
Dr Supriya Shetty, S20959, Dr, Savitha Arun, Dr. Namita C. Anagol
Abstract: This study was conducted at tertiary eye care centre with total sample size of 52 patients. Each group included 26 patients. Patients included in study were patient between 3-12 years of age attending the outpatient department and followed up for one year at interval of 3 and 6 months. Patients were assessed for type of amblyopia, visual acuity, cycloplegic refraction, contrast sensitivity, stereopsis .Patients of each group were followed up for above mentioned parameters. Patients were divided according to age group and occlusion therapy was advised with minimum of 2 hours of patching daily for near activities. VTS4 therapy group were advised exercises with software including office therapy of 15- 20 sittings and home therapy with compact disc installed with software. Conclusion: Improvement in best corrected visual acuity for distance at the end of 6 months was better in VTS4 therapy compared to occlusion group. Improvement in contrast sensitivity and fine stereopsis was noted in both groups but better improvement with VTS4 therapy.
Keywords: Amblyopia, Occlusion,Patching,VTS4, Visual Acuity, Stereopsis, Contrast Sensitivity
Introduction :Amblyopia is defined as “Decrease of visual acuity in one eye caused by abnormal binocular interaction occurring in one or both eyes as a result of pattern vision deprivation during visual immaturity for which no cause can be detected during the physical examination of the eyes and in which appropriate cause is reversible by therapeutic measure”1. Amblyopia therapy effectively restores normal or near normal visual function by eliminating eccentric fixation and also by developing more extensive synaptic input to visual cortex. It improves monocular deficits of visual acuity, monocular fixation, accommodation and ocular motility to establish binocular single vision. The most accepted therapy for treatment of Amblyopia is occlusion therapy, where the sound eye is patched either by part time or full time occlusion according to severity of Amblyopia and age of the patient. Occlusion of the normal eye improves visual stimulation of the affected eye, thus promoting binocular single vision.
Occlusion therapy works on the principle of patching the normal eye to simulate visual perception in amblyopic or lazy eye. Duration of patching of the eye with better visual acuity is decided based on the age of the patient and density of Amblyopia. Poor compliance was a major drawback of this treatment hence other modes of treatment were also considered2.Another newly accepted therapy for Amblyopia is vision therapy also known as Optometric Vision Therapy. It improves specific dysfunction of the vision system. Active vision therapy is designed to improve visual performance by patient’s conscious involvement in sequence of specific controlled visual tasks or procedures. This therapy for Amblyopia is designed to remediate deficiencies of specific areas like eye movements, fixation, spatial performance, accommodative efficiency and binocular function. Goal of vision therapy is to remediate these deficiencies along with subsequent equalization of monocular skills and finally integration of the amblyopic eye into binocular fixation.VTS4 program is a form of vision therapy which promotes visual stimulation by active vision therapy. Patients are trained with exercises using this software in the hospital known as office therapy and asked to continue the sessions at home using software installed in a compact disc with module for training at home and followed up on regular intervals to assess improvement.
Epidemiology of Amblyopia:
Prevalence of Amblyopia:
Amblyopia is the most common cause of uniocular reduced visual acuity in children with a prevalence of around 0.5% to 3.5% 3.
Incidence and Prevalence in South Indian Population: A Study conducted in South Indian population showed the incidence and prevalence of Amblyopia as 1.1% . A total of 63.7% children had mild to moderate Amblyopia, whereas (36.3%) had severe Amblyopia.4.The prevalence of Amblyopia is higher when associated with developmental disorders such as Down ’s syndrome, cerebral palsy, prematurity, low birth weight and ROP5,6.
Treatment of Amblyopia:
1.Refractive Correction and Adaptation:
2.Occlusion therapy:
Occlusion of the better eye has been the mainstay of Amblyopia treatment for more than two centuries for which treatment traditionally involves complete total occlusion of the non-affected eye. The aim of occlusion is to stimulate the amblyopic eye by suppressing the vision in the dominant eye. This forces the amblyopic eyes to visualize, equalize the vision, attain an optimum level of visual acuity and centralize fixation. The most common method is total occlusion of which there are two types:
Total occlusion (all light and form) : In this therapy, patch is applied to the periorbital skin of the non affected or less amblyopic eye made from usually hypoallergenic materials. This is most common and the preferred choice of treatment. Examples of which include hypo-allergenic adhesive skin patches or spectacle-mounted occluders that fit around the spectacle lens in cases of skin irritation to skin patches. Coverlet and Opticlude patches are used widely7. Rarely the use of an opaque contact lens is used to treat the condition. Problems of irritation, poor fitting lens and anterior segment complications have been documented8.
