
Malik R, Malik VK, Malik KPS
ABSTRACT
Purpose: This study aims at finding the Residual Spherical Refractive Error(RSRE)at 6 weeks after phacoemulsification, optimising the A-Constant in the SRK II formula using the RSRE, & further using the optimised A-Constant in SRK II formula to calculate IOL power to reduce/eliminate RSRE and hence reduce need for spectacles. Methods: This is a Progressive, Interventional study, where 150 cataractous eyes were included. Patients were divided in 2 groups. In Group-A, phacoemulsification was done and RSRE was calculated. A-constant used was 118. Using this RSRE, the pre-operative keratometry andaxial length, a surgeon specific A-Constant was derived. Phacoemulsification was done in Group-B, where IOL power was calculated using optimised A-constant in SRK II formula. The mean RSRE ofGroup-A was compared with that of Group-B, using the unpaired student t-test.
Results: The RSRE for Group-A was -0.2733±0.6879D. Using this RSRE, the new A-Constant for Group-B was 117.35±1.89. The RSRE for Group-B was 0.076±0.2012 D, which is much closer to emmetropia (p<0.0001). At the end of 6 weeks,53.33%, 25.33% and 21.33% patients were found to be Myopic, Emmetropic and Hypermetropic respectively in Group-A, which changed to 12%, 57.33% and 30.6% in Group-B. There was a 33.4% increase in post-operativeemmetropic cases in Group-B, compared to Group-A.
Conclusion: Optimising the A-constant of SRK II formula to get a surgeon specific A-constant is an effective method of reducing the post-operative RSRE, and hence reducing the need for spectacles after surgery.
Keywords: SRK II formula, Phacoemulsification, Outreach camps, Emmetropia, Refractive surprise
INTRODUCTION
Phacoemulsification with intraocular lens (IOL) implantation is the most common ophthalmic surgery performed in clinical practice. Its goal is to restore vision affected by different types of cataract. Postoperative emmetropia is a very important target for both surgeon and patient. Identifying the factors responsible for deviation from postoperative emmetropia and trying to minimize them will improve the quality of postoperative vision and will save the surgeon’s and patient’s efforts(1).
Accurate biometric analysis, selection and calculation of the adequate IOL power, and modern techniques for cataract surgery, all help surgeons to move towards the goal of an emmetropic cataract surgery. However, in spite of all these inputs, residual refractive error still occasionally occurs after cataract surgery(2). The IOL manufacturers suggest a lens-specific value for the A constant as a starting point for IOL calculation. Despite advances in surgical technique and biometry measurement, the post-operative refraction may deviate from the target refraction. (3,4,5).
Constant optimization is the process by which the IOL constant is adjusted to minimize the systematic errors (6).
The SRK (Sanders-Retzlaff-Kraff) formula has been found to be reasonably accurate for eyes with axial lengths between 22mm and 24.5mm. The SRK II was introduced for eyes that were outside this length bracket and is a modification of the original SRK formula with the addition of a correction factor that increases the lens power in short eyes and decreases it in long eyes covering >75% eyes(7).
With modern optical biometry for the majority of patients, informed formula choice and intraocular lens (IOL) constant optimization, outcomes of more than 90% patients within ±1 D and more than 60% patients within ±0.5 D of target are achievable. (8)
The purpose of this study was to find out the Residual Spherical Refractive Error (RSRE) after phacoemulsification surgery, to further optimize the A constant of SRK II formula using the Residual Spherical Refractive Error, and to ultimately use the optimised A-constant to calculate PCIOL power to eliminate/reduce RSRE in an attempt to reduce the need for spectacles after cataract surgery in outreach camps.
METHODS
The study was a prospective, interventional study, including 150 eyes of 150 patients coming to the eye OPD of ChhatrapatiShivajiSubharti hospital, willing to undergo cataract surgery.
This study examines the effect of Axial Length (AL) and average preoperative Keratometry (K) on the A constant using a cohort of cataract surgery patients.
The patients were divided into 2 groups, namely, Group-A (Study group) comprising 75 patients and Group-B (Test Group) comprising 75 patients.
