
Dr. Divya Alex, A15662, Dr. Indu V P
ABSTRACT:
PURPOSE: To evaluate the clinical findings in contralateral eyes of PCV by multimodal imaging.
METHOD: Retrospective analysis of 75 clinically unaffected, treatment naïve other eyes of unilateral PCV was made with the help of multimodal imaging. SD OCT, FFA, ICG images were utilised in the study. The study population had a minimum followup of one year. Focus was given to analyse the various structural changes and to find out the precursor lesions in the clinically unaffected eye during the follow up period.
RESULTS: Mean age of study group was 64.4+5.2 years with female predilection.Fundoscopy revealed focal RPE changes(50.6%), drusen(40%) and PED(16%).SDOCT revealed Pigment Epithelial Detachment (PED) in 18 eyes. Of which 9 eyes had flat irregular pigment epithelial detachment(FIPED),5 eyes had serous and 4 eyes had drusenoid PED.The other SDOCT findings were RPE undulations(56%), focal ellipsoidzone loss over sickRPE(38.7%),Thumb like PED (6.7%)and Doublelayer sign(9.3%).All the cases which developed disease activity showed horizontal elongation of FIPED with a mean length of 2065+498u(P<0.001). EDI show pachyvessels(161.2u+10)in 81%eyes with subfovealchoroidal thickness of (392.8u+74).The other 9 eyes with serous and drusenoid PED with a PEDmean height of 99+24u showed an increase in vertical height not more than 54u.Of which one case developed active polyp within 6mnths(P>0.05). ICG revealed posterior pole dilated vessels(29.3%),BVN(4%), polyps(9.33%); active(5.33%) which all found to have a significant positive correlation in the disease progression.
CONCLUSION: Emphasis the importance of bilateral multimodal imaging in follow-up as the other eye of PCV is predisposed. Even though clinically silent, other eye findings may corroborate to the diagnosis of PCV. Elongation of the flat irregular PED may be considered as a precursor lesion for the PCV. Long term studies are warranted.
KEYWORDS: Indocyanine Green Angiography, Spectral domain OCT, Enhanced Depth Imaging, Flat irregular pigment epithelial detachment, polyps
DIVYA ALEX, INDU V.P
Giridhar Eye Institute, Kochi, Kerala.
ADDRESS FOR CORRESPONDENCE: Dr.Divya Alex, Giridhar Eye Institute, Ponneth Temple road,Kadavanthra,Kochi-682020,Kerala,India.
E-mail- alex.divya@gmail.com
INTRODUCTION
Polypoidal choroidal vasculopathy is an exudative maculopathy; a part of pachychoroid spectrum. The disease is characterised by an inner choroidal vascular network of vessels ending in an aneurysmal bulge often visible as a reddish-orange spheroid, polyp like structure. PCV is usually a bilateral disease. The majority of the patients with evidence of PCV in one eye eventually develop similar lesions in the fellow eye.9 Our study was based on this fact.
There are no much documented evidences on the precursor lesions of PCV. One of the most common differential diagnosis of PCV is exudative or wet Age Related Macular Degeneration. Soft confluent drusens and reticular pseudo drusens are the known precursors of wet AMD.4 However, the significance of putative risk factors of PCV has not been clearly addressed. Identifying the early lesion of PCV, which is highly prevalent in Asian population, might contribute to understanding the pathophysiology of PCV. Studying the contralateral eye of unilaterally active PCV patients might be one of the measures to investigate the precursor lesions, because the probability of a PCV patient developing PCV in the contralateral eye is higher than the probability of normal age-matched person developing PCV.4
Woong kang etal have suggested that Drusen like deposists (DLD) which are larger than 125 microns may be early preclinical markers of PCV.4
This study was conducted to find out the morphological features of the uninvolved eyes of PCV and to investigate the precursor lesions of PCV by studying the uninvolved contralateral eye of active unilateral PCV patients.
MATERIALS AND METHODS
This study was a retrospective observational analysis on the other eye of 75 patients diagnosed with unilateral PCV, done at the Vitreoretina Clinic of the Giridhar Eye Institute,Cochin. India, between August 2013 and May 2017. Inclusion criteria were: unilateral PCV in age group morethan that of 40 years. Exclusion criteria were: Associated retinal diseases like diabetic retinopathy, macular scar, CNVM, geographical atrophy, any history of intraocular surgeries within the follow up period.
