
![]()
Dr. Kirti Singh, K04958, Dr. Mainak Bhattacharyya, Dr. Punita Kumari Sodhi, Dr. Mainak Bhattacharyya, Dr. sumit kumar
ABSTRACT
Purpose: To compare results of a novel “Conjunctival frill/ smile incision” on surgically induced astigmatism (SIA) and patient discomfort vs conventional trabeculectomyin initial postoperative period.
Methods: Sixty trabeculectomy cases were subjected to either conjunctival frill incision, performed 1.5- 2.0 mm from limbus (Study group) or conventional fornix based conjunctival flap (Control group). Corneal astigmatism &suture induced discomfort was assessed by keratometry and a self-devised patient questionnaire respectively.
Results: Both groups generated a “with the rule” SIA, which was 1.77vs 2.42 at 1 week and reduced to 1.27vs 1.8 in study vs control group, after removal of sutures – both scleral flap releasable and conjunctival at 1 month. Patient discomfort score, revealed enhanced comfort in 37% patients (study group) vs 17% (control group) during early post- operative period. After 1 month of surgery, good comfort was regained in all cases.
Conclusion: This novel suturing technique results in reduced surgically induced astigmatism (SIA), patient discomfort during first month after trabeculectomy.
Keywords: Conjunctival frill, Smile incision, Trabeculectomy, Astigmatism, Patient discomfort
BACKGROUND
Since introduction of trabeculectomy by Cairns in 19681, trabeculectomy has undergone multiple modifications to increase both survival and safety of the procedure. Of these different modifications, type of conjunctival flap has been subject to much research. Conjunctival incision influences both bleb morphology and therefore bleb longevity. Comparative studies to determine differences between these two standard conjunctival incisions of fornix based and limbal based by Shuster et al2, Grehn et al3, Traverso et al4, and Brincker et al5, have documented similar IOP control and bleb morphology.
The preferred conjunctival incision in our setting over last decade has been fornix based after the key study of Khaw PT et al6 with the authors reporting “ring of steel” formation at incision site of limbal based conjunctival flaps, being a risk factor for bleb failure and preventing posterior extent of bleb. However, the issues plaguing fornix based conjunctival flap (FBCF) have been – need for anchoring/suturing of conjunctiva to limbusto prevent bleb leak and shallow anterior chamber. These anchoring sutures lead to patient irritation, tear film disruption and corneal astigmatism.This study was designed to evaluate a new modified conjunctival incision, a golden mean between limbus and fornix, called “conjunctival frill incision” or “Smile incision” so called due to its physical appearance on table.
PURPOSE
To compare results of a novel “Conjunctival frill/ smile incision” on surgically induced astigmatism (SIA) and patient discomfort vs conventional trabeculectomyin initial postoperative period
MATERIALS & METHODS
A prospective, double arm, pre- andpost-interventional studyincluded 60 trabeculectomy cases in patients with >18 yrs of age and excluded patients with evidence of any prior incisional surgery involving superior conjunctiva, dry eyes and prior vitreoretinal surgery. Corneal astigmatism and suture induced discomfort was assessed by keratometry &self-devised patient questionnaire respectively. The discomfort induced by conjunctival suturing was graded by a Likertscale as mild, moderate, severe depending on symptoms of watering, foreign body and blurring of vision.Tear Break UpTime(TBUT) used to assess for evaporative dry eye disease subsequent to derangement in ocular surface.
Patients were randomly divided into two groups, with one group was subjected to ‘Smile conjunctival frill trabeculectomy’ and second group to conventional fornix based trabeculectomy. All patients were followed up for minimal 6 months with IOP, bleb morphology (IBAGS grading on slit lamp plus AS-OCT), surgically induced astigmatism(automated keratometry) evaluated at follow up visits of week 1, week 2, 1 month, 3 months and 6 months. Tear break up time assessed at all follow up visits upto 3 months, andPatient Discomfort Scorecalculated at week 1, week 2, and 1 month.
