
Dr. Purnima Rajkarnikar Sthapit, P20216, Dr. Santosh G Honavar
Abstract:
Purpose: To study the treatment response of retinoblastoma with vitreous seeds (VS) to periocular topotecan (POT)
Methods: Retrospective interventional study of 38 eyes of 35 patients with retinoblastoma with VS who received POT with concurrent intravenous chemotherapy(IVC)
Results: The mean patient age was 24 (range, 3-77) months. Mean follow-up was 8.5 (range,1-15) months. Focal VS in 20 (52.6%) eyes were treated with a mean of 3 (range 1-7) POT, with regression in 16 (80%). Diffuse VS in 18(47.4%) eyes were treated with a mean of 4 (range 1-7) POT, with regression in 8(44%). In all, 24(63.2%) eyes had complete remission of VS with POT alone. Eye salvage was possible in 19 (95%) eyes with focal VS and 12 (66.7%) with diffuse VS. Enucleation was needed for persistent VS and viable tumor(5), viable tumor alone(1) and recurrent VS(1). None of the patients developed systemic metastasis.
Conclusion: POT concurrent with IVC is safe and effective in the management of vitreous seeds.
Key-words: Retinoblasotma, Periocular injection, Topotecan, Vitreous seeds
Key Messages:
Periocular injection of topotecan with concurrent intravenous chemotherapy is a safe and effective method of management of vitreous seeds in retinoblastoma
Introduction:
We have come a long way in management of retinoblastoma with the aim of saving life to saving vision with targeted therapy like intra-arterial chemotherapy and focal therapy like transpupillary thermotherapy (TTT) and cryotherapy. In spite of this, vitreous seeding still a poses a challenge for many ocular oncologists. The avascularity of vitreous chamber hinders the penetration of intravenously administered chemotherapy leading to persistent seeding in spite of the main tumor getting regressed. Thus intravitreous route of chemotherapy has been widely used to encounter the seeds. However, there is always a possibility of extraocular extension of viable tumor through the needle tract. Therefore intravitreous therapy is only safely given after the tumor is significantly reduced by systemic or intra-arterial chemotherapy. Thus, during the active phase of disease, periocular chemotherapy is the best alternative where intravitreous concentration of drug was found to be 6-10 times higher than that achieved by intravenous route within 30 minutes of injection.[1] Periocular carboplatin has already been proven to be have high intraocular concentration with little systemic side effects but serious local adverse effects like orbital fibrosis and optic nerve atrophy.[2,3,4] However, a dose of 2mg of periocular topotecan was reported to be effective and safer compared to carboplatin.[3,5]
Intravenous topotecan is believed to be safe and active in extraocular and relapsed/resistant intraocular tumors of retinoblastoma as well.[6,7] Topotecan given by intravitreous route has already been proven to be effective in treating vitreous seeds.[1,8,9] Periocular topotecan was first studied by Carcaboso et al in 2007 in rabbit models and was found to achieve considerable intravitreous levels due to its favoured passage through blood retinal barrier.[10,11,12,13]
Many studies has been done on use of periocular topotecan for retinoblastoma but to our knowledge this is the first study specifically done on the response of vitreous seeds to periocular topotecan.[1,2,5,7,12]
Here we used topotecan by periocular route with concurrent systemic chemotherapy to viable vitreous seedings in active tumors to study the vitreous seeds regression and eye salvage.
Subjects and Methods:
It is a retrospective, noncomparative, interventional study where we included 38 eyes of 35 consecutive retinoblastoma patients with vitreous seeds managed with periocular topotecan injections, conducted at the Ocular Oncology services of Centre for Sight Eye Hospital, Hyderabad from July 2013 to February 2017. The data was collected from our comprehensive medical record files and serial Retcam images of the patients during the course of treatment. Demographic data recorded from the first visit to hospital included age at diagnosis in months, gender, laterality and involved eye (right or left). All patients were grouped as per the ICRB (International Classification of Retinoblastoma) after detailed examination under anaesthesia. The number of tumors per eye and the basal diameter and height of the largest tumor was recorded. Presence of anterior chamber seeds, iris new vessels (NVI) or neovascular glaucoma (NVG) were grouped as clinically high risk patients for metastasis. The presence and extent of subretinal seeds and vitreous seeds were assessed and classified as focal if located 3mm or less from tumor and as diffuse if located further than that. Vitreous seeds were further classified into primary (present at the time of diagnosis), secondary (developed later during the course of treatment), persistent (remained even after completion of systemic chemotherapy for tumor) and recurrent (reappeared after a disease free interval).
