
Dr. Aman Khanna, K15766, Dr. Apoorv Grover, Dr. Alok Sen
Purpose
To report the anatomical outcome of pars plana vitrectomy with SOI in paediatric patients presenting with severe traumatic endophthalmitis following open globe injury
Methods
A prospective case series of 18 patients (aged 2-13 years, mean age 5.68 ± 3.24 years) presenting with severe endopthalmitis, in tertiary eye care hospital in central India. All patients underwent PPV with SOI after primary repair. Vitreous was removed thoroughly with shaving of the peripheral vitreous base, cases with a minimum follow up of 6 months were included. The anatomical outcomes, as well as the associated complications were assessed
Results
The time of presentation following trauma varied from 1 to 15 days(mean duration 5.35 ± 4.47 days). Globe remained preserved in 17 eyes at the final follow up, with resolution of active infection. Fiveof the 18 eyes underwent silicone oil removal with reinjection of silicone oil within 6 months. Eleven of the 18 eyes had good media clarity with attached retina, while 2 had a detached retina. Four had hazy media with a pupillary membrane/occlusion pupillae. Keratopathy was notedin 4 cases.
Conclusion
Radical PPV with SOI can be used as a primary treatment option in severepaediatric traumatic endophthalmitis. Silicone oil injection allows control of infection and inflammation, as well as preserves anatomy of the eyeball in cases with an otherwise poor prognosis
Introduction –
Endophthalmitis is a devastating and vision threatening complication following penetrating ocular trauma, particularly in the paediatric age group, adding to physical, psychological and social burden due to the number of blind years the child has to survive with. It is estimated that out of 2.4 million eye injuries occurring in the United States annually, 35% are in children(1). Incidence of post traumatic endophthalmitis in children varies from 2.8% to 58.3%, much higher than that observed in adults (2). In a study conducted in North India it was observed to be 54.1% in children > 16 years with open globe injuries (3)
Despite recent advances in the management of endophthalmitis, final visual prognosis depends on the virulence of microorganisms, host resistance, and the time between the onset of disease and the initiation of treatment. Although there has been various studies supporting the role of vitrectomy in traumatic endophthalmitis it has been observed that repeat surgery may be required in large number of cases.
Silicone oil, a long-acting retinal tamponading agent, has been used for the treatment of complex retinal detachments associated with advanced proliferative retinopathy(4). Various studies have provided the evidence of silicon oil having anti bacterial and anti fungal properties (5) (6).
As there is not much evidence available in the literature to report the outcome of vitrectomy plus silicon oil in management of paediatric patients, we performed this study to report the anatomical outcome of pars plana vitrectomy with silicon oil injection (SOI) in severe traumatic paediatric enohthalmitis
Materials and methods-
This was a prospective interventional case series conducted in a tertiary eye care centre- “Sadguru Netra Chikitsalya” in Madhya Pradesh, India, over a period of 1 year August 2015 to September 2016. This Study included 18 eyes of 18 consecutive paediatric patients, presenting to the OPD with severe traumatic endophthalmitis following open globe injury (no fundus glow with severe vitritis on B scan). Light perception in all the patients at presentation was checked with an indirect ophthalmoscope in a dark room. In all patients prior to vitrectomy a B-Scan was performed to rule out IOFB or a retinal detachment.
Patient younger than 16 years of age having severe traumatic endophthalmitis following open globe injury and having a minimum follow up of 6 months were included in the study. Patients with no light perception at presentation and a retinal detachment on B scan were excluded.
Intervention -:All patients underwent primary Radical Vitrectomywith SOI. Radical vitrectomy involved a thorough removal of the vitreous along with shaving of peripheral vitreous base. 6eyes underwent corneo-scleral tear repair with Intravitreal antibiotic injection (gentamycin + ceftazedime) prior to vitrectomy
Results
The mean age was 6 ± 3 years (range 2-13 years). Out of 18 patients there were 11 males and 7 females, with mean days of presentation 5.1 days (range 1 – 15 days) (Table 1 ). Among 18 eyes 11 had a self sealed corneal tear, whereas 7 eyes had corneal tear with prolapsed Iris. Average follow up period was 9± 3 months. The most common mode of injury noted was by hypodermic needle, in 7 cases, followed by thorn injury in 3 cases. All patients in the study had a presenting Visual acuity of HM close to face or worse. (Table 2)
Table 3 shows Zone of involvement. Out of 18 cases 14 presented with Zone 1 injury and 4Zone 2. All patients were operated under general anaesthesia after undergoing required Pre-operative evaluation.
