters studied were age, sex, side(right or left), corneal graft clarity at the time of surgery, duration between the keratoplasty and glaucoma surgery, no of antiglaucoma drugs(topical and oral) before surgery, pre-op visual acuity and intraocular pressure, type of GDD. We measured post-op visual acuity and intraocular pressure on day 1, 1week, 4 week, 6 weeks, 3 months, 6 months. To study of the success of the GDD implants we measured number of drugs at 6 weeks, 3 months and 6 months. The success of GDD was classified as success (IOP<21 with or without one topical antiglaucoma drug), partial success (IOP<21 with two topical antiglaucoma drugs), failure(IOP> 21 with or without antiglaucoma medication. IOP<21 with more than two antiglaucoma medication or oral medication even without topical antiglaucoma medication) Statistical analysis of the data was conducted to study the outcome of GDD in these patients and compare the efficacy of different type of GDD. Statistically we used the T tests and Chi Square tests to compare the outcomes of different GDDs in our study.
RESULTS
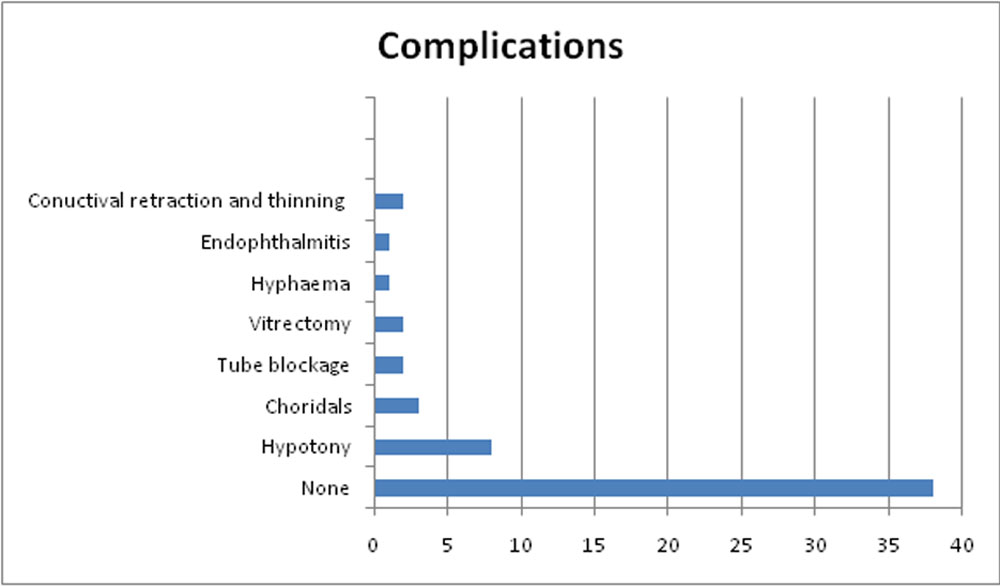
Descriptive analysis of the data showed age group of patients ranged from minimum 3 years to maximum 84 years with mean of 51.12 years with standard deviation of 19.86 years. Out of 57 eyes there were 11(19.3%) eyes of females and 46(80.7%) eyes of males while 35(61.4%) right eye and 22(38.6%) left eyes got operated on left eye. While looking into the graft clarity at the time of surgery 21(36.8%) eyes had clear graft, 14(24.6%) had corneal edema, 2(3.5%) had graft rejections, 1(1.8%) had vascularized graft and no data was available for 19 eyes. While looking into the anti-glaucoma drugs these patients were before surgery we found that maximum number of eyes 22(38.6%) were on four topical drugs, 21(36.8%) were on three topical drugs, 8(14%) were on 2 topical drugs, 4(7%) were on 1 topical drug, 1(1.8%) was on no drug. The topical drugs taken into considerations were beta-blockers, carbonic anhydrase inhibitors, alpha agonists, prostaglandins, mitotic. Besides the topical some patients were on oral drugs (oral glycerol, carbonic anhydrase inhibitors)also. Data analysis shows that before the surgery of 40 eyes (70.2%) patients were on single oral drug acetazolamide 250 mg tds while for 7 eyes (12.3%) patients were on 2 oral medication acetazolamide 250 mg tds and syrup glycerol 6 tea spoons tds. Only while operating 6 eyes(10.5%) patients were on cap Ioparsr while no data was available for 4 patients Two types of glaucoma drainage devices were used in our study Ahmed Glaucoma Valve and Aurolab Artificial Drainage Implant. Out of 57 eye 19(33.3%) had AADI while 38(66.7%) had AGV. We measured post-op visual acuity and intraocular pressure on day 1, 1week, 4 week, 6 weeks, 3 months, 6 months. We observed that after 6 months out of 55 eyes, 21(36.8%) went off drugs, 14(24.6%) were on one topical drug, 15(26.3%) were on two topical drugs, 4(7%) were on three topical drugs, 1(1.8%) was on four topical drugs, no data was available for 2 patients and only 1 patient remained on oral medication.Out of the 57 eyes that underwent GDD(Glaucoma Drainage Device) no complications were reported in 38 eyes while 8 eyes developed hypotony out of which choroidals were reported in 5 eyes, 2 tube blockage, 1 conjunctival retraction, 1 conjunctival thinning over the scleral patch, 1 hyphaema, 1 recurrent endophthalmitis. Some of the additional information we able to retrieve was that 2 patients underwent anterior vitrectomy in follow up,graft cleared in 6 patients which were edematous before the surgery while 2 patients developed graft failure and 1 patient was allergic to the topical drugs.
Table 1: Percentage of patients on topical drugs
| Topicals | Before surgery | 6 months FU |
| 0 | 1.8 | 36.8 |
| 1 | 7 | 24.6 |
| 2 | 8 | 26.3 |
| 3 | 21 | 7 |
| 4 | 41.1 | 1.8 |
| Missing | 1 | 3.5 |
Table 2: Success rate at 6 months
| Full success(IOP<21 off medications) | 21 |
| Partial success(IOP<21 with one or two topical medications) | 27 |
| Failure
(IOP< 21 with three or more topical medications) (IOP > with or without medications) (Oral medication irrespective of the IOP) |
9 |
Figure 1: Various complications which occurred after the surgery