Characteristic diagnostic features of PCV were the presence of reddish orange sub-retinal nodules, exudative maculopathy, hemorrhagic PED, spontaneous submacular haemorrhage in the fundoscopy, SDOCT findings like subretinal fluid, thumb like polyp,tall peaked polyp, double layer sign and thick choroid along with an ICG confirmation of the presence of branch vascular network or the polyp usually at the edge or notch of PED. The polypoidal hypercyanescence should appear within the first 6 minutes of ICG.A diagnosis of PCV was made through above mentioned multimodal imaging.
Colour fundus photo, SD OCT images, ICG images of the unaffected eye were analysed. Dense scan mode and enhanced depth imaging (EDI) were analysed in each follow up. . Dense scan parameters: 512 A-Scan within 16 frames,49 sections and 120 microns resolution in a 20 * 20 degree volume of the focused area. Dense scan is always better than a routine fast scan that chances of missing structural lesions are very less.
Colour fundus photographsof the unaffected eyes were evaluated for the presence of pigment epithelial detachments, drusen and pigmentary changes. Drusen were further grouped into small hard drusen, soft drusen, confluent drusen and reticular pseudodrusen. Small hard drusen were defined as drusen smaller than 63 μm, and soft drusen were defined as drusen that were 63 μm or larger with round and soft borders with evidence of corresponding lumpy bumby subRPE deposits on OCT. Reticular pseudodrusen were defined as drusenoid deposits on fundus, hypoautofluorescence on FAF, and evidence of corresponding subretinaldeposits on OCT. Pigmentary change was defined as depigmentation or reactive hyperpigmentation areas in fundus.
SDOCT images of the unaffected eyes were assessed for the presence of pigment epithelial detachments, subretinal fluid, ellipsoid zone disruption and specific features like thumb like polyp, tall peaked PED,notched PED and double layer sign(DLS).DLS was defined as two hyper reflective layers separated by a layer of hyper reflectivity. The inner layer is the hyper reflective irregularly elevated RPE and the outer layer is the inner layer of the Bruch’s membrane6. Flat irregular PED was defined as the separation of RPE from Bruchs without a gap of hyper reflectivity. If any of these signs were present, it was followed up and the measurement variations in the same were documented. SD OCT measurements were taken manually by a single masked observer. Choroidal thickness was measured manually with the help of built-in calipers in OCT software. Measurements were taken from the outer portion of hyperreflective RPE to the inner portion of hyperreflective zone corresponding to the choroidscleral junction. The height of the PED and the length of the PED were also measured. Height of the PED was measured as the vertical distance from the peak of the elevated hyperreflective RPE to the Bruchs membrane. Length was measured as the horizontal distance between 2 points where RPE is detached from Bruchs. The same parameters were used in the follow up scans.
ICG was repeated at the time of disease activity in the other eye.The presence of polyps, pulsatility,branching vascular network(BVN), choroidal hyperpermeability, and late geographic hyperfluorescence on ICGA were looked for. Active polyp was defined as nodular hypercyanescence appearing within first 6 minutes with a surrounding hypo- halo and leak in FFA. Quiescent polyps were defined as nodular hypercyanescence without a leak in FFA. Typically the early phase of the ICG angiogram (First one minute) reveals a distinct network of vessels within the choroid, called as Abnormal/Branching Vascular Network (AVN/BVN).7The polypoidal hypercyanescence should appear within the first 6 minutes of ICG.Late Geographic Hyperfluorescence (LGH) was defined as a hyperfluorescent lesion with clearly demarcated geographic margin, 10 min after the injection of ICG dye with a rosette-pattern and these strongly support the diagnosis of PCV.
STATISTICAL ANALYSIS
The data obtained from the patients were recorded and analysed. Results relating to categorical variables were expressed as counts and percentages. Two proportion Z test was used to find the difference in the two proportions. The results were considered statistically significant if P-value < 0.05.