SURGICAL TECHNIQUE
Peribulbaranesthesia without adrenaline, was given with proper care and minimal massage.Conjunctival incision was made 1.5 mm to 2.0 mm from limbusleaving a frill of conjunctiva attached. After adequately cauterizing the conjunctival bleeders, a scleral incision was made, in the form of an upward facing trapezium sized 4 by 3 mm. Superficial scleral flap was dissected till 1.5 mm of clear cornea. A side port entry was made 1-2 clock hours away from the margin of scleral flap and slow controlled release of aqueous was done while withdrawal, to prevent sudden hypotony. Intracameralpilocarpine was injected, followed by small amount of viscoelastic to tauten the iris. A bevelled anterior chamber entry was initiated with a 3.5 mm keratome, at base of scleral flap, at junction of blue grey zone. An inner sclerostomywas done with Kelly’s punch at base of the sclera flap and minimum of 2-3 punches were taken creating asclerostomy measuring 1.5 mm by 1 mm. A peripheral iridectomy was then performed. The superficial scleral flap was sutured with two – three fixed sutures and two releasable sutures. (Fig 1)
Conjunctiva was sutured in a running, horizontal mattress type,starting from one end with the suture knot resting away from the superior limbus. At end of surgery the bleb was raised by titration from side port.

Fig 1: Slit lamp photograph post smile incision trabeculectomy in immediate post-operative period
RESULTS :
The mean age was 41 ± 13 years (range 18-65 years) in study group and 49 ± 10 years (25-65 years) in control group. Both groups had almost similar sex distributions, male:female ratio 2:1.Glaucoma subtypes were heterogenous and equally distributed between angle closure glaucoma (25) and open angle glaucomaopen angle glaucoma (24), followed by juvenile open angle glaucoma (8), secondary glaucoma (2) and iridocorneal endothelial syndrome (1) cases.
Surgically induced astigmatism (SIA)
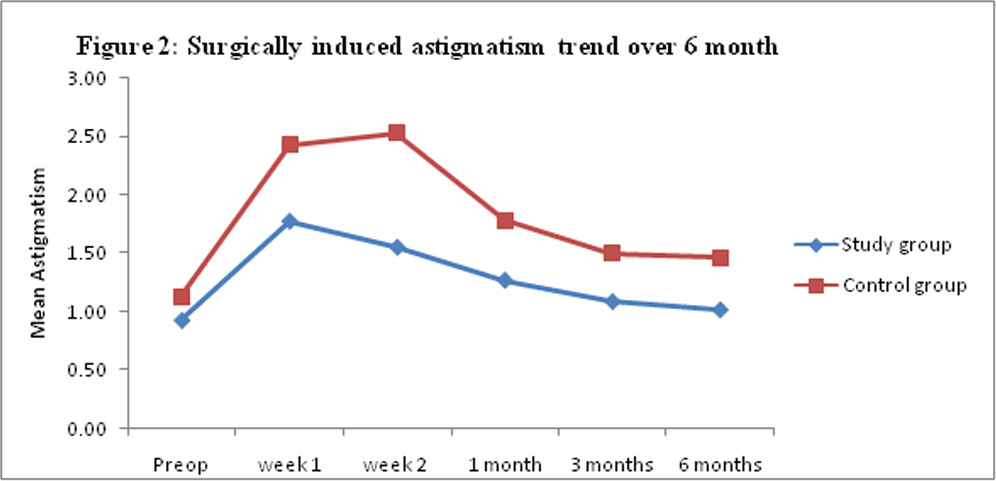
Surgically induced astigmatism (SIA) of corneal origin was “with the rule” of a magnitude1.77+ 0.8 vs 2.42 + 0.83 at 1 week in study vs control group. Study group documented a significantly less SIA versus control group (p < 0.001). Astigmatism was most pronounced during initial 2 weeks and reduced to 1.27+ 0.7 vs 1.8 + 0.8, (study vs control) after removal of scleral releasable and conjunctival sutures by first month of follow up.Table 1 and Figure 2 depict the same.