Total occlusion (excluding form):This allows penetration of some light. This type requires the use of opaque patches that are generally adhered to the spectacle lens, for example blenderm or Bangerter foils.
Conventional occlusion has contributed significantly to the treatment of Amblyopia, as it is convenient and cost-effective. There is no consensus, however, regarding the amount of prescription required for treatment. Examples of regimens include:
- “minimal occlusion” (15 minutes to 20-60 minutes/day)
- “part-time” (1-6 hours/day)9
- “full-time” (6 -8 hours/day)
- “constant” (all waking hours)10
Other prescription methods include a ratio according to the age of the amblyopic patient. One week per age of child ratio is taken, for example, 5 weeks of constant occlusion would be prescribed for a 5 year old amblyopic child. Lithander and Sjostrand applied 1 day per age of child with 1 day free, for example, 2 days of constant occlusion for a 2 year old amblyopic child with 1 day free or 5 days of constant occlusion for a 5 year old amblyopic child with 1 day free11. Prescribed regimens may be influenced by the threshold of visual acuity at the start of treatment, the type of diagnosis and compliance to treatment. For example, more intense patching regimes, irrespective of Amblyopia type, should be prescribed for severe Amblyopia in order to achieve at least 1 or more lines of successful visual improvement regardless of the acuity at the start of treatment. The side effects of occlusion are occlusion Amblyopia of the dominant eye, precipitation of strabismus, diplopia, and allergies to skin adhesive patches. Other concern is the cosmetic dissatisfaction associated with patching, impact on quality of life with poorer vision whilst occluding the better eye can affect compliance of patient to the therapy.
1.5.3. Penalisation
Pharmacological Treatment:
Vision therapy:
Vision therapy: Refers to active therapy to improve visual performance by patient’s conscious involvement in a sequence of specific controlled visual tasks. Active vision therapy compensates for anisometropia and its amblyogenic influences, stabilizes central foveal fixation, normalizes visual acuity , monocular skills , occulomotor or accommodative problems and their reaction time. It minimizes spatial distortion, suppression, strabismus and helps in achieving normal binocular function12.
VISION THERAPY SOFTWARE.4 :(VTS4 ) therapy
VTS4 software which works on principle of active vision therapy is a type of computer orthoptic program. First commercially available computerized orthoptic system was available in 1985.The system uses 8-bit microprocessor to present stimuli, analyze response and provide reinforcement. The programs are based upon the research of Jeffery Cooper OD MS FAAO and Jerry Feldman, a psychologist. Together they developed a training protocol using random dot stereogram’s in an operant conditioning paradigm12.( Figure 2).Vision therapy software 4 used in the study(VTS4 ) includes office and home therapy. VTS4 software has various modules dealing with strabismus, phorias and convergence insufficiency and Amblyopia. Amblyopia module of VTS4 is specifically designed to eliminate crowding phenomenon, suppression and promote binocular vision. It is based on principle of neuronal stimulation of cells. Program consists of larger targets during the beginning of session and later on it proceeds to smaller target. It uses the principle of monocular task in binocular field thus more effective than patching for Amblyopia as it promotes the amblyopic eye to view the lines and letters and the other eye (sound eye or less amblyopic eye) to view the background picture12.
Aims &Objectives : To assess the improvement of visual acuity with occlusion therapy and VTS4 therapy.
Primary objective: To assess the better and quicker method of vision improvement and to assess the improvement of binocular vision with both therapies.
Secondary objective: To ensure better quality of vision and to assess the superiority of each therapy over one another.
Material and Methods:
Study population: Pediatric patients of both genders, between age group of 3- 12 years diagnosed with Amblyopia attending to Outpatient department eligible as per the inclusion and exclusion criteria of this study.
Study design: A Hospital Based Randomized Prospective Study.