RESULTS:
75 cases were enrolled in the study. Mean age of study group was 64.4+5.2 years. Female predilection was noted in a ratio of 3:2. BCVA in the unaffected eye was better than 6/9 in all selected patients.
37.33% of the cases had drusens in the fundus photographs. Of which 56.57% were small hard drusens and 41.33 %were soft drusens and one patient had reticular drusens. 50.67% had pigmentary changes in the fundus. (Figure 1)There was a positive correlation between the pigmentary changes in the fundus and the progression of the disease.
Table 1:
| Colour Fundus Findings | P value | |||
| No. of Patients with Disease Activity | No.ofPatients without Disease Activity | |||
| No. of Patients | 9 | 66 | ||
| Drusen | 3(33.33) | 25(37.88) | 0.7926 | |
| Pigmentary changes | 8(88.89) | 30(45.45) | 0.015** | |
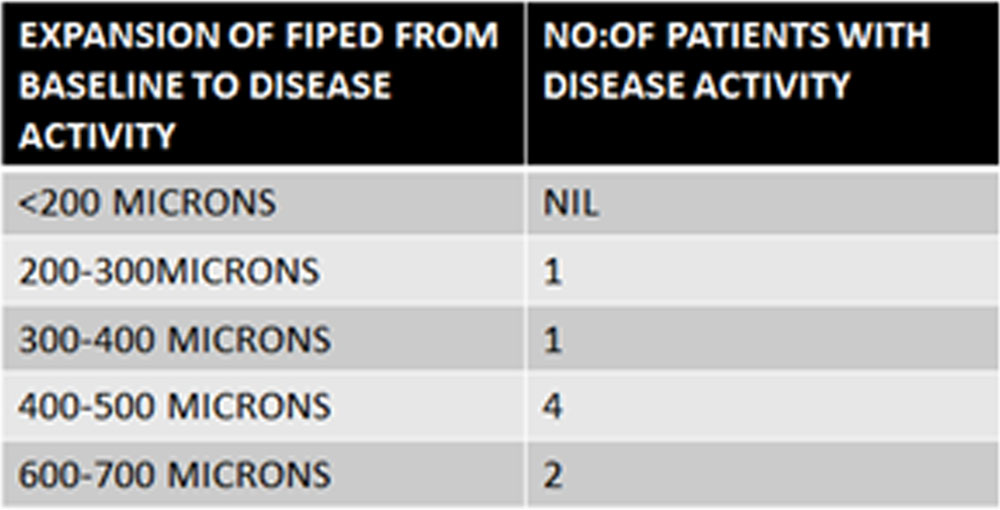
SDOCT revealed Pigment Epithelial Detachment in 18 eyes. Of which 9 eyes had flat irregular pigment epithelial detachment (FIPED).5 eyes had serous and 4 eyes had drusenoid PED. Flat irregular PED was found to be increasing in length in the followup scans taken. Of the 9 cases which had FIPED, the mean length of the detachmentat the beginning of study was 2065+106 microns. Out of these 9 cases, 8 cases developed disease activity within a mean time of 15 months+6 months. There was significant positive correlation between the elongation of the flat irregular PED and the progression of the disease with pvalue <0.0001 FIPED may be a precursor to the development of the DLS. All of these cases showed an expansion or increase in the length of the detachment when disease activity was detected by the presence of SRF in the followup scans.The mean length at the time of activity was 2868+156 microns. Mean increase in the length was around608+54 microns. (Figure2,3) The shortest followup period to develop disease activity was 6months and largest was 22 months. (Table2,4)
Table 2:
FIPED was structurally different from the Double layer sign(DLS).Table 3:, Figure 4
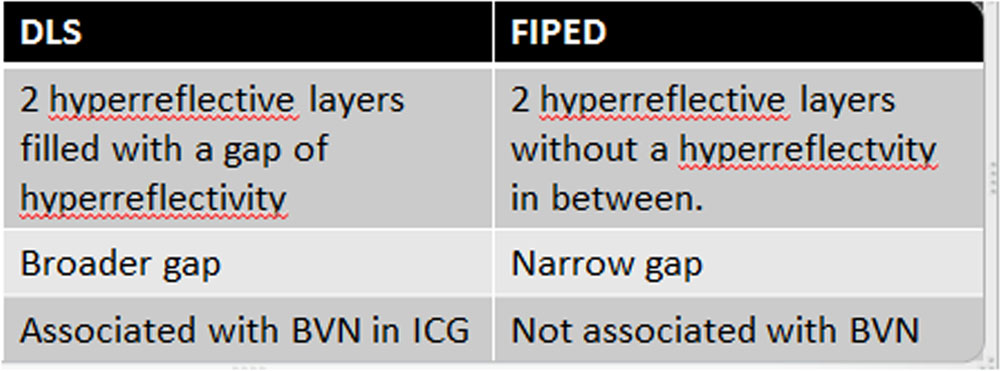
Table 4:
| SD OCT Features | P value | |||