| Table 1:Surgical induced astigmatism (SIA) | |||||
| SIA | Study group | Control | Intergroup difference (study vs control)
Mann-Whitney U test |
||
| Mean ± sd | Intragroup difference from
Preop. levels Paired student t test |
Mean ± sd | Intragroup difference from
Preop levels Paired student t test |
||
| Preoperative | 0.93±0.56 | – | 1.13±0.78 | – | 0.41 |
| Week 1 | 1.77±0.8 | <0.001* | 2.42±0.83 | <0.001 | 0.001# |
| Week 2 | 1.55±0.72 | <0.001* | 2.53±0.83 | <0.001 | 0.001# |
| Post releasable suture removal | |||||
| 1 month | 1.27±0.65 | <0.001* | 1.78±0.77 | <0.001 | 0.007 |
| Post conjunctival suture removal | |||||
| 3 months | 1.09±0.57 | 0.006 | 1.47±0.8 | <0.001 | 0.065 |
| 6 months | 1.02±0.75 | 0.081 | 1.46±0.74 | <0.001 | 0.035 |
Change in vertical steepening was highly significant in study group upto 2 weeks (p<0.001), which subsequently reduced over time whereas for control group this change in vertical steepening remained significant up to 3 months (p<0.001) follow up.
Though the horizontal flattening was noted in both the groups (study and control), change in horizontal keratometric values were insignificant in both the groups. Table 2
| Table 2: Alteration in keratometry (vertical and Horizontal meridian) over time | ||||||
| Vertical keratometry
(mean change from preoperative) |
Horizontal keratometry
(mean change from preoperative ) |
|||||
| Study group | Control group | Intergroup difference student
t test |
Study group | Control group | Intergroup difference student t test | |
| Week 1 | 0.8 | 1.3 | 0.1 | -0.03 | 0.015 | 0.86 |
| Week 2 | 0.5 | 1.4 | <0.001 | -0.07 | 0.04 | 0.65 |
| 1 Month | 0.16 | 0.74 | 0.01 | -0.17 | 0.08 | 0.23 |
| 3 Months | 0.26 | 0.32 | 0.8 | -0.97 | -0.01 | 0.06 |
| 6 Months | 0.29 | 0.16 | 0.6 | -0.025 | 0.09 | 0.8 |
Patient comfort
Patients with a functioning filtering bleb frequently complain of eye irritation, watering and foreign body sensation. Often blebs become large in size and height, leading to burning sensation and pain, a feature of bleb dysesthesia.
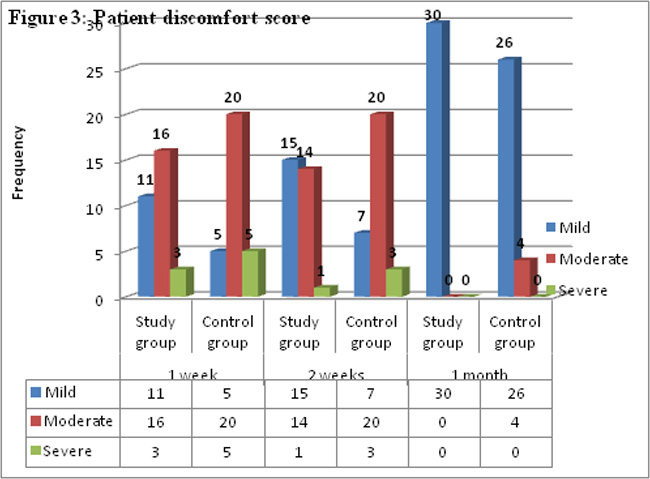
Patient discomfort score, measured by a self -devised Likert scale in our study to assess ocular surface showed that “Smile technique/ conjunctival frill incision “ (study group) led to significantly enhanced comfort in immediate post-operative period to trabeculectomy cases; subsequently comfort difference was minimal in the two groups. In the first week, 37% patients in study group had good comfort levels vs 17% in control group, found to be statistically significant (p-value = 0.038).Fig 3At first month follow up good comfort was regained in almost all cases irrespective of type of conjunctival incision.