AADI VS AGV
We further studied the comparison of AADI VS AGV in our study in these patients. As we described above out of 57 eyes 19(33.3%) underwent AADI while 38 (66.7%) underwent AGV implant. The patients who underwent AADI implant were comparatively on younger side with mean age 40.16 year (CI 32.27- 48.04) while the patients who underwent AGV had mean age 56.61 years (50.25- 62.96). The mean duration between the OPK and GDD was 15.32 months (CI 7.78- 22.85) in AADI vs 32.29 months (CI 15.07-49.51) in AGV. The mean no of topical drugs in AADI before the surgery were 3.37(CI 3.0 – 3.74) while in AGV were 2.95 (CI 2.58- 3.31). Mean no of oral drugs in AADI before surgery were 1.26(CI 1.05-1.48) vs 0.95(CI 0.82- 1.08) in AGV. No of drugs after 6 months in AADI is 1.17(1.69-65) while in AGV is 1.05(1.41-0.69)
Table 3: Intra-ocular pressure (in mmHg)comparison between AGV and AADI
| AADI | AGV | |
| Pre –op IOP (in mmHg) | 28.63 | 30.0 |
| 6 weeks (in mmHg) | 12.89 | 15.42 |
| 3 months (in mmHg) | 15.53 | 15.47 |
| 6 months (in mmHg) | 12.11 | 14.95 |
Figure 2: Trend of Intraocular pressure control in 2 groups
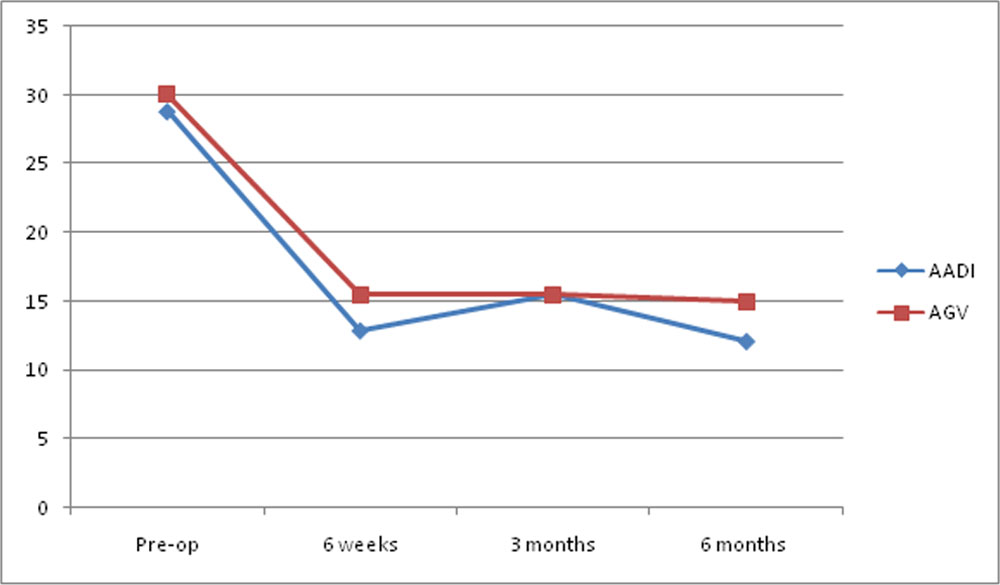
Figure 3: Number of topical drugs needed in 2 groups
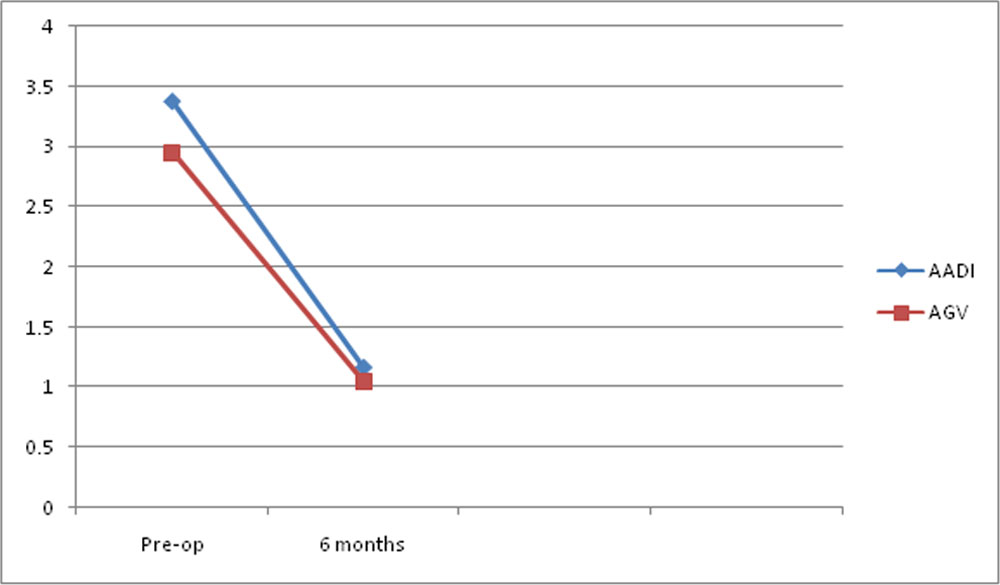
Figure 4: Comparison of visual outcome among 2 groups
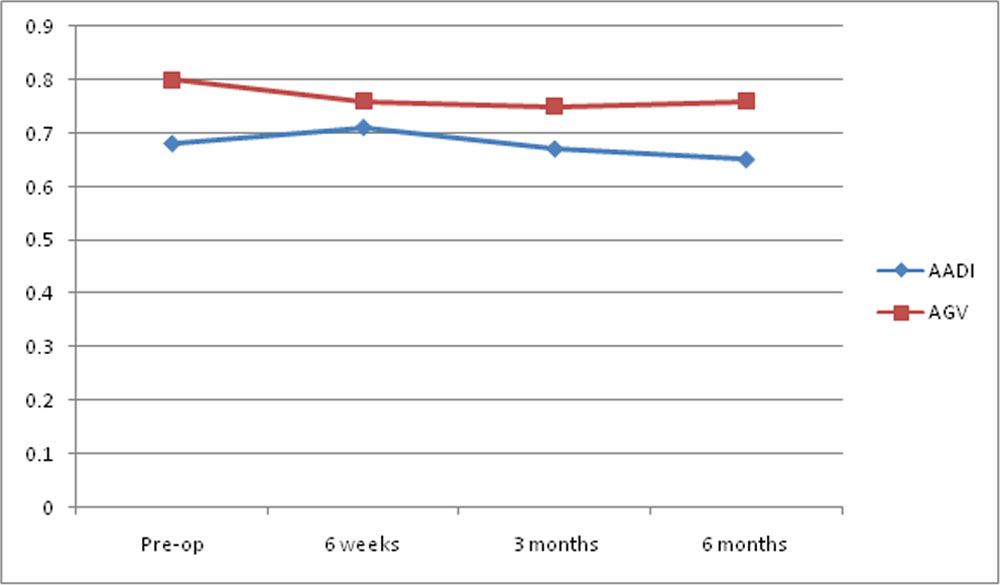
Table 4: Success at 6 months
| AADI | AGV | |
| Full success( IOP<21 off medications) | 6 | 15 |
| Partial success(IOP<21 with one or two topical medications) | 10 | 17 |
| Failure
(IOP< 21 with three or more topical medications) (IOP > with or without medications) (Oral medication irrespective of the IOP) |
3 | 6 |
| Percentage success( full and partial) | 84.21 | 84.21 |
Vision
| Vision | AADI | AGV |
| Pre-op | 0.68 | 0.80 |
| 6 weeks | 0.71 | 0.76 |
| 3 months | 0.67 | 0.75 |
| 6 months | 0.65 | 0.76 |
DISCUSSION