| No. of Patients with Disease Activity | No. of Patients without Disease Activity | |||
| No. of Patients | 9 | 66 | ||
| 1) PED | ||||
| a) Flat Irregular PED | 8(88.89) | 1(1.52) | <0.0001** | |
| b) Serous PED | 1(11.11) | 4(6.06) | 0.571 | |
| c) Drusenoid PED | 0(0.00) | 4(6.06) | 0.4509 | |
| 2) Pachychoroid vessel | 9(100.00) | 51(77.27) | 0.1122 | |
| 3) Double layer sign | 3(33.33) | 1(1.52) | 0.048** | |
| 3)Thumb like PED | 2(22.22) | 0(0.00) | 0.061 | |
** indicates a significant association (p-value <0.05)
The association of serous PED and drusenoid PED failed to find a positive correlation in the PCV disease activity.The other 9 eyes with serous and drusenoid PED with a PED mean height of 99+24u showed an increase in vertical height not more than 54u.Of which one case developed active polyp within 6mnths(P>0.05)which failed to find a positive correlation with disease activity. Flat irregular PED with a property of lateral expansion found to have significant correlation with the probability of disease activity.
The other SDOCT findings were RPE undulations(56%), focal ellipsoidzone loss over sickRPE(38.7%),Thumb like PED (6.7%)and doublelayer sign(9.3%) of which the presence of DLS found to have a positive correlation on the progression of PCV.
Presence of a single or multiple thick choroidal vessels compressing the choriocapillaries (pachy vessel) was found in 81% of the other eye of PCV. The mean vertical height of the single thickest pachyvessel obtained by enhanced depth imaging was 161.2+ 10u. But the same finding failed to show a significant correlation on disease progression. The mean subfoveal choroidal thickness obtained was 392.8+74u which was definitely larger than the normal population.
On initial ICG analysis of the other eye, we found to have a positive correlation between the following features and the disease activity.Table 5: Figure 5
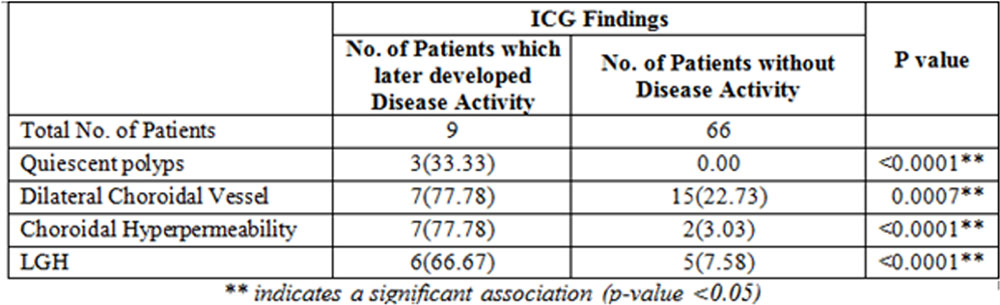
The repeated ICG taken at the time of disease activity showed the presence of active polyp in 4 cases and BVN in 3 cases. And in one case ICG was inconclusive.