At the end of 6 month follow up 17 eyes had good anatomical outcome with a stable globe, inflammation was well controlled in all eyes, with none of the eye requiring an evisceration procedure. None of the eyes in the study had an associated Retinal detachment on B-scan at the time of intervention. Table 5 shows the outcomes at 6 month follow- up.
Complications seen at the final follow- up are given in Table -4. 2 eyes developed Retinal detachment in follow up period.Keratopathy was observed in 4 eyes, 4 eyes in the study developed a pupillary membrane, 1 eye noted for corneal decompensation
Out of 18 eyes 4 eyes required a repeat surgery (Table-6), 2 for retinal detachment, 1 for silicon oil in anterior chamber, and 1 for pupillary membrane. Eyes with repeat surgery for retinal detachment underwent vitrectomy with silicon oil infusion, at final follow up 1 had an attached retina whereas, other had a detached retina with PVR changes and was left alone.
Image 1 (A) Shows hazy fundus view of a patient at presentation , 1 (B) (C) and (D) shows postoperative images at 2 weeks 6 weeks and 5 months respectively, having an attached retina and an Oil filled Eye.
Discussion
It is estimated that approximately 18,000000 people globally suffer from uniocular blindness resulting from trauma (7). Open globe injuries account for majority of cases of post traumatic endophthalmitis. The incidence of OGI induced endophthalmitis varies from 6.8 to 54.2 %. In a series in India it was found to be 51 %(8).
It is observed that traumatic endophthalmitis is more frequently seen in children hailing from rural areas. In our study majority of children were from rural set up, this increased incidence of traumatic endophthalmitis in rural areas could be a result of poor awareness and scarce availability of treatment options in these areas.
In our study a male preponderance was observed, as 11/18were boys. Rishi Et alin a study also observed male predominance with 72% boys(9). Similar result was seen in study by Junejo et al (10) with 65 % boys. This could be attributed to more outdoor play and unsupervised playing activity by boys.
The most common mode of injury in our study was found to be by hypodermic needle followed by thorn, which was different than other studies in India who observed broom stick injury as the most common mode (3,9,10). The reason for increased incidence of trauma by hypodermic needle can be due to poor waste disposal system in rural areas.
There is a variedopinion on treatment of severe traumatic endophthalmitis. While some believing early vitrectomy to be superior to Intravitreal antibiotics (11,9) others showing no difference between vitrectomy and intravitreal antibiotics. Astudyobserved that patients undergoing early vitrectomy are 27 timesmore likely to have anoptimal anatomical outcome(9). In our study we performed a combination of Radical vitrectomy with SOI along with intravitreal antibiotics. In literature few authors have proposed this technique for treatment of traumatic endophthalmitis in adults. However for paediatric patients, a PubMed search using key words “Paediatric traumatic endophthalmitis with PPV, SOI” showed only one study wherein PPV with SOI was performed for traumatic paediatric endophthalmitis(12).
Radical vitrectomy allows better removal of inflammatory debris and microbiological load. It also prevents formation of peripheral vitreous traction bands by removal of organized vitreous and membranes that act as a scaffold for scar tissue growth and subsequent RD and PVR (13, 14).
Intraocular inflammation leads to lack of visibility of the fundus leading to a delay in management in these cases, this delay not only hampers the long term anatomical outcomes but also increases the chances of rhegmatogenous retinal detachment which can progress to PVR changes causing an irreversible damage to the retina.
We therefore, recommend SOI, which not only provides an optically clear media but also has been found to have anti microbial properties(15). Other advantages of SO being, it acts as a tamponading agent which prevents formation of Rhegmatogenous retinal detachment. It also leads to compartmentalization of the eye into an anterior compartment (ie, up to the anterior chamber) and a posterior compartment with a reduced vitreous-filled phase (between the retinal surface and the posterior surface of the silicone oil bubble), which has been hypothesized to enhance the therapeutic effect of intravitreal antibiotics(14, 16).
In our study we achieved a good anatomical outcome, as until the final follow up, no eye became phthisical. None of the eyes required evisceration as inflammation was well controlled. Similar results were obtained in studies by Bali et al (16) and Azad et al (14) in adult patients. Jin et al (12) using similar technique in paediatric traumatic endophthalmitis observedresults consistent with our study. In theirretrospective study of 107 eyes, 1 eye went into phthisis and 3 eyes required evisceration due to uncontrolled inflammation.
