
Dr. Antony Arokiadass B, B18727, Dr. C A Nelson Jesudasen
ABSTRACT:
PURPOSE
This study was done to assess the use of after image slides available in the synoptophore in assessing Torsional Amplitudes (TA) and to compare TA between emmetropes and myopes.
METHODS
50 emmetropes (Gr I) and 50 myopes with corrected acuity of 6/6 (Gr II) were included. After orthoptic evaluation, the horizontal fusional amplitudes (HFA) was assessed. To assess TA, the after image slides were inserted horizontally aligned and rotated until the subject appreciated diplopia. The range for intorsion and extorsion were added to get TA.
RESULTS
Near point of convergence, near point of accommodation, HFA and TA in Gr I and Gr II were – 6.8 ±1.5 cm,7.3 ±1.7 cm, 11.8 ±2.1 deg, 8.4 ±1.4 deg and 6.7 ± 1.2 cm, 6.8 ±1.6 cm, 12.5 ±2.5 deg, 7.7 ± 1.5 deg respectively. TA was significantly lower in myopes (p=0.03)
CONCLUSION
After image slides can be used to assess TA. Myopes have significantly lower torsional amplitudes than do emmetropes.
Key Words: cyclofusion, torsional fusion, torsional vergence amplitude
Introduction
Fusion is the ability of the brain to form a single composite mental image from two similar images, each lacking in a small detail, which is perceived separately by the two eyes. Motor fusion aids sensory fusion by maintaining the image of objects of interest at the fovea of both the eyes. Measurement ofvergence amplitudes evaluates the ability of the motor system to overcome induced misalignment of the visual axis: – horizontally (convergence and divergence), vertically (sursumvergence and deosursumvergenvce) and torsionally( incyclovergence and excyclovergence). While horizontal and vertical misalignments can be induced by prisms, torsional vergence measurements necessitate the use of the synoptophore. Torsional fusional amplitudes are seldom measured and their variation in patients with different refractive errors have not been well studied. Special slides have been designed for measuring torsional amplitudes in the past.[1],[2]
Although these special slides have been reported in the scientific literature, after- image slides of the synoptophore,which are commonly available,can also be used to study the torsional fusional vergence. The present study was done to evaluate the usefulness of afterimage slides in measuring torsional vergence amplitudes and to assess the influence of refractive errors on the same.
Materials and Methods
This descriptive, comparative study was done in a tertiary eye care hospital, after approval of the Institutional Review Board. Patients aged 10 to 25 years were included in the study, and divided in to 2 groups; Group I of emmetropes andGroup II of myopes with a refractive error of>1 diopter.
Patients above 25 years, with previous history of ocular surgery or trauma,anterior or posterior segment pathology, manifest strabismus,no simultaneous perception, astigmatism of more than 0.5 cylinder, with BCVA <6/6, anisometropia (difference of more than 1 D between the eyes)and/or any systemic disorders, were not considered for participation in the study.
All the patients underwent a detailed evaluation including visual acuity assessment for near and distance, cover tests, Extra ocular motility assessment, orthoptic evaluation comprising measurement of near point of accommodation ( NPA) andnear point of convergence(NPC) with Royal Air Force( RAF) rule. Horizontal fusional amplitudes were measured with the synoptophore with fusional slides.
The torsional fusional amplitude was measured in the following manner. The after- image slides were placed in the slide holders, such that both were horizontally- oriented. The torsional position of the slide was changed by intorting the synoptophore arms, and the point at which the patient appreciated diplopia was noted. This procedure was then performed with the synoptophore arms extorted.Torsional range was calculated by adding the amplitudes of extorsion and intorsion, beyond which the patients appreciated torsional diplopia. The average of three readings was taken for each patient. In the myopic group, all tests were done with the appropriate refractive correction in place.
Results
100 patients(Group 1, 50 emmetropesand Group 2, 50 myopes) were included in the study. The demographic characteristics are summarized in Table 1.There was no significant difference in the demographic characteristics of both the groups.