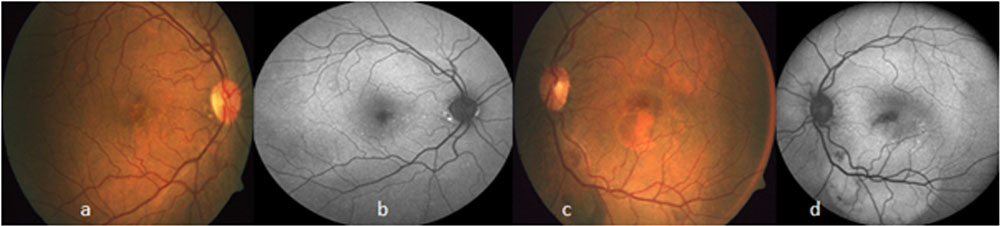
Figure1: (a) other eye of PCV with few drusens and pigmentary changes at fovea.(b) FAF showing hyperautofluorescent spots corresponding to the drusens. (c) active PCV eye with foveal haemorrhage and serous macular detachment (d)FAF showing hypoAF corresponding to the haemorrhage and hyper AF corresponding to the serous detachment.
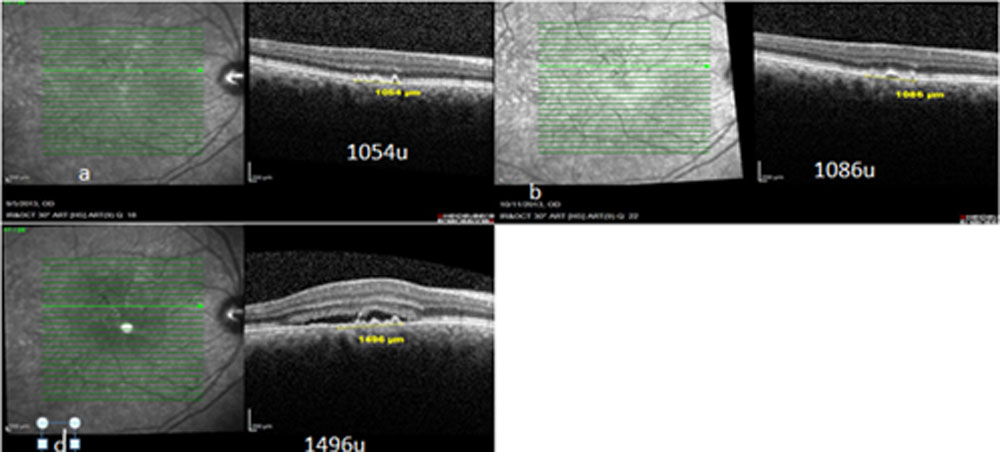
Figure 2: (a,b,c) SDOCT showing the progression of the flat irregular PED over a period of 13 months. (c) shows expansion of FIPED from 1054 microns to 1496 microns with appearence of subretinal fluid
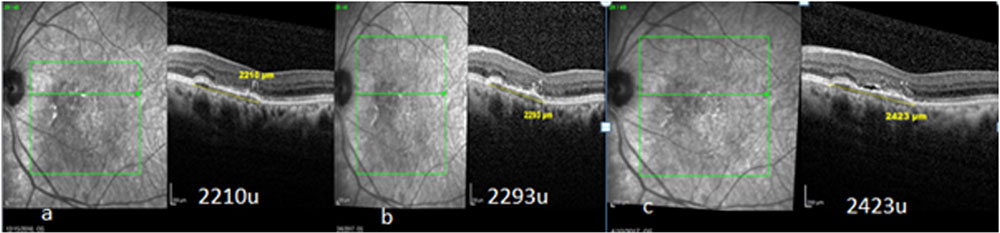
Figure 3(a,b,c) SDOCT images showing progression of the flat irregular PED over a period of 12 months with appearance of SRF.