Study period is from December 2015 to November 2016 including follow up period of six months.
Sample Size: Was estimated by using the Mean Vision between two procedures after treatment. Mean Vision after treatment with Occlusion therapy was 0.15 ± 0.25 . Hence a total of 60 subjects will be included in the study.
Sample Size Estimation Formula:
Sample size = 2SD2(Zα/2+Zβ)2
Patients in each group: Occlusion therapy group and VTS4 therapy group included 26 patients each. These patients were followed up for 3 and 6 months for assessment of improvement of visual acuity and other parameters .Total of 52 patients will be included in the study.
Materials:
Patients attending Outpatient department were examined using torch light, streak retinoscope, Autorefractometer , Slit lamp unit, Slit lamp Biomicroscopy using 90D and 78D lens and indirect ophthalmoscope, Vision Therapy Software (VTS4) and Occluders for treatment.
Inclusion criteria:
- Children between 3- 12years.2.Best corrected Visual acuity of 6/12to 6/60 3.Both male and female patients.4.StrabismicAmblyopia not more than 30 degree of manifest squint.5.Anisometropic Amblyopia ,not more than visual acuity difference of two lines between two eyes.6.Hypermetropia less than 6D.7.Myopia less than 6D.8.Patient with astigmatism of not more than 3D.9.Patients with Ametropic Amblyopia.10.Deprivational Amblyopia: cataract.11.Amblyopa ex anopsia.1Unilateral or bilateral cases.13.Patients willing to participate in the trial.
Exclusion criteria: 1.Patients more than 12 years of age.2.Patients with alternating squint.3.Patients with myopia more than 6D.4.Patients with Hypermetropia of more than 6 D.5.Patients with astigmatism of more than 3D.
Material and Methods:
Tests included for both groups:
Ocular examination:. Direct torch light examination, slit lamp examination for anterior segment examination. Fundus examination using 90D or 78D Slit lamp Biomocroscopy. Indirect ophthalmoscope, Cycloplegic refraction with Retinoscopy, subjective correction or both, assessment of binocularity with titmus fly and Contrast sensitivity with Pelli Robson chart
Protocol for patching: Occlusion therapy: Patching was performed using commercially available patches like Occluders( Figure1). Full correction with spectacles is given and following regimen for patching was followed. Patching till 6 yrs: Patch is placed over the dominant eye one day for each year of the child’s age, then switched to other eye for one day each cycle. Patching in 6- 12 years: alternate day occlusion13.Minimum patching of at least 2 hours in each group irrespective of age with near activities was advised during patching.
Vision therapy software :(VTS4):Therapy includes office therapy and home therapy: Sessions are divided into office therapy and home therapy. Office therapy includes a minimum of 20 minutes exercises daily or on alternate day basis with VTS4for minimum of 15- 20 sittings followed by home therapy which consists of daily 20 min exercise of home therapy. Office therapy is performed using 3D glasses during exercises with refractive error correction. Office sessions are monitored. Home therapy is performed by patching of the sound (dominant eye) with full spectacle correction, done without using the 3D glasses Compact disc installed with patented software is provided to the patient to perform home therapy. .Exercises is performed for 150 sittings and the patient is followed up for the improvement in visual acuity, Contrast sensitivity and Stereopsis. Patients of each group were followed up for 3 and 6 months for visual parameters like Best Corrected Visual Acuity, Stereopsis and Contrast sensitivity and examined at 3 and 6 months interval.
Statistical methods:
Data is entered into Microsoft excel data sheet and was analyzed using SPSS 22 version software. Categorical data are represented in the form of Frequencies and proportions. Chi-square test will be the test of significance. Continuous data will be represented as mean and standard deviation. Independent t test will be the test of significance to identify the mean difference between two groups. Paired t test will be the test of significance for paired date (i.e. before and after treatment). P value<0.05 was considered as statistically significant19.
RESULTS:
Statistical analysis: Data was entered into Microsoft excel data sheet and analyzed using SPSS 22 version software. Categorical data was represented in the form of Frequencies and proportions. Chi-square test was used as test of significance for qualitative data. Continuous data was represented as mean and standard deviation. Independent t test was used as test of significance to identify the mean difference between two quantitative. P value (Probability that the result is true) of <0.05 was considered as statistically significant after assuming all the rules of statistical tests. Statistical software: MS Excel, SPSS version 22 (IBM SPSS Statistics, Somers NY, USA) was used to analyze data.