Tear break up time
Tear disruption measured by TBUT, did not result in significant tear instability at any time during the post-operative period. It remained greater than 10 sec at 10.63 + 0.6:: 10.43 + 0.9 in study vs control group. This minimal disruption was most likely due to our practice of using frequent lubricant drops in the postoperative trabeculectomy cases.
DISCUSSION
Surgical induced astigmatism (SIA)
Post-operative astigmatism is one of the most important causes for diminution of vision after trabeculectomy. Hugkulstone et al in 1991 investigated changes in corneal astigmatism after trabeculectomy and reported a reduction in vertical corneal radius, inducing SIA of “With the rule” (WTR) astigmatism upto a follow up of 7 weeks.7Kook et al in 2001 studiedSIA over a longer follow up of 12 months period and reported “With rule astigmatism”(WTR) at 3 months, followed by an “against the rule” (ATR) shift at 1 year.8Claridge et al used computer-assisted corneal topography to document surgically induced astigmatism (SIA) after trabeculectomy and reported superior steepening of corneal curvature in majority , which they attributed to tissue contraction around the trabeculectomy site secondary to extensive scleral cautery. This finding was echoed by Rosen et al9and Vernon et al.10Dietze et al, mentioned the possibility of tight sutures and suggested a “posteriorly placed wound gape” from the internal sclerostomy as the cause.11Cunliffe et al (1992) in addition suggested that the internal sclerostomy allowed corneal edge of trabeculectomy to sink slightly thereby decreasing vertical radius of cornea.12
This surgically induced astigmatism is invariably corneal in origin and occurs more with use of corneal anchoring of conjunctiva, as required in fornix based conjunctival flap. As our study group involved conjunctiva to conjunctiva continuous suturing, without the suture being passed through cornea tissue, the resultant astigmatism was expected to be less. In addition, the astigmatism reduced after removal of both releasable and conjunctival suturing. Thus, only corneal astigmatism by keratometry was assessed.
The SIA in study group was found to be significantly less compared to control group using Mann Whitney U test with p-values < 0.001 at week 1 and 2 and p < 0.007 at month 1.On further evaluation change in vertical and horizontal meridian over time vertical steepening noted evident of With the rule astigmatism(WTR) most pronounced at week 2 and 1 month. The reduction in astigmatism was noted on further follow up maximum at 1 month and minimal thereafter, the prescription of glasses should therefore be delayed till 1 month; the same has been postulated by Delbeke et al who have reported stabilization of astigmatism at 3 month postop.13 The reduction in SIA was steep for study group with minimal astigmatism induced, resolving within 2-4 weeks, whereas for control group the SIA declined sharply in first month and slowly thereafter with decline continuing till 3 month. This would imply that “Smile incision” induces less SIA and causes more rapid resolution after suture removal.
Tear break up time
Mendes C et al studied tear instability post filtering surgery and reported significant reduction in tear break up time after surgery.14 Ji H et al in a cross-sectional study documented Dry Eye Disease(DED) to be relatively more common in patients with functioning filtering blebs following trabeculectomy than control group.15
No published study so far has evaluated tear instability in trabeculectomy cases based on type of conjunctival incision, to the best our knowledge.Tear disruption (assessed by BUT), was expected to be less for study group with no anchoring suturing. However, our study results did not corroborate this hypothesis since BUT values at 1 week and 1 month did not differ significantly between two groups although tear disruption was less in study group. This may be explained by the fact that our trabeculectomy cases are prescribed frequent lubricants during the immediate and intermediate post op period, which could mitigate dry eye effect subsequent to tear film disruption by suturing.