Morphology of vitreous seeds was studied in terms of presence as dusts, spheres or clouds. Their location was also noted as being free floating in vitreous cavity, deposits on ciliary body or resting on prehyaloid or retrohyaloid space.[14,15,16]
The chemotherapy protocol included a standard dose of combination of standard or high dose of intravenous vincristine, etoposide and carboplatin in all patients with viable tumor and vitreous seeds.
All the patients in the study received a variable number of periocular injections of topotecan. First of all the eye to be injected was identified and periocular area cleaned with 5% povidone iodine solution. A wire speculum was put and eyeball was rotated and fixed at temporal gaze with tooth forcep. Under the direct visualization of microscope, 2mg (2ml) of Topotecan was injected at inferonasal quadrant in posterior subtenon layer with a 27 gauge needle. After withdrawing the needle, the injection site was pressed with cotton tipped bud for one minute before eye is padded with antibiotic ointment for 24 hours.[16] The patients were prescribed a tapering dose of steroid eye drops for 12 days, cyclopentolate 1% eye drop thice daily for seven days and ibuprofen syrup thrice daily for three days. Along with this, all patients also received a minimum of six cycles chemotherapy which was extended up to ten cycles when large viable tumor was still present in eyes, with potential for vision or globe salvage. There was an exception in one child who received 20 cycles of standard dose chemotherapy for multiple recurrences in both eyes over a period of three years.
Some patients also received focal treatment with transpupillary thermotherapy and cryotherapy wherever indicated. All the patients were called after four weeks for examination under anaesthesia and same treatment continued until complete regression of vitreous seeds or switched to intravitreal topotecan when the main tumor regressed precluding the fear of tumor seeding through the needle tract or until a decision for enucleation or external beam radiotherpay was taken. Even after the remission of tumor and vitreous seeds, examinations were continued every three months for possible recurrence. If the vitreous seeds recurrence was associated with significant tumor recurrence warranting systemic chemotherapy, then periocular topotecan was re-initiated and documented in the study. Whereas if there was only a small tumor recurrence, intravitreal topotecan along with TTT was given and these patients were excluded from the study. The outcome in every case and decision for further treatment was done by the senior author who was an experienced ocular oncologist.
The clinical data was entered in an Excel sheet and were analysed with regard to the outcome measures – vitreous seed regression pattern in focal and diffuse type, number of periocular and additional intravitreal injections required and eye salvage.
Results:
At the National Retinoblastoma Centre, Centre for Sight, Hyderabad, from July 2013 to February 2017, 38 eyes (14 right, 23 left) of 35 patients(22 male, 13 female) with vitreous seeds who received periocular topotecan with concurrent intravenous chemotherapy were taken up for this study. The mean patient age was 24 (range, 3-77) months. Among 35 patients, 19 had bilateral disease however only two had family history of retinoblastoma. On International Classification of Retinoblastoma (ICRB) grouping, maximum number of eyes fell into group D (n-23) followed by group E (n=10) and group C (n=3). Four patients in group E also had clinical high risk factors like anterior chamber seeds in one, NVI in two and NVG in one. Seven eyes had a single large tumor filling most of the vitreous cavity. There was more than one tumor in 12 eyes. Among 38 eyes, endophytic tumor and mixed endo-exophytic tumor was seen in 17 eyes each, 2 had pure exophytic tumor which developed secondary vitreous seeds later and two had diffuse infiltrative retinoblastoma.
The maximum basal diameter of the largest tumor ranged from 7-20mm (mean, 14.3mm; mode 18mm). Tumor height ranged from 3-18mm (mean 10.7mm; mode 10mm). Seven eyes had focal and eleven had diffuse concurrent subretinal seeds. Vitreous seeds were focal in 20(52.6%) eyes and diffuse in 18(47.4%). Twenty eight patients had primary vitreous seeds at presentation while seven developed secondary vitreous seeds later during the course of treatment. The various morphology of seeds documented were dusts (n=8), spheres (n=33) and clouds (n=18), though many had a combination of all three. Ciliary body seeds along with vitreous seeds were noted in four eyes. Vitreous seeds were located in prehyaloid area in six and retrohyaloid in one eye while rest of the patients had free floating vitreous seeds.