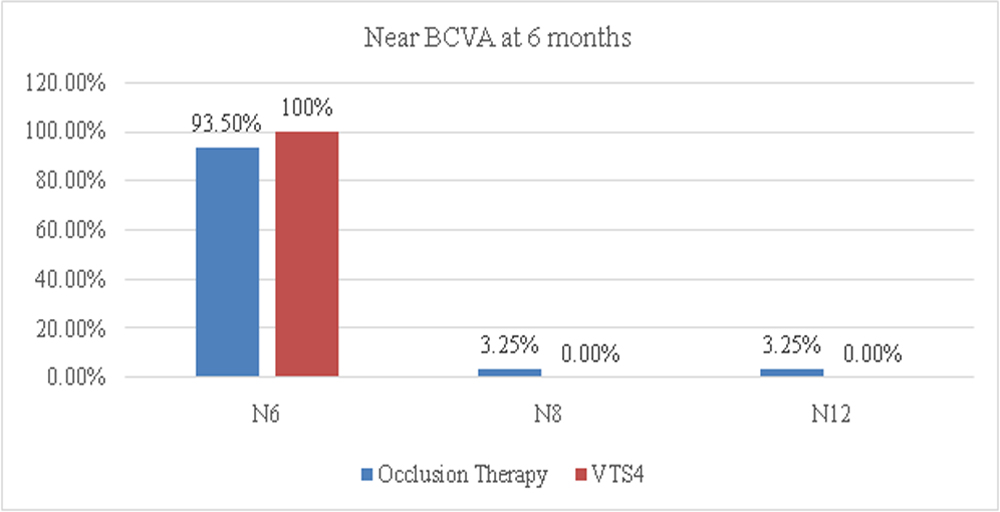
Figure 4 : Bar diagram showing Comparison of Logmar Distant and Near Vision at different Follow up period between the groups and within the groups
χ 2 = 1.104, df = 1, p = 0.295
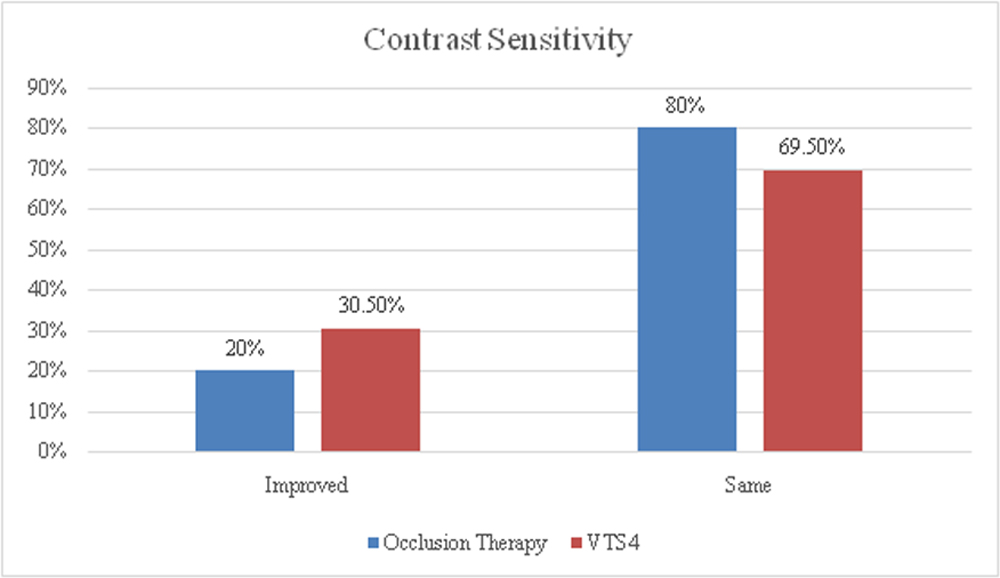
Figure 1.Bar diagram showing Final outcome of Contrast sensitivity between two groups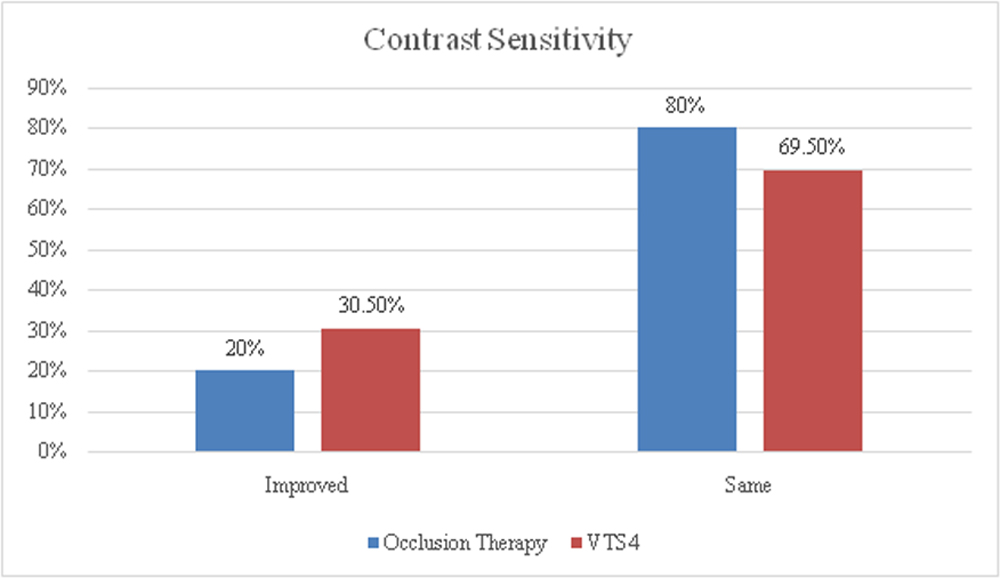
χ 2 = 1.104, df = 1, p = 0.295
Figure 1.Bar diagram showing Final outcome of Contrast sensitivity between two groups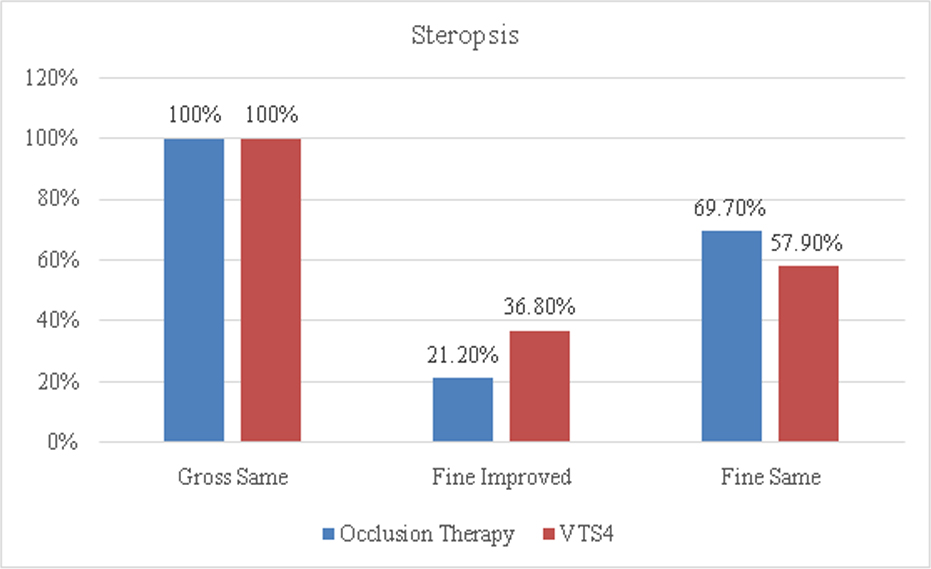
Figure 2. : Bar diagram showing Final outcome of Stereopsis between two groups
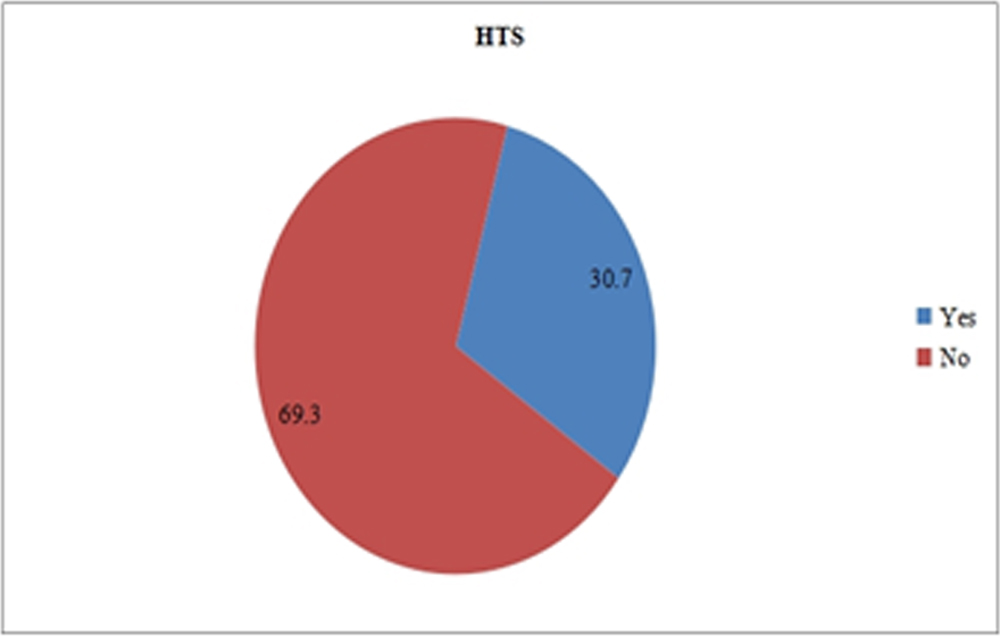
Figure 3: Pie diagram showing HTS among VTS4 group
IDISCUSSION: This is a prospective study of 52 patients diagnosed with Amblyopia in which patient were randomized to occlusion therapy and VTS4 therapy group with added home therapy and 26 patients were included in each group. Majority of patients included in our study were Anisometropic Amblyopia in both groups. According to this study final outcome of BCVA was better in VTS4group ( 93.94%) compared to occlusion group ( 73.1%) and the end of six months, maximum of 3 line improvement and 4 line improvement in occlusion and VTS4therapy group respectively was seen. However, there was no statistically significant difference between two groups.