Performing a radical vitrectomy in paediatric patients with traumatic endophthalmitis is a challenging task as a PVD is absent, and induction is difficult. An excessive inflammatory reaction with dense adherent vitreous membranes is often present. There are high chances of occurrence of an iatrogenic break in these cases, especially due to poor visualization and a friable retina,hence no attempt should be made to peel the membranes. We observed an iatrogenic break in 2 cases while performing radical vitrectomy.
Use of silicone oil may be associated with complications such as emulsification of oil, or oil in anterior chamber which can lead to development of Keratopathyand secondary glaucoma. Postoperative B-Scan evaluation is difficult in Oil filled eyes. In this study 6 of the 18 eyes developed Keratopathy at final follow up. In study by Nagpal et al(17)in adult patients, 2 cases developed Keratopathy at final follow up.
In children the risk of general anaesthesia warrants the need for one time procedure, so this technique holds the advantage by eliminating or reducing the need of multiple interventions.
Age, visual acuity at presentation, type of trauma, source of trauma, lens injury, Retinal detachment, delayed presentation and culture positivity are identified as risk factors for a poor outcome(18,19,20). Rishi et al (9) in their study observed, children who received immediate treatment within 24 hours, had 9 times higher chances of achieving a better functional and anatomical outcome than those treated later. Another observation made was patients with associated Retinal detachment had a 5 fold more chances of an adverse outcome, in their multivariate analysis they did not found age, lens injury, culture positivity and type or source of trauma to be associated with poor outcome.
In our study 2 /18 children required a second surgery for subsequent retinal detachment, similar results were obtained in a study by Nagpal et al (17), who observed 10% casesrequiring a repeat surgery for RD in adult patients.
Few limitations of this study was a small sample size, absence of a control group, multiple surgeons, refraction and detailed visual status was not assessed in all cases, particularly younger age group. There is also a need for longer follow up.
To conclude Radical vitrectomy with SOI can be a useful method in cases of severe paediatric traumatic endophthalmitis, but to manage this complication best way is to raise the awareness about the importance of early presentation.
References
- Prevent Blindness America. The Scope of the Eye Injury Problem. 2010. Available from:https://www.preventblindness.org/sites/default/files/national/documents/fact_sheets/FS93_ScopeEyeInjury.pdf
- Bhagat N, Nagori S, Zarbin M. Post-traumatic infectiousendophthalmitis. Surv Ophthalmol 2011;56:214–51
- Narang S, Gupta V, Simalandhi P, Gupta A, Raj S, Dogra MR. Paediatric open globe injuries. Visual outcome and risk factors for endophthalmitis. Indian J Ophthalmol 2004; 52: 29-34
- Azen SP, McCuen BW, Stern W, et al. Vitrectomy with siliconeoil or perfluoropropane gas in the eyes with sever proliferative vitreoretinopathy. Silicone Study Report 3. Retina 1993; 13: 279-84.
- Azen SP, Scott IU, Flynn HW, et al. Silicone oil in the repair of complex retinal detachments: a prospective observational multicenter study. Ophthalmology 1998; 105: 1587-97
- Ozdamar A, Aras C, Ozturk R, Akin E, Karacorlu M, Ercikan C. In vitro antimicrobial activity of silicone oil against endophthalmitis-causing agents. Retina 1999; 19: 122-6
- Schwartz SG, Flynn HW, Jr., Das T, Mieler WF. Ocular infection:endophthalmitis. Dev Ophthalmol 2016;55:176–88
- Das T, Kunimoto DY, Sharma S, Jalali S, Majji AB,Nagaraja Rao T et al. Relationship between clinicalpresentation and visual outcome in postoperative andposttraumatic endophthalmitis in South Central India.Indian J Ophthalmol 2005; 53: 5–16
- E Rishi, P Rishi, VV Koundanya, C Sahu, R Roy and PS Bhende. Post-traumatic endophthalmitis in 143 eyes of children and adolescents from India. Eye (2016), 1–6
- Junejo SA, Ahmed M, Alam M. Endophthalmitis in paediatric penetrating ocular injuries in Hyderabad. J Pak Med Assoc. July 2010, Vol. 60, No. 7
- Cakir M, Cekic O, Pekel G, Yilmaz OF. Pars plana vitrectomyresults of exogenous endophthalmitis in children. Eur JOphthalmol 2010;20:424–8.