In Group-A, biometry was done using the TOPCON KR 8800 (Itabashi, Tokyo, Japan) and PacScan plus (300AP+ by SONOMED) [Sonomed Escalon, Lake Success, NY, USA] to calculate the power of an IOL, theoretically resulting in emmetropia by a single resident, hence eliminating observer bias. The IOL calculation formula used was SRK II, which is same as used routinely in our OPD.Phacoemulsification was performed by only one surgeon, hence, eliminating surgeon bias.
Only one type of IOL (PMMA; A-Constant 118) was used, thus eliminating different IOL design as a possible source of difference in residual refractive error.
In our setup, IOLs are available only in whole numbers or in denominations of 0.5 (20D, 20.5D, 21D and so on), hence if the calculated IOL power was not a whole number or a denomination of 0.5, it was rounded off to the nearest whole number or 0.5 denomination, and the difference was added/subtracted mathematically from the residual spherical refractive error post operatively.
Patients with senile/pre-senile cataract and Best Corrected Visual Acuity (BCVA) ≤ 6/36 were included. Patients having BCVA≥ 6/24, irregular corneas, congenital abnormalities, co-morbid retinal pathologies, previous intra-ocular surgeries, amblyopia, nystagmus or strabismus were excluded.
Post-operative RSRE was determined for each patient by manual refraction. This too, was done by a single resident to avoid any bias.Using the IOL constant calculation chart by Dr. Hill (9), an optimized A-constant was determined, using pre-op keratometry (K1, K2), pre-op axial length and post-operative RSRE.
In Group-B, Phacoemulsification was carried out similar to Group-A , except that the IOL power was calculated by using SRK II formula with the optimised A constant.Post-operative refractive error was seen and compared with Group-A.
Patients were called for follow up at 1, 2, 4 and 6 weeks post operatively. At each follow up, manual refraction was done to conclude the refraction. For both groups A and B, the refraction at the end of 6 weeks was considered stable and final.
Residual spherical refractive error in Group-A and B was compared statistically using the unpaired student t-test and significance level was set as p<0.05.
RESULTS
In our study, a total of 150 eyes of 150 patients were divided equally in two groups, A & B. No drop-outs were seen. Table 1 highlights the demographics of our study. 58.66% (44/75)patients in Group-A and 53.33% (40/75) patients in Group-B were male. 41.33% (31/75) patients in Group-A and 46.66% (35/75) patients in Group-B were female. A male predominance was seen in both our study groups.
TABLE 1 – Demographics
| SEX (M/F) | MEAN AGE (YEARS) | |
| GROUP A | 44/31 | 62.16 ± 13.24 |
| GROUP B | 40/35 | 65.18 ± 12.59 |
The mean age in Group-A was 62.16 ± 13.24 years, while it was 65.18 ± 12.59 years in Group-B. The mean age was slightly higher in Group-B, compared to Group-A.
In both Group-A and B, most of the axial lengths were in the 23 – 24.5 mm bracket, ie, 35 (46.66%) in Group-A and 31 (41.33%) in Group-B.The second majority was seen in the 22-23 mm bracket, ie, 23 (30.66%) in Group-A and 26 (34.66%) in Group-B. 12% and 21.33% patients were observed in the 21-22 mm bracket in Group-A and B respectively. A very small proportion of eyes were observed in the 20-21 and >24.5mm bracket. No axial length was recorded to be less than 20 mm, in either groups. Mean was 22.91 ± 1.0362 mm in Group-A, and 22.83 ± 0.8459 mm in Group-B. The mean was marginally higher in
Group-A.
The mean of K1 (Horizontal Corneal curvature) in Group-A was 44.25 ± 1.7195 D, and 43.31 ± 1.3405 D in Group-B. The mean of K2 (Vertical Cornel curvature) in Group-A was 43.75 ± 1.7756 D and 42.19 ± 1.5974 D in Group-B. We observed that in both our study groups, an against the rule astigmatism was found, as seen by K1>K2 in both the groups.
The new ‘Surgeon Specific’ A-Constant that was calculated using the RSRE (at the end of 6 weeks from patients of Group-A), the pre-operative axial lengths and keratometry reading was 117.35 ± 1.88.The modified A constant varied between 108.44 to 119.16.This new A-Constant (Mean=117.35) was used to calculate the IOL power in Group-B.