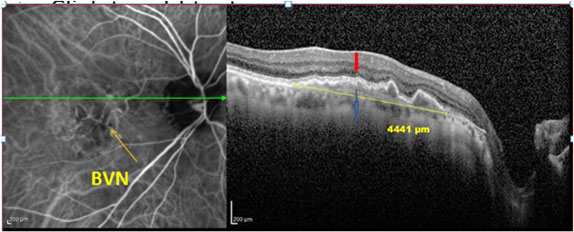
Figure 4 :Simultaneous ICG+OCT image: Double Layer sign(DLS) with BVN: shows two hyper reflective layers separated by a layer of hyper reflectivity, which is more broad than FIPED images.Red arrow showing RPE ,blue arrow showing Bruchs, yellow arrow on the right corresponding ICG image showing Branch vascular network(BVN)
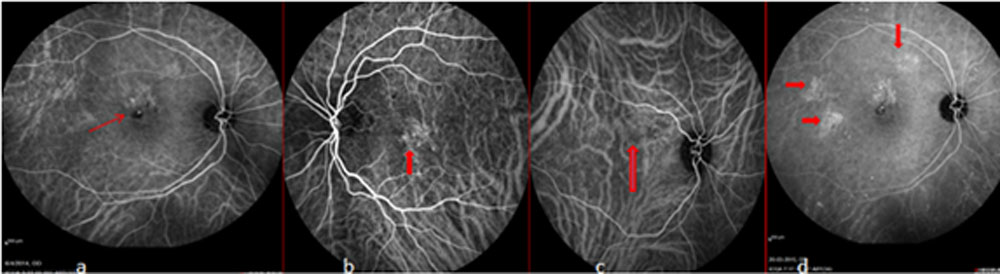
Figure5ICG frames(a)nodular hypercyanescence with surrounding hypo halo suggestive of active polyp. (b) network of choroidal vessels at fovea –BVN.(c)dilated choroidal vessels at posterior pole. (d)active polyp at fovea with Late Geographical hypercyanescence(red arrows)
DISCUSSION:
This study included the uninvolved, treatment naïve other eyes of polypoidal choroidal vasculopathy. Patients with evidence of PCV in one eye may eventually develop similar lesions in the fellow eye. The bilateral PCV has been reported in about 15 -20% of cases.12 Studying changes in the uninvolved fellow eye without active exudative maculopathy could be an effective method of evaluating precursor lesions of these diseases.
There has been only very few studies regarding the precursor lesions of polypoidal choroidal vasculopathy. The study by Kang,Lee and etal suggests that pigmentary change and sub-retinal or sub-retinal-pigment-epithelial grayish yellow deposits with an irregular margin described as drusen like deposits (DLD) are early precursor lesions of PCV. DLDs larger than 125 μm in size are specific precursor lesions of PCV. Identifying the precursor lesion of PCV has various implications like the pathophysiological process can be identified. Most importantly, the disease is identified at its earliest stage, sohelps in early treatment and better prognosis.4
In our study,we found a positive correlation between the pigmentary changes in the fundus which were defined as areas of depigmentation or reactive hyperpigmentation and the chances of development of PCV in the other eye.There was a significant correlation between the presence of Flat irregular PED(FIPED)and its lateral expansion with the disease progression in the unaffected eye.Most of the specific ICG findings like presence of polyps,choroidal hyperpermeability and late geographical hypercyanescence also showed positive correlation with the disease progression. All of these features showed a significant Pvalue <0.005. Presence of double layer sign also found to have a significant positive correlation on the disease activity.
Presence of a single or multiple thick choroidal vessels compressing the choriocapillaries (pachy vessel) was found in 81% of the other eye of PCV.But the same finding failed to show a significant correlation on disease progression. The mean subfoveal choroidal thickness obtained on EDI was 392.8+74u which was definitely larger than the normal population.The other SDOCT findings including focal RPE undulations, focal ellipsoidzone loss over sickRPE thumb like PED failed to find a positive correlation on the progression of PCV.
We would like to emphasis on the Flat irregular PED and its lateral expansion over time as a precursor of the polypoidal choroidal vasculopathy since this correlation has not yet published in any literature till date. Liu et al and De Salvo et al have described that the presence of OCT features like tall peaked PED, notched PED, double-layer sign and thumb-like polyp, it may be possible to suspect PCV and differentiate it from Wet AMD to a large extent. ICGA remains the gold standard in diagnosing PCV. We would also like to emphasise that FIPED is structurally different from the DLS. FIPED may be the precursor of development of DLS.
The earliest time period in which the disease activity found was 6months. The patient had pretty good vision 6/9 or better at the time of finding out the disease activity. So earlier we find out the lesion, the better the prognosis. In our study, association between the presence of serous PED or drusenoid PED was not stastically significant with the disease activity.