Patient comfort
In our study 37% (11/30 patients) in study group documented good comfort level versus 17 % (5/30) in control group at 1st week follow up. After suture removal, in both groups the comfort level improved; to 50 % in study group and 23 % in control group. This indicates a significant improvement in comfort score in immediate post- operative period in patients with Smile incision vs fornix based incision. At 1 month follow up, good comfort was regained in almost all patients irrespective of type of suturing in 87 – 100 % cases. This finding implied that Smile technique/ conjunctival frill incision gave more comfort in immediate post- operative period to trabeculectomy cases in the initial fortnight; subsequently comfort difference was minimal in the two groups. To the best of our knowledge no prior study has evaluated patient discomfort post trabeculectomy
CONCLUSION
This novel suturing technique results in reduced SIA, patient discomfort during first month after trabeculectomyand is equally effective in intraocular pressure (IOP) control. Reduction of surgical time and corneal distortion are further benefits of this technique. Thus, this technique can be easily adopted for trabeculectomy especially in eyes with no prior intraocular surgery.
REFERENCES
- Cairns JE. Trabeculectomy.Preliminary report of a new method.Am J Ophthalmol. 1968 Oct;66(4):673-9.
- Shuster IN, Krupin T, Kolker AE, Becker B: Limbus-v-fornix-based conjunctival flap in trabeculectomy: A long term randomized study. Arch Ophthalmol. 1984;102:361-2.
- Grehn F, Mauthe, Pfeiffer N:Limbus-based versus fornix-based conjunctival flap in filtering surgery. Int Ophthalmol 1989,13:139-43.
- Traverso CE, Tomey KF, Antonios S. Limbal- vs fornixbasedconjunctival trabeculectomy flaps. American Journalof Ophthalmology 1987;104(1):28–32.
- Brincker P, Kessing SV. Limbus-based versus fornix-based conjunctival flap in glaucoma filtering surgery. Acta Ophthalmol (Copenh). 1992;70:641–4.
- Khaw PT, Dhingra S. The Moorfields Safer Surgery System. Middle East Afr J Ophthalmol. 2009; 16(3): 112–115
- Changes in keratometry following trabeculectomy. Br J Ophthalmol 1991;17:217-8.
- KookMS, KimHB, LeeSU. Short term effect of Mitomycin-C augmented trabeculectomy on axial length and corneal astigmatism. J Cataract Refract Surg. 2001;27:518–23.
- ClaridgeKG, GalbraithJK, Karmel V et al. The effect of trabeculectomy onrefraction, keratometry and corneal topography .Eye.1995;9:292–8.
- Vernon SA, Spencer AF. Intraocular pressure control following microtrabeculectomy. Eye. 1995; 9: 299-303.
- Kawana K, Kiuchi T, Yasuno Y, Oshika T. Evaluation of trabeculectomy blebs using 3-dimensional cornea and anterior segment optical coherence tomography. Ophthalmology 2009; 116(5):848–55.
- Cunliffe IA, Dapling RB, West J, et al. A prospective study examining the changes in factors that affect visual acuity following trabeculectomy. Eye. 1992;6:618–22.
- Delbeke H, Stalmans I, Vandewalle E, Zeyen T. The Effect of Trabeculectomy on Astigmatism.J Glaucoma. 2015; 11: 1-5.
- Mendes CRN, Hida RY, Kasahara N.Ocular Surface Changes in Eyes with Glaucoma Filtering Blebs. Current eye research. 2012, 37(4):309-11.
- Ji H, Zhu Y, Zhang Y, Li Z, Ge J, Zhuo Y. Dry Eye Disease in Patients with Functioning Filtering Blebs after Trabeculectomy. PLoS ONE. 2016; 11(3): e0152696.
Leave a Comment