Figure 1 shows the post op refractive status of the eye, in group-A and B. We considered the eye to be Myopic if the RSRE at the end of 6 weeks was < 0 D,Emmetropic if the RSRE was 0 D, and Hypermetropic if the RSRE was > 0 D.
FIGURE 1 – Post-Operative Refractive Status
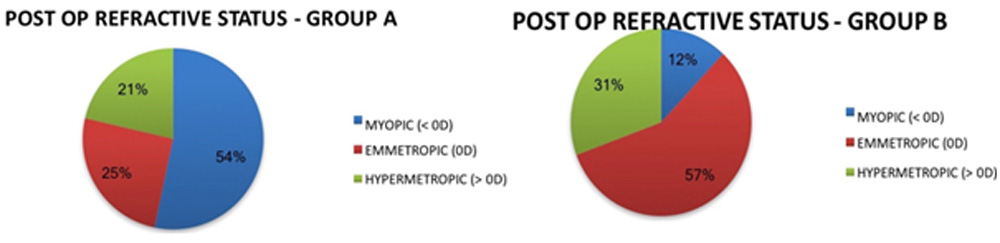
40 (53.33%) patients were left Myopic in Group-A, as compared to only 9 (12%) in Group-B.19 (25.33%) attained a Spherical Emmetropic state in Group-A, compared to 43 (57.33%) in Group-B.16 (21.33%) were left Hypermetropic in Group-A, which increased to 23 (30.6 %) in Group-B.
Table 2 demonstrates the RSRE observed in both the groups at each follow-up. The range of RSRE in Group-A was the same over the 6 post-operative weeks, ie, from -3.50 D to 0.75 D.The Mean RSRE at the end of the 1st post-operative week was -0.2768 ± 0.6555 D. The mean, however, increased in the 2nd week and stayed the same till the end of the 6th week, ie, -0.2733 ± 0.6879 D. The RSRE at the end of week 1 in Group-B ranged between -1 to 1.25 D. This range shifted slightly to -0.75 to 1 D at the end of the 2nd week and hence remained the same till the end of the 6Th week.
TABLE 2- Comparing the RSRE of Group A and B
| GROUP A | GROUP B | ||||
| MEAN (D) | STD. DEV. | MEAN (D) | STD. DEV. | P – VALUE | |
| WEEK 1 | -0.2768 | 0.6555 | 0.0833 | 0.2973 | <0.0001 |
| WEEK 2 | -0.2733 | 0.6879 | 0.0933 | 0.2687 | <0.0001 |
| WEEK 4 | -0.2733 | 0.6879 | 0.0833 | 0.2674 | <0.0001 |
| WEEK 6 | -0.2733 | 0.6879 | 0.0833 | 0.2674 | <0.0001 |
The mean RSRE at the end of 1st week was observed to be 0.0833 ± 0.2973 D. This mean increased slightly to 0.0933 ± 0.2687 D at the end of the 2nd week, but, it again dropped to 0.0833 ± 0.2674 at the end of the 4th week and stayed the same till the end of the 6th week.On comparing the RSRE of Group-A with that of Group-B, we observed that the difference was statistically significant after each of Week 1, 2, 4 and 6 ie p < 0.0001.