Uncontrolled glaucoma is one of the most significant causes of graft failure and visual acuity loss. Thus, glaucoma must be treated aggressively. If treatment with topical antiglaucoma medications is not reaching the target IOP, surgical treatment is required. The best surgical method for the treatment of glaucoma in patients with penetrating surgery has not been clearly defined. Argon laser trabeculoplasty, TRAB, implantation of glaucoma drainage devices, and cyclodestructive procedures are the currently available surgical treatments. Argon laser trabeculoplasty is limited totreatment of moderate glaucoma, and cyclodestructive procedures are used when other surgical interventions have failed. Therefore, TRAB and implantation of glaucoma drainage devices are the most commonly performed surgical procedures for treatment of postPKP glaucoma 16,17
Though the use of GDDs for controlling refractory glaucoma is well known; its use in post-PKPG glaucoma is scanty18-28.Kirkness was the first to report the use of GDDs in PKPG18. Subsequently, it was advocated that GDDs can also be implanted either before/simultaneously with PKP (if expecting post-PKPG).Anita Panda et all discussed the role of the AGV in management of the pot PKg glaucoma
Different authors have used altered success criteria with varied results.29,30-32 Romaniuk29 found that AGV successfully (IOP <21 mmHg) controlled post-PKPG in 73.5% (13/17) eyes in 1 year. Wilson et al. [23,24] defined success as 5 <IOP <21 mmHg with no need for further glaucoma surgery, and no loss of light perception, and found the probability of success to be 87.9% at months 11–13, 80.5% at months 20–24, 73.2% at months 25–30, and 69.8% at months 41–52 for AGV. The absolute success rate was defined as IOP less than 21 mm of Hg without any medication while qualified success was defined as IOP less than 21 mm of Hg with antiglaucoma medication or with additional surgical maneuver. In Anita Pnadaet all the absolute success rate was 11/20 (55%) and the qualified success rate was 6/20 (30%); the total was 17/20 (85%) after AGV. The qualified success rate was achieved with antiglaucoma medication in three patients; twopatients qualified with tube repositioning and another qualified with anterior vitrectomy. Furthermore, we also noted that the mean number of medications used dropped from 2.92 ± 0.49 to 0.39 ± 0.65 after AGV implantation.