Other eye being predisposed to the disease, it should be meticulously searched on each followup for the signs of activity It is a common practice to take a macular line scan in the unaffected eyes of exudative maculopathy with a prejudiced mind. However, with the evidences based on this study,we strongly recommend to take a dense scan at the initial visit and on each follow up visit. If the other eye have any positive correlation features like pigmentary changes on fundus, flat irregular PED,DLS they should be kept under close monitoring to pick up the earliest sign of activity.
The main limitation of the study was the short term follow up of one year. The mean duration of the disease activity was 15 months. That means almost 50% of active PCV developed in the other eye during a follow up of more than 1 year. So long term studies are warranted.
CONCLUSION:
Our study emphasise the importance of multimodal imaging in finding the structural and morphological changes in the treatment naïve clinically unaffected PCV eyes. The presence of flat irregular Pigment Epithelial Detachment with its characteristic property of lateral expansion or elongation can be considered as a precursor lesion for Polypoidal choroidal vasculopathy. These cases must be kept under close monitoring.Long term studies may be helpful to pickup more precursor lesions of PCV which may throw light in identifying the pathophysiology of the disease.
FINANCIAL SUPPORT AND SPONSORSHIP: NIL
CONFLICTS OF INTEREST: THERE ARE NO CONFLICTS OF INTEREST
REFERENCES:
1)Yuzawa M, Mori R, Kawamura A. The origins of polypoidal choroidal vasculopathy. Br J Ophthalmol. 2005
2)Sasahara M, Tsujikawa A, Musashi K, Gotoh N, Otani A, Mandai M, Yoshimura N. Polypoidal choroidal vasculopathy with choroidal vascular hyperpermeability. Am J Ophthalmol. 2006;142:
3)Uyama M, Matsubara T, Fukushima I, Matsunaga H, Iwashita K, Nagai Y, Takahashi K. Idiopathic polypoidal choroidal vasculopathy in Japanese patients. Arch Ophthalmol. 1999;117:1035–1042
4)Yannuzzi LA, Ciardella A, Spaide RF, Rabb M, Freund KB, Orlock DA. The expanding clinical spectrum of idiopathic polypoidal choroidal vasculopathy. Arch Ophthalmol. 1997;115:478–485
5)Investigationof precursor lesions of polypoidal choroidal vasculopathy using contralateral eye findings. 2017 Feb;255(2):281-291. doi: 10.1007/s00417-016-3452-5.Graefes opthalmology
6)Sasahara M, Tsujikawa A, Musashi K, Gotoh N, Otani A, Mandai M, Yoshimura N. Polypoidal choroidal vasculopathy with choroidal vascular hyperpermeability. Am J Ophthalmol. 2006;142
7)Yuzawa M, Mori R, Kawamura A. The origins of polypoidal choroidal vasculopathy. Br J Ophthalmol. 2005
8)Martin J, Rodman J, Pizzimenti J et al. The “Double- Layer Sign”: In Vivo Imaging of Polypoidal Choroidal Vasculopathy. Optom Vis Sci 2013;90:e293- e300
9)Sato T, Kishi S, Watanabe G, et al. Tomographic features of branching vascular networks in polypoidal choroidal vasculopathy. Retina 2007;27:589–594
10)Tan CS, Ngo WK, Lim LW, Lim TH. A novel classification of the vascular patterns of polypoidal choroidal vasculopathy and its relation to clinical outcomes. Br J Ophthalmol. 2014;98:1528–1533
11)Yannuzzi LA, Sorenson J, Spaide RF, Lipson B. Idiopathic polypoidal choroidal vasculopathy (IPCV) Retina. 1990;10
12)Spaide RF, Koizumi H, Pozzoni MC. Enhanced depth imaging spectral-domain optical coherence tomography. Am J Ophthalmol. 2008;146:496–500.
13)Guyer DR, Puliafito CA, Mones JM, et al. Digital indocyanine-green angiography in chorioretinal disorders. Ophthalmology. 1992;99:287–291.
14)Stephen. J.Ryan. Fifth edition.Section3. choroidal vascular or bruchs membrane diseases.Chapter 71.polypoidal choroidal vasculopathy1285-1290
Leave a Comment