FIGURE 2 – Distribution of patients according to RSRE (at 6 weeks) in Group A and B
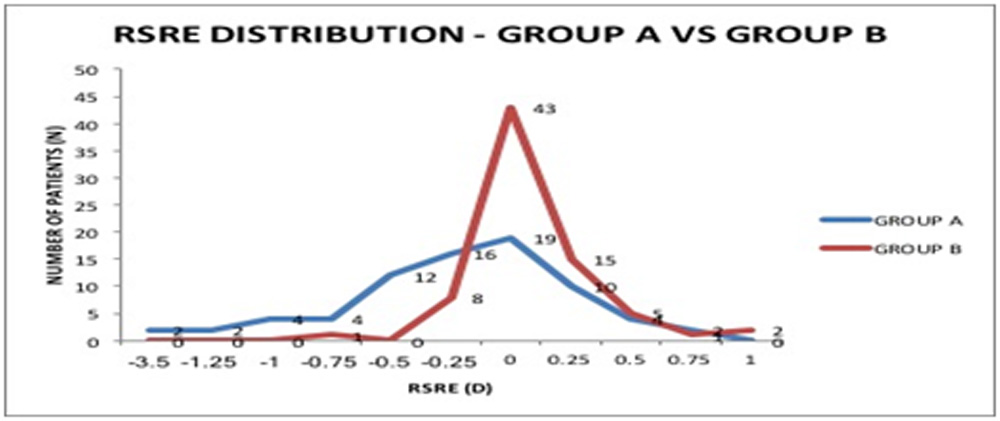
Figure 2 compares the distribution of patients according to RSRE at the end of 6 weeks post-op in Group-A with that of Group-B.In group-A, 19 (25.33%) patients were emmetropic. As discussed above, 40 (53.33%) patients were left Myopic. They were distributed as follows: 2 (2.66%), 2 (2.66%), 4 (5.33%),
4 (5.33%), 12 (16%) and 16 (21.33%) had an RSRE of -3.5, -1.25, -1, -0.75, -0.5 and -0.25 D respectively. 16 (21.33%) patients were left hypermetropes and were distributed as follows: 10 (13.33%), 4 (4.33%) and 2 (2.66%) patients had an RSRE of 0.25. 0.5 and 0.75 D respectively.In group-B, majority of the patientsie, 43 (57.33%) patients wereemmetropic. As discussed above, 9 (12%) patients were left Myopic. They were distributed as follows: 1 (1.33%) and 8 (10.66%) had an RSRE of -0.75 and -0.25 DS respectively.23 (30.66%) patients were left hypermetropic and were distributed as follows: 15 (20%), 5 (6.66%), 1 (1.33%) and 2 (2.66%) patients had an RSRE of 0.25. 0.5, 0.75 and 1 D respectively.
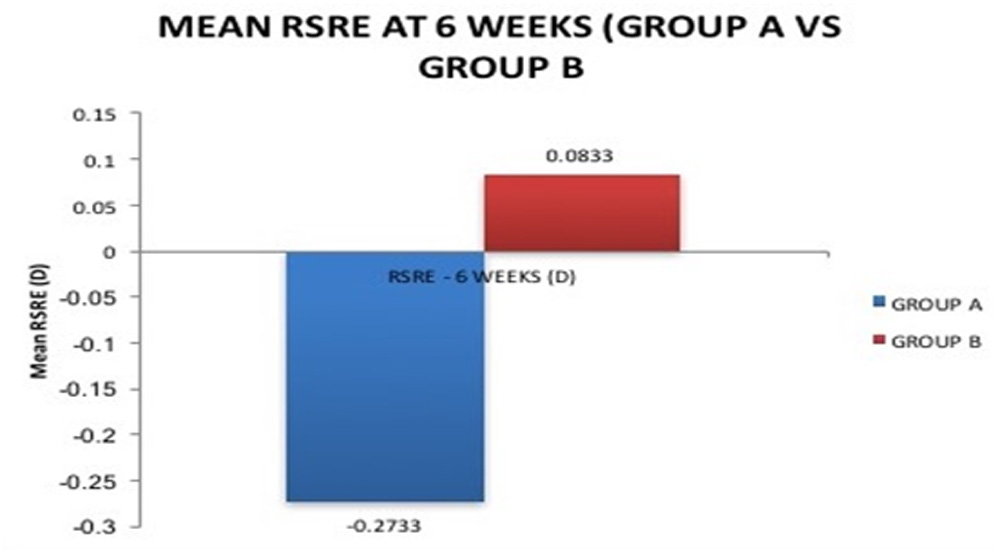
We considered the RSRE at 6th week as final, hence, on comparing Group-A (-0.2733 D) with Group-B (0.0833 D) (Figure 3), we found a shift of mean RSRE closer to emmetropia. This difference was considered extremely statistically significant as shown by the P-value (<0.0001).