- Jin W, Xu Y, Wang W, Xing Y et al. Efficacy and Safety of 23-Gauge Pars Plana Vitrectomy/Silicone Oil Tamponade Combination for Treatment of Pediatric Post-TraumaticEndophthalmitis. Curr Eye Research. April 2017 ; DOI: 10.1080/02713683.2017.1297460
- Kaynak S, Oner FH, Koc¸ak N, et al. Surgical management ofpostoperative endophthalmitis: comparison of 2 techniques. J CataractRefract Surg. 2003;29(5);966-9
- Azad R, Ravi K, Talwar D, et al. Pars plana vitrectomy with or withoutsilicone oil endotamponade in post-traumatic endophthalmitis.Graefes Arch Clin Exp Ophthalmol. 2003;241(6): 478-83
- Oldrich Chrapeka et al.The in vitro antimicrobial activity of silicone oils used in ophthalmic surgery Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2012 Mar; 156(1):7–13
- Bali E, Huyghe P, Caspers L, et al. Vitrectomy and silicone oil in thetreatment of acute endophthalmitis. Preliminary results. Bull Soc BelgeOphtalmol. 2003; 288:9-14
- Nagpal M, Jain P et al. Pars Plana Vitrectomy With or Without Silicone Oil Endotamponade in Surgical Managementof Endophthalmitis. Asia-Pac J Ophthalmol 2012;1: 216 – 221
Table 1-: Demography and days at presentation
| Sr No. | Age /sex | Days of presentation | Cause of trauma |
| 1) | 3 / F | 10 | Thorn |
| 2) | 13 / F | 2 | Wood |
| 3) | 6 / F | 4 | Thorn |
| 4) | 2 / F | 8 | Needle |
| 5) | 9 / F | 7 | Needle |
| 6) | 4 / M | 1 | Wood |
| 7) | 3 / M | 6 | Needle |
| 8) | 5 / M | 2 | Umbrella |
| 9) | 9/ M | 3 | Wire |
| 10) | 11 / M | 6 | Thorn |
| 11) | 4 / M | 1 | Needle |
| 12) | 4 / M | 1 | Pen tip |
| 13) | 7 / F | 4 | Scissor |
| 14) | 2 / M | 4 | Hair pin |
| 15) | 5 / M | 15 | Needle |
| 16) | 7 / F | 15 | Needle |
| 17) | 3 / M | 2 | Iron |
| 18) | 12 / M | 2 | Needle |
Table 2 -: Presenting Visual Acuity
| Sr No. | Presenting VA |
| 1) | fixing |
| 2) | PL+ |
| 3) | PL+ |
| 4) | PL+ |
| 5) | PL+ |
| 6) | PL+ |
| 7) | Not fixing |
| 8) | PL+ |
| 9) | HM+ |
| 10) | HM+ |
| 11) | Not fixing |
| 12) | fixing |