In those 38 eyes, there were a total of 42 episodes of vitreous seeding along with active tumor, where periocular topotecan was given. In all, a total of 150 injections were given in the entire study duration. Focal vitreous seeds in 20 eyes were treated with a mean of 3 (range 1-7) periocular topotecan, with complete regression in 16 (80%) eyes. Diffuse vitreous seeds in 18 eyes were treated with a mean of 4 (range 1-7) periocular topotecan, with complete regression in 8 (44%). In all, 24 (63.2%) eyes had complete remission of vitreous seeds with periocular topotecan alone. Of 14 eyes with persistent vitreous seeds, 8 needed an additional treatment with intravitreal toptecan injection before complete remission of seeds, one needed radiotherapy, while five eyes were enucleated. Recurrent vitreous seeds were seen in 18 eyes which were treated with periocular topotecan alone in five, re-initiation of same (systemic chemotherapy with periocular topotecan) in four, intravitreal toptecan in eight and enucleation in one. All patients received an average of concurrent standard dose chemotherapy of 6.4 cycles (range 0-20, mode 6) while 6 patients also received high dose chemotherapy of up to 8 cycles. Three patients also received 3 cycles of triple drug super selective intra-arterial chemotherapy. Mean follow-up was 8.5 (range, 1-15) months. At the end of the treatment, we could achieve 95% eye salvage rate in eyes with focal vitreous seeds and 68% eye salvage rate in those with diffuse vitreous seeds. Enucleation (n=7) had to be done for persistent vitreous seeds and a viable tumor (n=5), for large viable tumor alone (n=1) and recurrent vitreous seeds (n=1). However histopathological high risk factors were not documented in any of them. Apart from occasional conjunctival chemosis, no side effects were noted. None of our patients developed extraocular tumor extension or systemic metastasis.
Discussion:
Primary vitreous seeds arise from the budding of large endophytic tumors while secondary vitreous seeds arise from chemotherapeutic drug induced tumor necrosis. In both the cases, the systemic chemotherapeutic drug fails to maintain adequate concentration in relatively avascular vitreous cavity leading to persistent seeds despite tumor regression. In order to gain access to vitreous, intravitreal injection of carboplatin, melphalan and topotecan has been widely used by various authors to encounter these notorious vitreous seeds.[1,8,9,17]
Though the trend toward direct intravitreal therapy has limited the use of periocular treatments, there is always a risk of extraocular implantation of tumor through the needle tract when used in active stage of disease. Therefore, a safer and efficient route of chemo drug delivery was tried which is subconjunctival or subtenon’s injection. Many authors have successfully used it as an adjuvant route in cases of large tumors since periocular route has been found to have increased vitreous concentration and tumor regression than in systemic chemotherapy alone.[1,2,5,10,18] Among other chemodrugs, topotecan has been found to have good trans-scleral penetration, and is stable for longer periods with no sight threatening complications.[5,7,12,16,18]In this study we used posterior subtenon injection of topotecan with concurrent systemic chemotherapy in active stage of disease, specifically for all kind of vitreous seeds management. Out of 38 eyes, 18 had subretinal seeds as well which are believed to be a source of new tumor and thus vitreous seeds.[8,16,19]
Vitreous seeds were most common in ICRB group D (60%) in our study which was reported by Shields as well.[17] They were found to be arising almost exclusively from large endophytic or mixed tumors (89.5%) as explained by Munier.[14] The mean basal diameter and height generating vitreous seeds were 14.3 and 10.7mm respectively with seven patients having large tumor filling most of the vitreous cavity. Therefore larger the tumor the more chance of getting vitreous seeds during the course of treatment and hence the need for more aggressive management of the tumor and seeds.[16,19]
Complete remission of vitreous seeds with periocular topotecan alone was seen in 24 (63.2%) eyes, with a mean of three (range 1-7) injections for focal and a mean of four (range 1-7) injections for diffuse vitreous seeds, thus proving that periocular topotecan is a safe and efficient method for combating vitreous seeds during the active state of disease. It has been shown to be effective in tumor control as well.[5,10,12,16,18] The persistent vitreous seeds in rest of the patients (n=14) was successfully managed by intravitreous topotecan in eight patients and radiotherapy in one patient, while five eyes needed enucleation.
Periocular topotecan has been proved to be a safe route of drug delivery.[5,16,18,20] Though serious drug reaction was noted on carboplatin and topotecan given together by one author, we did not encounter such reaction.[21]
Manjandavida et all on the analysis of 14 articles by various authors on primary chemotherapy alone for vitreous seeds concluded that overall 30-70% of eye ultimately needed enucleation.[8] In our study, we could achieve 95% eye salvage rate in eyes with focal vitreous seeds and 68% eye salvage rate in those with diffuse vitreous seeds. Thus we conclude that periocular topotecan with concurrent primary intravenous chemotherapy is one the best options for effective control of vitreous seeds in retinoblastoma.