FIGURE 3 – Mean RSRE at 6 Weeks
DISCUSSION
This was a prospective, interventional study wherein we aimed at observing the Residual Spherical refractive error (RSRE) after Phacoemulsification, and using that to modify the A-Constant in the SRK – II formula. The ultimate goal was to eliminate/reduce the RSRE, by using the modified A-Constant in the SRK II formula.Studies by Gogate(10)&Gurung(11) & deducted that phacoemulsification gave better uncorrected visual acuity in their study population at the end of 6 weeks.We chose phacoemulsification over SICS, with the aim of keeping thepost operative refractive error to a minimum.We tried to remove as many sources of error and bias possible. All biometric readings were taken by a single resident, hence, eliminating observer bias.Only one experienced surgeon performed all phacoemulsification surgeries, and all cases were uneventful, with successful in-the-bag placement of the PCIOL.Only one type of PCIOL was used in all the cases.Nick(12) postulated that an inadvertent placement of the IOL in the sulcus will cause a 0.75 D myopic shift.
In our study, 58.66% and 53.33% patients were male in Group-A and B respectively.41.33%, 46.66% patients were female in Group-A and B respectively. There was a clear male predominance.
The mean age in Group-A was 62.16 ± 13.24 years, and 65.18 ± 12.59 years in Group-B. The difference in ages of the two groups was insignificant as seen by the p value, which was 0.1544 (>0.05).
In majority of patients, the axial lengths in both Group-A and B were within the 23 -24.5 mm range, namely 46.66% in Group-A and 41.33% in Group-B. The mean axial length from our study was 22.91 ± 1.0362 mm in Group-A, and 22.83 ± 0.8459 mm in Group-B. Our findings resembled the findings of Nangia V et al(13), who conducted an observational study on ocular axial lengths. The mean axial length in their study was 22.6 ± 0.91 mm.
Regarding astigmatism, and prevalent keratometry readings, the mean of K1 in Group-A was 44.25 ± 1.7195 D and 43.31 ± 1.3405 D in Group-B. The mean of K2 in Group-A was 43.75 ± 1.7756 D and 42.19 ± 1.5974 D in Group-B. Both groups showed against the rule (ATR) astigmatism, since K1>K2 in both the groups.
In our routine setup (Group-A), more than half of the patients being operated for cataract surgery were being left Myopic, ie53.33% of patients undergoing cataract surgery had a RSRE of <0 D after 6 weeks of surgery. Similarly, 21.33% were Hypermetropic (RSRE >0 D). Hence in all 74.66% patients were Ammetropic after routine cataract surgery and only 25.33% patients were Emmetropic (0DS). The high number of myopes noted were attributed to variability in the corneal compression while calculating the axial length using the contact A-Scan. This was in agreement to the findings of Schelenz J(14), who too concluded that the contact technique yielded shorter measuring values than the immersion technique.Snead et al(15), also concluded that the present tendency towards unpredicted postoperative myopia points towards the measured axial length being slightly shorter than the actual value. This was attributed to corneal indentation caused by a solid tipped A-Scan probe.
Jorge L(16) stated that during the postoperative healing process, an anterior movement of the IOL in the bag resulting from capsular fibrosis and contraction, can lead to myopic shifts in spherical equivalent of 0.70 DS from 1 day postoperatively up to 2 months. This could also be a possible cause of RSRE.
Holladay JT(17) found that axial length was the greatest contributor to improved IOL power predictabilities. However in Group-B, ie after modification of the A constant, 12% patients were left Myopic (RSRE <0DS) after 6 weeks of surgery, 30.6% were Hypermetropic and 57.33% patients were Emmetropic.
Comparing the two groups, the proportion of myopes had significantly fallen, from 53.33% to 12%, while the proportion of spherical emmetropes had significantly increased from 25.33% to 57.33%. However, the number of hypermetropes had slightly increased from 21.33% to 30.6%.
These findings were in agreement with R Sheard(8) and Snead et al.(15), who found that IOL constant optimisation has been shown to improve substantially prediction accuracy for contact ultrasound A-Scan (from 79.7 to 82.5% within ± 1 D). HoweverAristodemou P et al(3) refuted our findings by concluding that optimizing IOL constants for IOLMaster biometry substantially improved refractive outcomes, far exceeding any additional benefit of personalizing IOL constants for individual surgeons.