There was a significant difference in mean Contrast sensitivity between two groups from 1st visit till 6 months follow up. However, in occlusion group there was no significant difference in mean Contrast sensitivity between 1st visit versus 3rd month and between 1st visit and 6 months follow up value, p=0.824. In VTS4group , there was no significant difference in mean Contrast sensitivity in 1st visit and 3rd month values, but there was significant improvement in Contrast sensitivity compared to first visit.. It is observed that improvement in Contrast sensitivity is better in VTS4 group ( 30.5%) as compared to occlusion group but there was no statistically significant difference between two groups (p=0.295). In the study conducted by Sjostrand et al, where Contrast sensitivity was measured pretreatment and post treatment in patients with strabismic and anisometropic Amblyopia after occlusion therapy had shown that pretreatment patient presented with strabismic Amblyopia had better Contrast sensitivity 11.
In this study there was no significant difference in mean fine Stereopsis between two groups from 1st visit till 6 months of follow up. In occlusion group there was no significant difference in mean fine Stereopsis between 1st visit compared to 3rd month but significant improvement was observed between 1st visit and 6 months follow up value. In study conducted by Wallace et al, used Randot Preschool Stereoacuity test to evaluate Stereopsis. It was observed that better baseline stereoacuity was associated with better baseline amblyopic eye acuity( p <0.001).Thus concluded that even if their visual acuity deficit resolves , many children with anisometropic Amblyopia have stereoacuity worse than that of non-amblyopic children of the same age13In VTS4 study group , there was no significant difference in mean fine Stereopsis between 1st visit and 3rd month values , but there was significant improvement in fine Stereopsis at 6 months compared to 1st visit value..Hence it was observed that improvement in fine Stereopsis was better in VTS4( 36.8%) compared to occlusion group( 21.2%),p=0.176.But there was no statistically significant difference between two groups.14,15,16. Observations done in this study showed that VTS4 therapy had a better edge over occlusion in terms of improvement in visual acuity, Contrast sensitivity and fine Stereopsis. Patients with VTS4 therapy showed improvement in these parameters probably due to compliance to the therapy as this involves shorter duration of exercises compared to long hours of patching and more over this therapy works on neuronal stimulation to improve the visual parameters . Since it is computer based games it holds attention of patient to therapy and cosmetically more acceptable to patients especially in the older age groups. Constraints observed in our study in occlusion therapy was compliance to patching which was cosmetically unacceptable to the child especially the older children and social stigma associated with it. Adherence to patching and glasses were the biggest hurdle observed in these patients . Disadvantages of VTS4 therapy observed was that patients had to come to hospital for these exercises with added on travel cost and the cost of the treatment and its availability in tertiary eye care centers. Hence accessibility to patients from small towns is difficult.