TABLE 1: AGE AND GENDER CHARACTERISTICS OF THE STUDY PARTICIPANTS
| S No | Parameter | Emmetropic group(Gr I) | Myopic group(Gr II) | Statistical significance |
| 1 | Age ( in years) | 19.42 ± 3.54 | 19.84 ± 2.83 | t= -0.654, degree of freedom (df) = 98, P = 0.514 |
| 2 | Gender ( M:F) | 15: 35 | 22: 28 | χ 2 :1.53,df=1,P=0.22 |
The refractive error in the myopic group ranged from -1 to -7 D in either eye(mean RE :2.75±1.37 D; LE : 2.71±1.41 D). There was no significant difference in the refractive error between the two eyes in the myopic group(paired t test; t=1.013; df=49; p= 0.316). The comparison of orthopticparameters between both groups has been summarized in Table 2.
TABLE 2: COMPARISON OF ORTHOPTIC PARAMETERS BETWEEN THE EMMETROPES & MYOPESENROLLED IN THE CURRENT STUDY
| Sno | Parameter | Emmetropic group
( Gr I) |
Myopic
group ( Gr II) |
Statistical
Significance(unpaired `t’ test) |
| 1 | Near Point of Convergence | 6.8 ± 1.5 cm | 6.72 ± 1.26 cm | t = 0.287 df = 98;P = 0.78 |
| 2 | Near Point of Accommodation | 7.3 ± 1.7 cm | 6.8 ± 1.6 cm | t = 1.27 df = 98; P = 0.21 |
| 3 | Horizontal fusional amplitudes | 11.8 ±2.1deg | 12.5 ±2.5deg | t = -1.46 df = 98;P = 0.148 |
| 4 | Torsional fusional amplitudes | 8.38 ± 1.6 deg | 7.70 ± 1.5 deg | t = 2.199, df = 98;P = 0.030 |
Abbreviation: df= degree of freedom (Group 1 number [50]-1 + Group 2 number [50]-1= 48)
FIGURE 1: BOX PLOT SHOWING VALUES OF TORSIONAL FUSIONAL AMPLITUDES OF THE EMMETROPES & MYOPESENROLLED IN THE CURRENT STUDY
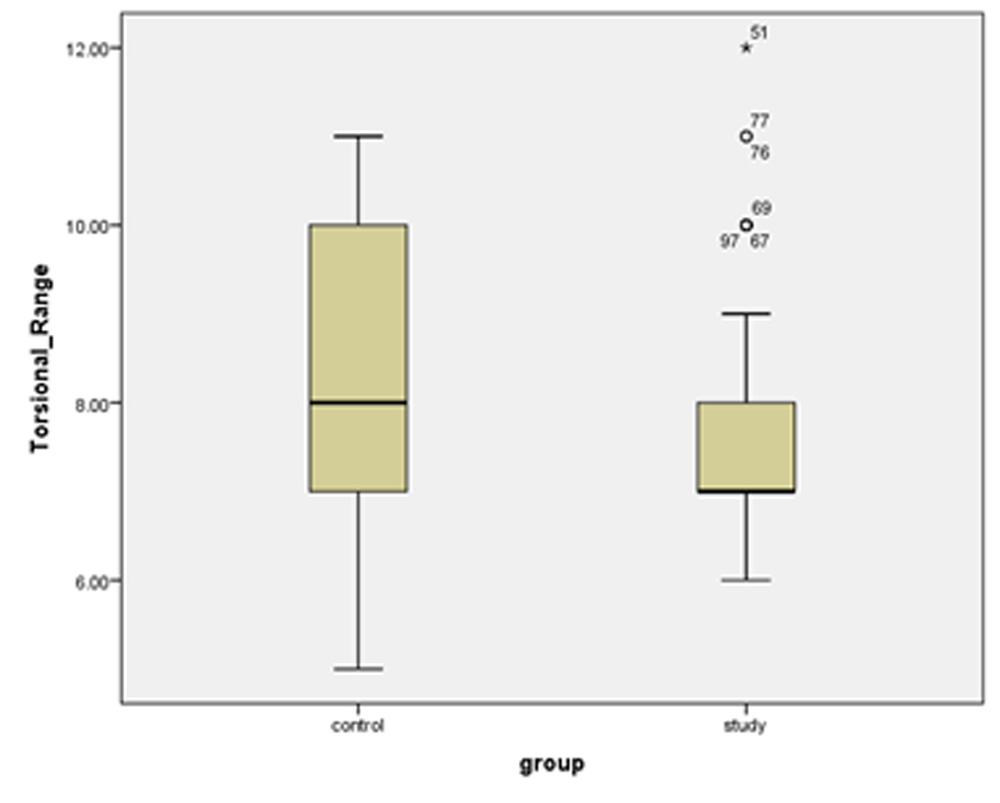
Control= emmetropes; Study= myopes
There was no significant difference in the horizontal fusional amplitudes between the emmetropes and myopes. The torsional fusional vergence amplitude was 8.38 ± 1.6deg in the emmetropes and 7.70 ± 1.5deg in the myopes(Table 2, Fig. 1); this difference was statistically significant.