| 13) | PL+ |
| 14) | Not fixing |
| 15) | PL+ |
| 16) | PL+ |
| 17) | Fixing |
| 18) | PL+ |
Table 4-: List of Complications
| Complications | Patients |
| keratopathy | 4 |
| Retinal detachment | 2 |
| Corneal decompensation | 1 |
| Pupillary membrane | 4 |
| Hypotony | 2 |
Table 3 -: Zone of injury
| Zone | No. Patients |
| Zone 1 | 14 |
| Zone 2 | 04 |
Table 5 -: Outcomes at final follow up
| Outcomes | No. Patients |
| Anatomical stability | 17 |
| Good media clarity with attached retina | 11 |
| Repeat Surgery with SOI | 04 |
Table 6 -: Reason for second surgery
| Repeat surgery (cause) | No. Patients (4) |
| Retinal detachment | 2 |
| Silicon Oil in AC | 1 |
| Pupillary membrane | 1 |
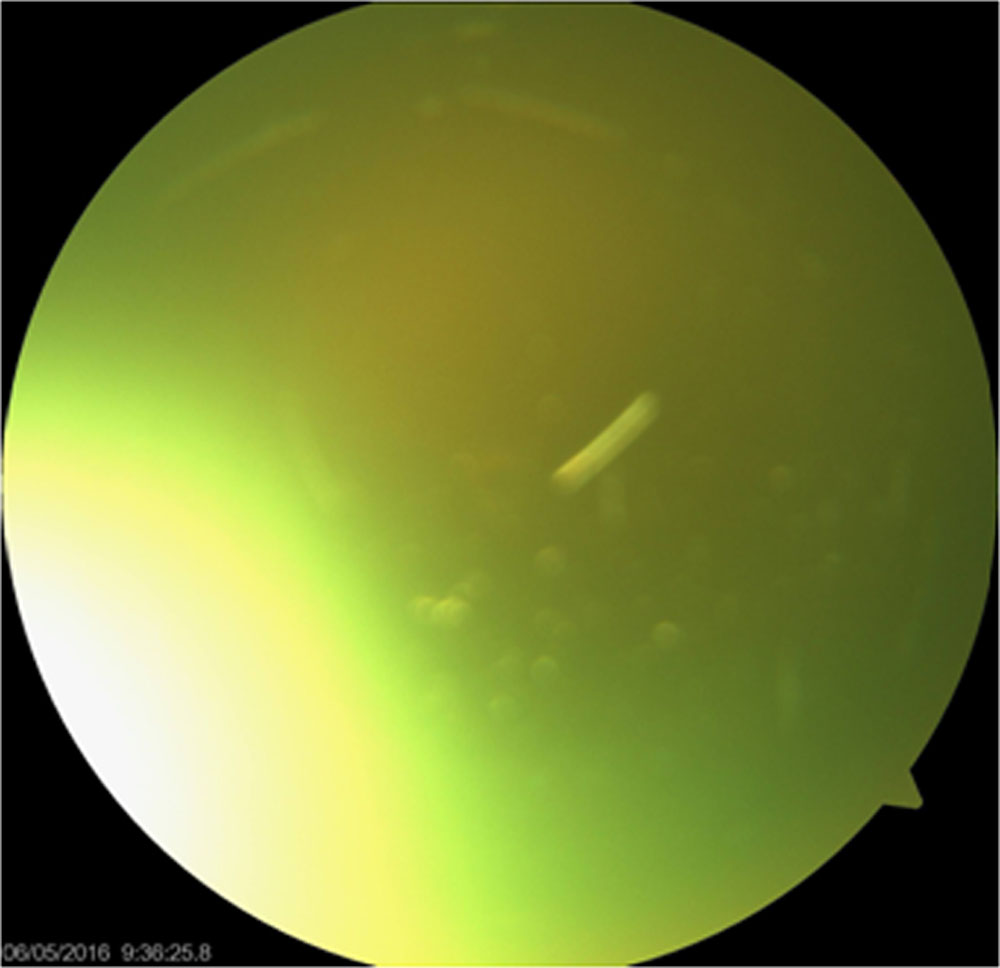
Image 1(A) Preoperative
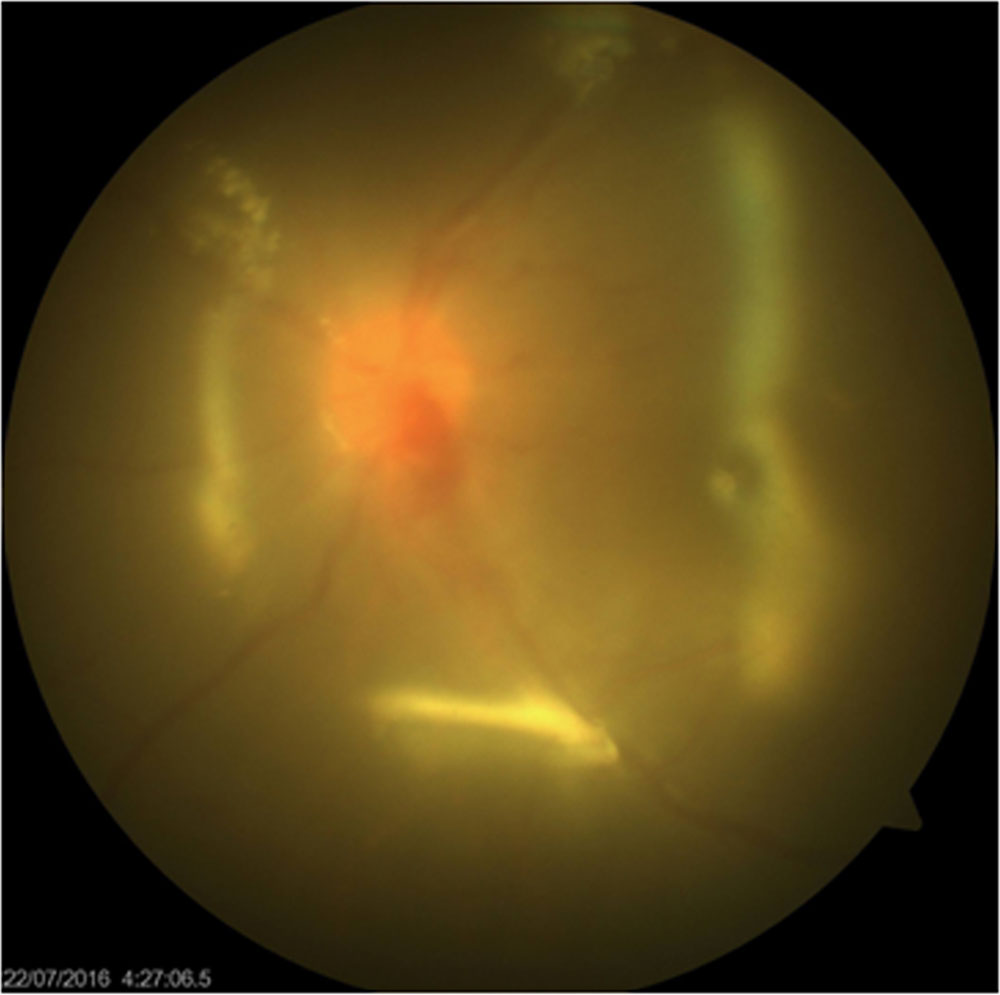
Image 1 (B) Postoperative 2 week ( Retina on and Oil filled eye)

Image 1 (C) Postoperative 6 week
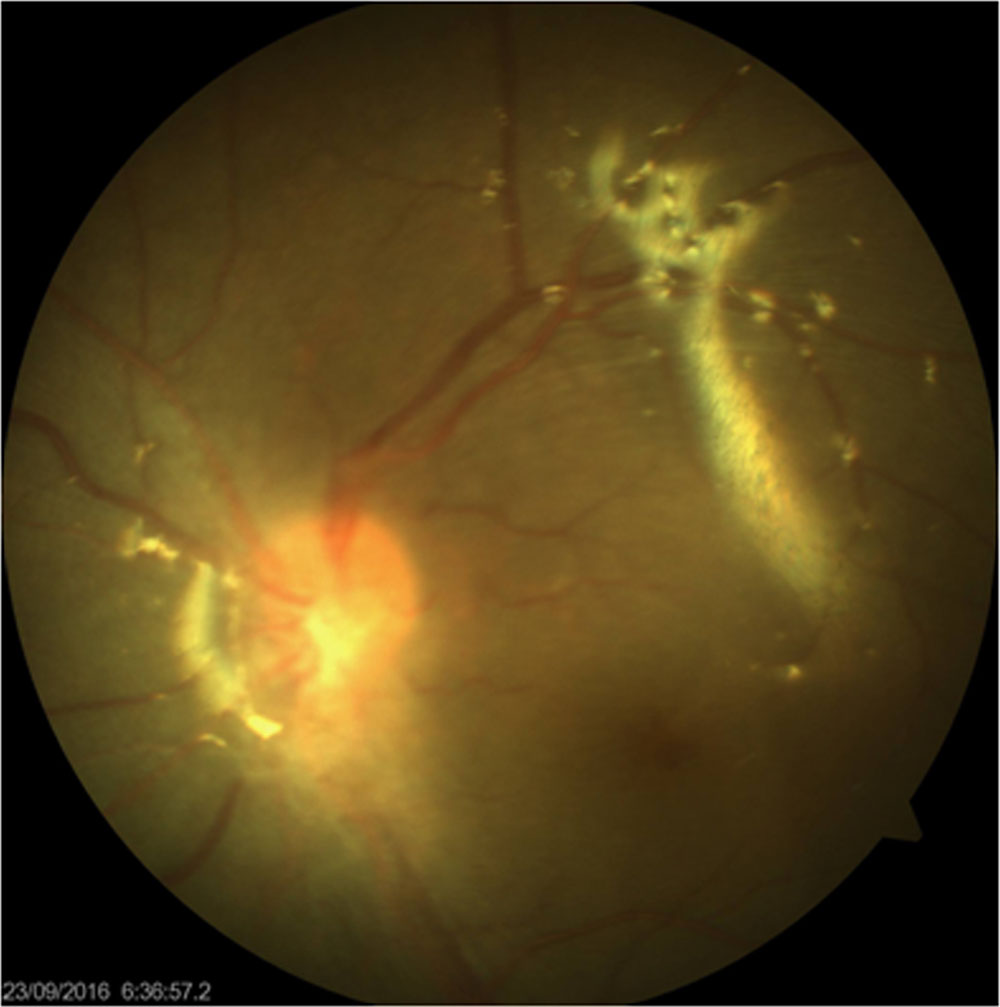
Image 1 (D) 5 month Postoperative image
Leave a Comment