The RSRE in Group-A ranged from (-3.5D) to (+0.75D). The Mean at the end of the 1st week was -0.2768 ± 0.6555 D, and it changed to -0.2733 ± 0.6879 D at the end of the 2nd, 4th and 6th week. On plotting the RSRE of Group-A at the 6th week, linearly, we found an increasing trend. All the patients in Group-A were implanted with the same type of IOL, which had an A-Constant of 118.Using the RSRE, Pre-Operative Axial length and Keratometry, a modified A-Constant was calculated using the online chart made by Dr. Warren E. Hill(9).We used a method similar to Holladay(18), who used the postoperative stabilized refraction, dioptric power of the implanted IOL, the preoperative corneal and Axial length measurements to calculate the personalized ‘Surgeon Factor’, and then the improved formula was tested by comparing it with the then currently used formulae.
The modified Surgeon Specific A-Constant that was calculated, ranged from 108.44 – 119.16, with a mean of 117.35 ± 1.88. The mean Axial Length in Group-A was 22.91 mm, while that for Group-B was 22.83 mm. Merriam JC (19) postulated that the A constant for longer eyes with flatter corneas is larger than the A constant for shorter eyes with steeper corneas.
Our findings were similar to their postulation. A slightly smaller mean axial length in Group-B was associated with a smaller axial length.The RSRE in Group-B ranged from -1 to 1.25 D at the end of week 1 and from -0.75 to 1 DS at the end of the 2nd, 4th and the 6th week. The mean RSRE at the end of the 1st week was observed to be 0.0833 ± 0.2973 D. This mean increased slightly to 0.0933 ± 0.2687 D at the end of the 2nd week, but it again dropped to 0.0833 ± 0.2674 D at the end of the 4th week and stayed the same till the end of the 6th week.
Our results of using the modified A-Constant were better than those observed by MS Dang(20). When % of eyes with 1D error was considered, they observed that the original SRK II had a 78% accuracy. The modified SRK II formula improved these statistics to 80%. The results of our study showed that 100% of patients in Group-B, ie group with modified SRK II formula had a RSRE within ±1D.The change of RSREat the end of the 4th and the 6th week was from -0.2733 ± 0.6879 D in Group-A to 0.0833 ± 0.2674 in Group-B. The RSRE had thus moved towards emmetropiaie the amount of ammetropia had decreased.This change at the end of the 1st, 2nd, 4th and 6th week was statistically significant (p < 0.0001) as calculated by the unpaired student t-test.
Gunnar H(21) concluded that the use of modified A constant in SRK II formula resulted in statistically significant reduction in mean refractive error (p<0.001).We noted that the mean RSRE at the end of 6th week was myopic in Group-A and this changed to a slight hypermetropia.Conversely, Petermeier K(22) did not prefer using the SRK II formula as it led to higher post op residual refractive error compared to other formulae.
On plotting the distribution of RSRE in Group-A and Group-B together, we noted that, the range had been significantly reduced, ie from (-3.5) – 0.75 D in Group-A to (-0.75) – 1 D in Group-B.The percentage of cases with post-operative emmetropia had jumped from 25.33% in Group-A to 57.33% in Group-B, a more than double leap in numbers.Also the mean RSRE at 6 weeks in Group-B (0.0833 D) was much closer to emmetropia than in Group-A (-0.2733 D).
CONCLUSION
We conclude from our study that SRK II formula without A-Constant modification was therefore ineffective in providing postoperative emmetropia. Constant optimization helped in bringing the mean postoperative RSRE closer to emmetropiaand also helped in significantly increasing the number of cases with postoperative emmetropia.
Hence in a developing and overpopulated country like India especially in a setup like ours, where patients belong mostly to the rural population,and usually do not turn up for regular follow ups, it is necessary to try and leave the patients emmetropic, and hence reduce the need for spectacles after cataract surgery.
Constant optimization is a cheap, effective and convenient method to decrease /eliminate the postoperative RSRE and should be employed in all setups that still use the contact method of A-Scan for axial length estimation.
REFERENCES
- Rasheed A. Aiming for Emmetropia after cataract surgery. Iraqi Postgraduate Medical Journal. 2013;12(16088360): 721-26.
- Behndig A, Montan P, Stenevi U, Kugelberg M, Zetterström C, Lundström M. Aiming for emmetropia after cataract surgery: Swedish National Cataract Register study. Journal of Cataract & Refractive Surgery. 2012;38(7):1181-1186.