The incidence of graft rejection following AGV is a serious issue and previous studies have reported incidence between 15% and 41%.35,36 The mode of action toward the causation of rejection as put forward by Kirkness was the presence of a tidal flow of cells in and out of the tube located in the AC that may allow aqueous to come into contact with circulating lymphocytes, through the drainage tube, and that the tube may also allow the retrograde passage of inflammatory cells into the AC, increasing the risk of graft rejection. 35The other mode of occurrence as hypothesized could be due to an alteration of the blood-ocular barrier caused by the GDD.36We encountered graft rejection only in one eye in our series that had uncontrolled IOP, which however could be managed with high-dose intravenous pulse steroids, and the grafts remained clear. The frequency of graft failure following GDDs in post-PKPG was reported to be 44%.37This was attributed to corneal endothelial trauma during GDD implantation which is more relevant to post-PKPG eye
Alvarenga et al. in 2004 reported their experience on the long-term follow-up of GDD and commented that the frequency of graft failure may increase following GDDs.33The etiology of failure as suggested by them could be multifactorial, which includes preexisting underlying chronic inflammation, extensive PAS, multiple previous surgeries, and poor endothelial cell count drainage tube per se which may provide a conduit for the retrograde passage of inflammatory cells into the AC.33 We encountered one graft failure which was attributed to tube touch and accentuated by the second surgical repair for its adjustment.
There was no significant change in the BCVA at the final follow-up. Most of the patients had poor vision (<hand movement close to face) initially and the vision dropped further slightly. The findings also corroborate well with those of the literature. The postoperative complication as encountered in our series was AGV in tube blockage with vitreous resulting in a high IOP in one patient. The eye was subjected to anterior vitrectomy and the IOP was controlled without medications. Bleb needling was needed in one patient with an encapsulated AGV plate. Other complications such as, graft infection occurred in one patient and was managed with concentrated antibiotics and tarsorrhaphy in a similar manner.
In summary, this is the first report from India Anita Panda et all on the use of AGV for post-PKPG and we can conclude that implanting AGV is a viable option for controlling IOP for 6 months in post-PKPG34In our study the we studied the effect of the glaucoma drainage devices in the post opk patients. Our patients have minimum follow up of atleast 6 months after the GDD surgery.
Glaucoma drainage devices are studied to find out for assessing their safety and cost effective solutions.
REFERENCES
- Anita Panda, Vadivelu Jaya Prakash, Tanuj Dada, Anoop Kishore Gupta, SudarshanKhokhar, and MurugesanVanathi. Ahmed glaucoma valve in post-penetrating-keratoplasty glaucoma: A critically evaluated prospective clinical study. Indian J Ophthalmol. 2011 May-Jun; 59(3): 185–189.