References:
- Shields CL, Lally SE, Leahey AM, Jabbour PM, Caywood EH, Shields JA. et al. When to Use Intravenous, Intra-Arterial, Periocular, and Intravitreal Chemotherapy.Curr Opin Ophthalmol. 2014;25(5):374-385.
- Abramson DH, Frank CM, Dunkel IJ. A phase I/II study of subconjunctival carboplatin for intraocular retinoblastoma. Ophthalmology. 106:1947-50.
- Mulvihill A, Budning A, Jay V, et al. Ocular motility changes after subtenon carboplatin chemotherapy for retinoblastoma. Arch Ophthalmol. 2003;121:1120–24.
- Schmack I, Hubbard GB, Kang SJ et al. Ischemic necrosis and atrophy of the optic nerve after periocular carboplatin injection for intraocular retinoblastoma. Am J Ophthalmol. 2006;142:310–315.
- Chantada GL, Fandino AC, Carcaboso AM, Lagomarsino E, de Davila MT, Abramson DH. et al. A phase I study of periocular topotecan in children with intraocular retinoblastoma.Invest Ophthalmol Vis Sci.2009 Apr;50(4):1492-6.
- Chantada GL, Fandiño AC, Casak SJ,Mato G, Manzitti J, Schvartzman E. Activity of topotecan in retinoblastoma. Ophthalmic Genet2004 Mar;25(1):37-43.
- Brennan RC, Qaddoumi I, Mao S, et al. Ocular Salvage and Vision Preservation Using a Topotecan-Based Regimen for Advanced Intraocular Retinoblastoma.J Clin Oncol. 35:72-77.
- Manjandavida FP, Honavar SG, Reddy VAP, Khanna R. Management and Outcome of Retinoblastoma with Vitreous Seeds. 2014;121:517-524.
- Stathopoulos C, Say EAT, Shields CL. Intra-arterial and Intravitreal Chemotherapy for Retinoblastoma. Curr Ophthalmol Rep. 2017;5:73.
- Carcaboso AM, Bramuglia GF, Chantada GL,Chiappetta DA, de Davila MT, Rubio MC.et al. Topotecan vitreous levels after periocular or intravenous delivery in rabbits: an alternative for retinoblastoma chemotherapy. Invest Ophthalmol Vis Sci. 2007 Aug;48(8):3761-7.
- Schaiquevich P, Carcaboso AM, Buitrago E, et al. Ocular pharmacology of topotecan and its activity in retinoblastoma. 2014 Sep;34(9):1719-27.
- 12. Carcaboso AM, Chiappetta DA, Javier AW, Ho”cht C, Fandin AC, Croxatto JO.et al. Episcleral Implants for Topotecan Delivery to the Posterior Segment of the Eye. Invest Ophthalmol Vis Sci. 2010;51:2126 –34.Mendoza
- PR,Grossniklaus HE.Therapeutic Options for Retinoblastoma. Cancer Control. 2016 Apr;23(2):99-109.
- Francis L. Munier. Classification and Management of Seeds in Retinoblastoma. Ophthalmic Genetics. 2014; 35(4): 193–207.
- Francis JH, Marr BP, Abramson DH. Classification of Vitreous Seeds in Retinoblastoma. Ophthalmology. 2016;123:1601-1605.
- Rao R, Honavar SG. Recent Developments in Retinoblastoma.DJO. 2016;27:50-61.
- Shields CL, Douglass AM, Beggache M, Say EAT, Shields JA. Intravenous Chemotherapy for Active Vitreous Seeding form Retinoblastoma. Outcomes After 192 Consecutive Injections. The 2015 Howard Naquin Lecture. Retina June 2016;36(6):1184–90.
- Mallipatna AC, Demaras H, Chan HS, et al. Periocular topotecan for intraocular retinoblastoma. Arch Ophthalmol2011;129:738–45.
- Shields CL,Honavar SG, Shields JA, Demirci H, Meadows AT, Naduvilath TJ. Factors Predictive of Recurrence of Retinal Tumors, Vitreous Seeds, and Subretinal Seeds Following Chemoreduction for Retinoblastoma.Archives of Ophthalmology. 2002;120(4):460-4.
- Kaliki S, Shields CL. Retinoblastoma: Achieving new standards with methods of chemotherapy. Indian J Ophthalmol 2015;63:103-9.