- Aristodemou P, Knox Cartwright N, Sparrow J, Johnston R. Intraocular lens formula constant optimization and partial coherence interferometry biometry: Refractive outcomes in 8108 eyes after cataract surgery. Journal of Cataract & Refractive Surgery. 2011;37(1):50-62.
- Ladas J, Stark W. Improving Cataract Surgery Refractive Outcomes. Ophthalmology. 2011;118(9):1699-1700.
- Merriam J, Zheng L, Merriam J, Zaider M, Lindström B. The effect of incisions for cataract on corneal curvature. Ophthalmology. 2003;110(9):1807-1813.
- Olsen T. Improved accuracy of intraocular lens power calculation with the Zeiss IOLMaster. ActaOphthalmologicaScandinavica. 2006;85(1):84-87.
- IOL: Power calculation & selection. [Internet]. 2017 [cited 17 August 2017]. Available from: https://rajswasthya.nic.in/RHSDP%20Training%20Modules/Ophthalmologist/Cataract%20Surgery%20with%20IOL.Pdf/03%20IOL%20calculation.pdf
- Sheard R. Optimising biometry for best outcomes in cataract surgery. Eye. 2013;28(2):118-125.
- Warren E. Initial IOL constant calculation sheet. [Internet]. [Place unknown]: East valley ophthalmology. Doctor-hill.com. 2017 [cited 17 August 2017]. Available from: https://www.doctor-hill.com/physicians/docs/4-IOL-constants.xls
- Gogate P, Kulkarni S, Krishnaiah S, Deshpande R, Joshi S, Palimkar A et al. Safety and Efficacy of Phacoemulsification Compared with Manual Small-Incision Cataract Surgery by a Randomized Controlled Clinical Trial: Six-Week Results. Ophthalmology. 2005;112(5):869-874.
- Gurung A, Karki D, Shrestha S, Rijal A. Visual outcome of conventional extracapsular cataract extraction with posterior chamber intraocular lens implantation versus manual small-incision cataract surgery. Nepalese Journal of Ophthalmology. 2010;1(1).
- Astbury N, Ramamurthy B. How to avoid mistakes in biometry. Community Eye Health. 2006;19(60):70-71.
- Nangia V, Jonas J, Sinha A, Matin A, Kulkarni M, Panda-Jonas S. Ocular Axial Length and Its Associations in an Adult Population of Central Rural India: The Central India Eye and Medical Study. Ophthalmology. 2010;117(7):1360-1366.
- Schelenz J, Kammann J. Comparison of contact and immersion techniques for axial length measurement and implant power calculation. Journal of Cataract & Refractive Surgery. 1989;15(4):425-428.
- Snead M, Rubinstein M, Lea S, Chopdar A. Calculated versus A-scan result for axial length using different types of ultrasound probe tip. Eye. 1990;4(5):718-722.
- Alio J, Abdelghany A, Fernández-Buenaga R. Management of residual refractive error after cataract surgery. Current Opinion in Ophthalmology. 2014;25(4):291-297.
- Holladay J, Prager T, Ruiz R, Lewis J, Rosenthal H. Improving the Predictability of Intraocular Lens Power Calculations. Archives of Ophthalmology. 1986;104(4):539-541.
- Holladay J, Musgrove K, Prager T, Lewis J, Chandler T, Ruiz R. A three-part system for refining intraocular lens power calculations. Journal of Cataract & Refractive Surgery. 1988;14(1):17-24.
- Merriam J, Nong E, Zheng L, Stohl M. Optimization of the A Constant for the SRK/T Formula. Open Journal of Ophthalmology. 2015; 05(03):108-114.
- Dang M, Raj P. SRK II formula in the calculation of intraocular lens power. British Journal of Ophthalmology. 1989;73(10):823-826.
- Høvding G, Natvik C, Sletteberg O. The refractive error after implantation of a posterior chamber intraocular lens. The accuracy of IOL power calculation in a hospital practice. ActaOphthalmologica. 1994 Oct;72(5):612-6.
- Petermeier K, Gekeler F, Messias A, Spitzer M, Haigis W, Szurman P. Intraocular lens power calculation and optimized constants for highly myopic eyes. Journal of Cataract & Refractive Surgery. 2009;35(9):1575-1581.
Leave a Comment