- Clinical approach to corneal transplantation. In AAO Basic and Clinical Science Course. Section 8; 2005–2006: 425-446
- Foulks GN (1987) Glaucoma associated with penetrating keratoplasty. Ophthalmology 94(7):871–874
- Wilson SE, Kaufman HE (1990) Graft failure after penetrating keratoplasty. SurvOphthalmol 34(5):325–356
- Irvine AR, Kaufman HE (1969) Intraocular pressure following penetrating keratoplasty. Am J Ophthalmol 68(5):835–844
- Goldberg DB, Schanzlin DJ, Brown SI (1981) Incidence of increased intraocular pressure after keratoplasty. Am J Ophthalmol 92(3):372–377
- Karesh JW, Nirankari VS (1983) Factors associated with glaucoma after penetrating keratoplasty. Am J Ophthalmol 96(2):160–164
- Chien AM, Schmidt CM, Cohen EJ, Rajpal RK, Sperber LT, Rapuano CJ, Moster M, Smith M, Laibson PR (1993) Glaucoma in the immediate postoperative period after penetrating keratoplasty. Am J Ophthalmol 115(6):711–714
- Kirkness CM, Moshegoy C (1988) Post-keratoplasty glaucoma. Eye 2(Suppl):19–26
- Bryd S, Tayeri T (1999) Glaucoma associated with penetrating keratoplasty. ClinOphthalmol 39:17–28
- Tanuj Dada, MD, Anand Aggarwal, MD, DNB, KB Minudath, MD, M Vanathi, MD, Sunil Choudhary, MD, DNB, Viney Gupta, MD, RamanjitSihota, MD, FRCS, and Anita Panda, MD, FRCS. Post-penetrating keratoplasty glaucoma. Indian J Ophthalmol. 2008 Jul-Aug; 56(4): 269–277.
- Wu S, Xu J (2017) Incidenceand risk factors for post-penetrating keratoplasty glaucoma: A systematic review and meta-analysis. PLoS ONE 12(4): e0176261.https://doi.org/10.1371/journal. pone.0176261
- Mehmet OrcunAkdemir .Banu Torun Acar .FuruzanKokturk .SuphiAcar. Clinical outcomes of trabeculectomy vs. Ahmed glaucoma valve implantation in patients with penetrating keratoplasty. IntOphthalmol DOI 10.1007/s10792-015-0160-9
- Tai M-C, Chen Y-H, Cheng J-H, Liang C-M, Chen J-T, et al. (2012) Early Ahmed Glaucoma Valve Implantation after Penetrating Keratoplasty Leads to Better Outcomes in an Asian Population with Preexisting Glaucoma. PLoS ONE 7(5): e37867. doi:10.1371/journal.pone.003786
- Budenz DL1, Barton K2, Gedde SJ3, Feuer WJ3, Schiffman J3, Costa VP4, Godfrey DG5, Buys YM6; Ahmed Baerveldt Comparison Study Group. Five-year treatment outcomes in the Ahmed Baerveldt comparison study. Ophthalmology. 2015 Feb;122(2):308-16. doi: 10.1016/j.ophtha.2014.08.043. Epub 2014 Oct 17
- Ishioka M, Shimazaki J, Yamagami J et al (2000) Trabeculectomy with mitomycin C for post-keratoplasty glaucoma. Br J Ophthalmol 84:714–717
- Kornmann HL, Gedde SJ (2015) Glaucoma management after corneal transplantation surgeries. CurrOpinOphthalmol. doi:10.1097/ICU.0000000000000237
- Kirkness CM, Ling Y, Rice NS. The use of silicone drainage tubing to control post keratoplasty glaucoma. Eye. 1988;2:588–90.
- McDonnell PJ, Robin JB, Schanzlin DJ, Minckler D, Baerveldt G, Smith RE, et al. Molteno implant for control of glaucoma in eyes after penetrating keratoplasty. Ophthalmology. 1988;95:364–9. [PubMed]
- Beebe WE, Starita RJ, Fellman RI. The use of Molteno implant and anterior chamber tube shunt to encircling band for the treatment of glaucoma in keratoplasty patients. Ophthalmology. 1990;97:1414–22. [PubMed]
- Rapuano CJ, Schmidt CM, Cohen EJ, Rajpal RK, Raber IM, Katz LJ, et al. Results of alloplastic tube shunt procedures before, during, or after penetrating keratoplasty. Cornea. 1995;14:26–32.