Discussion
Cyclofusion or torsional fusional vergence, has been calculated by different authors using diverse techniques.Cylcofusion assumes importance in management of patients with cyclovertical muscle palsies, especially superior oblique palsy.
Sharma et al [1], using the Polaroid dissociation scotometer, studied cyclofusion in normal patients and those with superior oblique palsy. Special torsion slides were used for the assessment of the same. Hereported that cycofusion was about 12 degrees(break point) and 9 degrees( recovery point) for incyclovergence and excyclovergence in normal subjects.
Sen et al [2] studied the excyclo and incyclovergence across horizontal and vertical meridians in different gaze positions and found that torsional fusion in the horizontal meridian (5.98 ± 2.25) was more difficult compared to vertical meridian(9. 40±3.93). In the current study, we have compared the torsional vergences in the horizontal meridian alone. While Sen et al. used slides specially designed to measure cyclodeviation , commonly available after image slides were used by us in a horizontal fashion to assess the torsional vergence inthe current study.
Various studies have reported that subjects could fuse upto 16.8 degrees of excyclotropia and
11.8 degrees of incyclotropia.[3]Guytonobserved that cyclofusionupto 12 degis possible in the peripheral Pannum’s space and the degree of cyclofusion is better farther from the fovea. The extent of retinal areas involved in cyclofusion may differ with the slides used to measure torsional vergence. Hence, varied results may be obtained too.[4]
Differences invergence amplitudes in different refractive errors has not been well studied. Although a patient with refractive error wearing optimal spectacle correction may be technically considered an emmetrope, the results of several studies [5] ,[6]suggestthat there are significant differences in the fusional vergence and stimulus AC/ A ratio when refractive error is corrected by laser surgery. In the current study, myopes were found to have significantly lower torsional fusional vergences compared to emmetropes(Table 2, Fig. 1), although the significance of this difference is clinically not very marked.
A potential disadvantage of using these slides is that there would be no dissimilarity between the two slides, as is usually evident in the fusion slides of the synoptophore. Nevertheless, they have been found in this study to measure the torsional vergences with good validity. Another limitation of the current study is that only the break points have been calculated and not the recovery points.
Conclusion
After image slides can be used to measure torsional fusional amplitudes. Torsional fusional amplitudes are influenced by refractive error.
Bibliography
- Sharma P, Prasad K, Khokhar S. Cyclofusion in normal and superior oblique palsy subjects. J PediatrOphthalmol Strabismus. 1999 Oct;36(5):264–70.
- Sen DK, Singh B, Mathur GP. Torsional fusional vergences and assessment of cyclodeviation by synoptophore method.Br J Ophthalmol 1980; 64: 354-357.
- Georgievski Z, Sleep M, Koklanis K. Simulated torsional disparity disrupts horizontal fusion and stereopsis. J AAPOS OffPubl Am AssocPediatrOphthalmol Strabismus. 2007 Apr;11(2):120–4.
- Guyton DL. Ocular torsion: sensorimotor principles. Graefes Arch ClinExpOphthalmol Albrecht Von Graefes Arch KlinExpOphthalmol. 1988;226(3):241–5.
- Prakash G, Choudhary V, Sharma N, Titiyal JS. Change in the accommodative convergence per unit of accommodation ratio after bilateral laser in situ keratomileusis for myopia in orthotropic patients: prospective evaluation. J Cataract Refract Surg. 2007 Dec;33(12):2054–6.
- Han J, Hong S, Lee S, Kim JK, Lee HK, Han S-H. Changes in fusional vergence amplitudes after laser refractive surgery for moderate myopia. J Cataract Refract Surg. 2014 Oct;40(10):1670–5.
Leave a Comment