Conclusion:
We found in this study that both modalities of treatment had shown improvement in visual acuity and some amount of improvement in Contrast sensitivity and Stereopsis but VTS4 therapy had advantage in terms of acceptance and compliance shown by the patients to therapy. Occlusion therapy basically deals with improvement of vision but other aspects of vision like accommodation, eye movements and suppression were better treated with vision therapy. Patients in VTS4 therapy group were older compared to the occlusion group. One of the issues with patching was the apprehensiveness of older children to patching for daily activities making it cosmetically unacceptable and thus contributing to non-compliance. The duration of the study was short and longer follow up is needed to assess the visual parameters and their maintenance of visual acuity. Longer period of study would help us assess efficacy of VTS4 therapy over occlusion and how long the sessions of therapy has to be continued to prevent recurrence or regression of visual parameters. We report that there was improvement in best corrected visual acuity in VTS4 therapy group compared to occlusion group at the end of 6 months .Improvement in Contrast Sensitivity and fine Stereopsis was seen in both the groups, but better results with VTS4. Children performed these activities easily which is fun based and stigma free. The quality of life is better as the only seeing eye is not patched especially in patients with dense amblyopia. Though occlusion is age old therapy proven for Amblyopia, compliance related issues and longer hours of patching can interfere with the psychosocial growth of the child, hence VTS4 therapy can be considered as a good and safe alternative to patients of older age group and who have accessibility to it.
Limitations Of The Study:1.Shorter duration of study which does not assess regression, recurrence and maintenance of vision with both these therapies.2.There is no prior study available to correlate with the findings of our study.3.VTS4 therapy procedure was not economically feasible for many patients.4.VTS4 therapy is not accessible at all centres.
REFRENCES
1. Von Noorden, GMaumenee A. Von Noorden-Maumenee’s Atlas of strabismus. 1st ed. Saint Louis: C.V. Mosby; 1977.
2. Holmes JClarke M. Amblyopia. The Lancet. 2006; 367(9519):1343-1351.
3. Von Noorden,GCampos E. Binocular vision and ocular motility. 1st ed. St. Louis, Mo.: Mosby; 2002.
4. Ganekal S, Jhanji V, Liang Y, Dorairaj S. Prevalence and Etiology of Amblyopia in Southern India: Results from Screening of School Children Aged 5–15 years. Ophthalmic Epidemiology. 2013;20(4):228-231.
5.Tsiaras W, Pueschel S, Keller C, Curran R, Giesswein S. Amblyopia and visual acuity in children with Down’s syndrome. British Journal of Ophthalmology. 1999;83(10):1112-1114.
6. Black P. Visual disorders associated with cerebral palsy. British Journal of Ophthalmology. 1982;66(1):46-52.
7. De Zárate BR1, Tejedor J. Current concepts in the management of amblyopia. Clin Ophthalmol.2007 Dec;1(4):403-14.
8. Anderson, Justin E. et al. “Opaque Contact Lens Treatment For Older Children With Amblyopia”. Eye & Contact Lens: Science & Clinical Practice 32.2 (2006): 84-87.
9. Chaudhary, Aparajita et al. “A Comparative Study Of The Efficacy Of Part Time Occlusion And Full Time Occlusion Therapy In Moderate And Severe Amblyopia In Children And Factors Influencing The Outcome”. Indian Journal of Clinical and Experimental Ophthalmology.2016. 2(2): 162.