- Coleman AL, Mondino BJ, Wilson MR, Casey R. Clinical experience with the Ahmed Glaucoma Valve implant in eyes with prior or concurrent penetrating keratoplasties. Am J Ophthalmology. 1997;123:54–61. [PubMed]
- Rumelt S, Rehany U. Implantation of glaucoma drainage implant tube into the ciliary sulcus in patients with corneal transplants. Arch Ophthalmol. 1998;116:685–7.
- Arroyave CP, Scott IU, Fantes FE, Feuer WJ, Murray TG. Corneal graft survival and intraocular pressure control after penetrating keratoplasty and glaucoma drainage devices. Ophthalmology. 2001;108:1978–85
- Al Torbak AA. Graft survival and glaucoma outcome after simultaneous penetrating keratoplasty andAhmed glaucoma valve implant. Corneaa. 2003;22:194–7
- Al Torbak AA. Outcome of combined Ahmed glaucoma valve implant and penetrating keratoplasty in refractory congenital glaucoma with corneal opacity. Cornea. 2004;23:554–9.
- . Romaniuk W, Fronczek M, Szkaradek P, Dorecka M. Implantation of Ahmed-type valve in the treatment of glaucoma, following penetrating keratoplasty. KlinOczna. 2004;106:170–2
- Ayyala RS, Zurakowski D, Monshizadeh R, Hong CH, Richards D, Layden WE, et al. Comparison of double-plate molteno and ahmed glaucoma valve in patients with advanced uncontrolled glaucoma. Ophthalmic Surg Lasers. 2002;33:94–101.
- Romaniuk W, Fronczek M, Szkaradek P, Dorecka M. Implantation of Ahmed-type valve in the treatment of glaucoma, following penetrating keratoplasty. KlinOczna. 2004;106:170–2
- Wilson MR, Mendis U, Smith SD, Ahmed PA. Glaucoma valve implant vs trabeculectomy in the surgical treatment of glaucoma: A randomized clinical trial. Am J Ophthalmol. 2000;130:267–73
- Wilson MR, Mendis U, Smith SD, Paliwal A, Haynatzka V. Long-term follow up of primary glaucoma surgery with Ahmed glaucoma valve implant versus trabeculectomy. Am J Ophthalmol. 2003;136:464–70.
- Topouzis F, Coleman AL, Choplin N, Bethlem MM, Hill R, Yu F, et al. Follow up of the original cohert with the Ahmed Glaucoma Valve implant in eyes with prior or concurrent penetrating keratoplasties. Am J Ophthalmol. 1999;128:198–4.
- . Alvarenga LS, Mannis MJ, Brandt JD, Lee WB, Schwab IR, Lim MC. The Long term results of Keratoplasty in eye with GDD. Am J Ophthalmol. 2004;138:200–5
- . Coleman AL, Hill R, Wilson MR. Initial clinical experience with the Ahmed glaucoma valve implant. Am J Ophthalmol
- . Kirkness CM, Ling Y, Rice NS. The use of silicone drainage tubing to control post keratoplasty glaucoma. Eye. 1988;2:588–90
- McDonnell PJ, Robin JB, Schanzlin DJ, Minckler D, Baerveldt G, Smith RE, et al. Molteno implant for control of glaucoma in eyes after penetrating keratoplasty. Ophthalmology. 1988;95:364–9
- Rapuano CJ, Schmidt CM, Cohen EJ, Rajpal RK, Raber IM, Katz LJ, et al. Results of alloplastic tube shunt procedures before, during, or after penetrating keratoplasty. Cornea. 1995;14:26–32.
Leave a Comment