- Athale UH, Stewart C, Kuttesch JF, Moghrabi A,Meyer W, Pratt C. et al. Phase I study of combination topotecan and carboplatin in pediatric solid tumors. J Clin Oncol. 2002;20(1):88-95.
Acknowledgement:
I would like to thank Mr Vivekananda Reddy for helping out with the statistical analysis of the study.
Figures:
Figure 1. Focal vitreous seeds arising from large tumor (left).Complete regression of vitreous seeds along with tumor following perioular Topotecan(right).
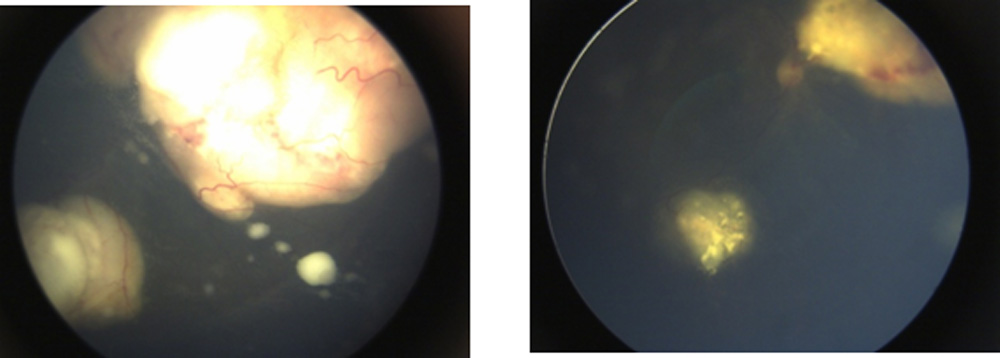
Figure 2. Diffuse vitreous seeds with budding endophytic tumor (left).Regressed tumor and vitreous seeds (right) following periocular topotecan.
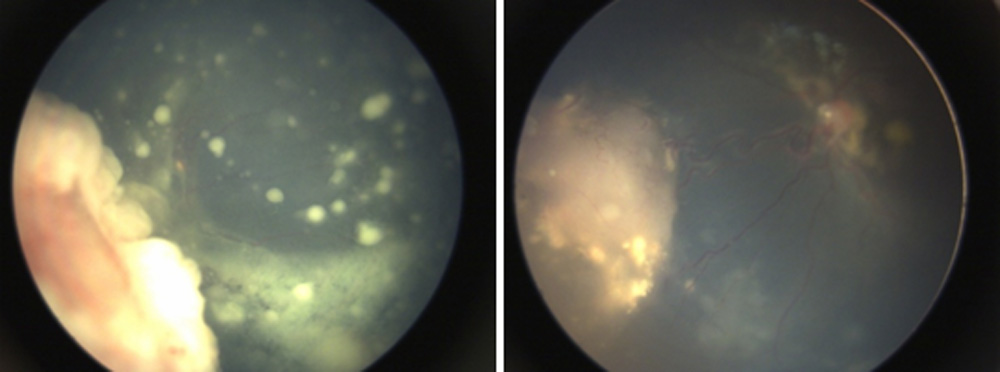
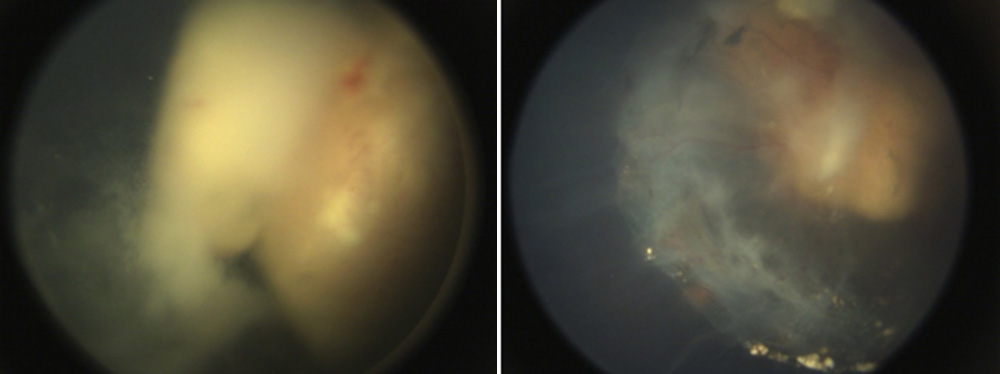
Figure 3. Vitreous cloud overlying the tumor (left).Regressing vitreous cloud and tumor (right) with periocular topotecan.
Leave a Comment