10. Keech, Ronald V, Wanda Ottar, and Linna Zhang. “The Minimum Occlusion Trial for The Treatment Of Amblyopia”. Ophthalmology (2002). 109(12): 2261-2264.
11. Lithander, J and J Sjostrand. “Anisometropic And Strabismic Amblyopia In The Age Group 2 Years And Above: A Prospective Study Of The Results Of Treatment.”. British Journal of Ophthalmology .1991: (75.2) 111-116.
12. Jeffery Copper OD: Vision Therapy Software 4 Manual:Pg34.
13. Agervi P,Kulgelberg U:Ophthalmology.Randomoized evaluation of spectacles plus alternate day occlusion to treat amblyopia.2010.(Feb.);117(2):381-7
14.Wallace DK, Lazar EL, Melia M, Birch EE, Holmes JM, Hopkins KB, Kraker RT, Kulp MT, Pang Y, Repka MX, Tamkins SM, Weise KK; Pediatric Eye Disease Investigator Group.J AAPOS. 2011 Oct;15(5):455-61
15. Li RW, Ngo C, Nguyen J, Levi DM..PLoS Biol. 2011 Aug; 9(8):e1001135.
16. Christina Gambacorta; Samuel Huang; Indu Vedamurthy; Mor Nahum; Jessica Bayliss; Daphne Bavelier; Dennis Levi .Action Video Games as a Treatment of Amblyopia in Children: Journal of Vision August 2014, 14, 665
FIGURES

Fig 1: Occlusion therapy
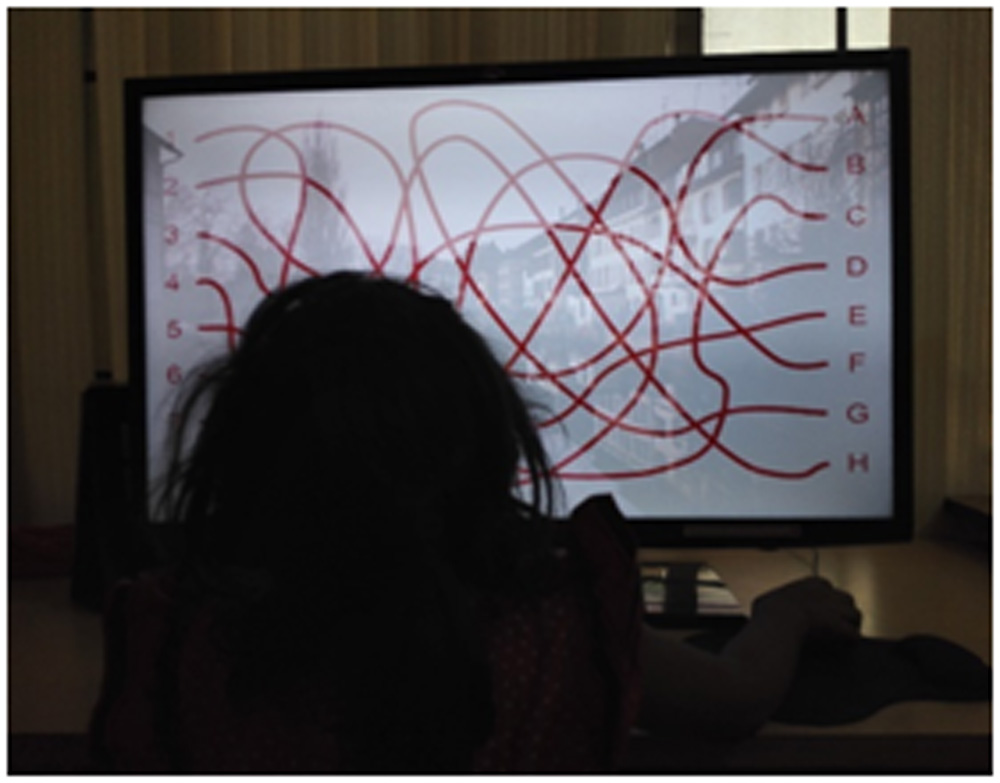

Fig2.VTS4 Therapy
Leave a Comment