
![]()
Dr. Anshulee Sood, S17183, Dr. Sahithya Bhaskaran, Dr. Shashikant Shetty, Dr. P. Vijayalakshmi
ABSTRACT
AIM
To assess neuro-ophthalmological diseases in professional drivers which can prove hazardous to the individual as well as the public.
METHODS
Retrospective data of 38 professional drivers referred to the neuro-ophthalmology department was reviewed and assessed.
RESULTS
Out of 38, 13 patients were found to have visually disabling ocular pathology which can prove to be dangerous while driving.
CONCLUSION
The study gives an insight to the fact that we need a thorough knowledge, examination standards, protocols and better co-ordination among Physician, Ophthalmologists and the State to determine whether an individual is functionally fit to drive or not.
INTRODUCTION
The decision to recommend a license for driving is an important one. It equates to freedom, independence and in many cases economic livelihood for the patient. But if the recommendation is based on an incorrect assessment, it may prove hazardous to the individual as well as it may compromise public safety. Neurological disorders can compromise a person’s driving fitness. However, the complexity of these disorders – and the subjective nature of evaluations – can make determining driving fitness difficult.
As an Ophthalmologist, we need to be more vigilant as many visually disabling diseases can be easily missed in a routine ophthalmological examination. Unfortunately, there seems to be little consensus among health professionals, driving experts, and state government on how to advise these individuals. Despite being an issue of such massive impact, there are very few studies addressing the need for an elaborative workup before issuance of driving license. The aim of this study was to have an insight on the ocular status of the professional drivers, who, if given a driving license without proper assessment and regular review, can pose a serious public health problem.
METHODS AND MATERIALS
This is a single centre retrospective study which included professional drivers by purposive sampling who came to the outpatient department of Aravind Eye Hospital, Madurai for ophthalmological check-up either for issuance or renewal of driving license or with some other symptom in a period of 3 months i.e. January to March 2017.
All patients received a comprehensive ocular examination which included Best corrected visual acuity, Intra-ocular pressure (by non-contact tonometer), Binocular Single Vision (by Worth four dot test), Colour vision (by Ishihara plates), central fields (by Bjerrum tangent screen), slit lamp examination of anterior segment and fundus examination (by 90 D lens). Out of these, the patients who had specific ocular pathology were referred accordingly to various speciality clinics. We further analysed the data of the patients who were referred to neuro-ophthalmological department. There were 38 such patients who underwent further examinations and investigations based on their symptoms and findings of initial examination.
RESULTS
Out of a total of 2677 professional drivers who came to the OPD, 38 were referred to the neuro ophthalmological department of Aravind Eye Hospital, Madurai.
All 38 drivers were males. The mean age of the drivers was 48.29 ± 7.37 years.
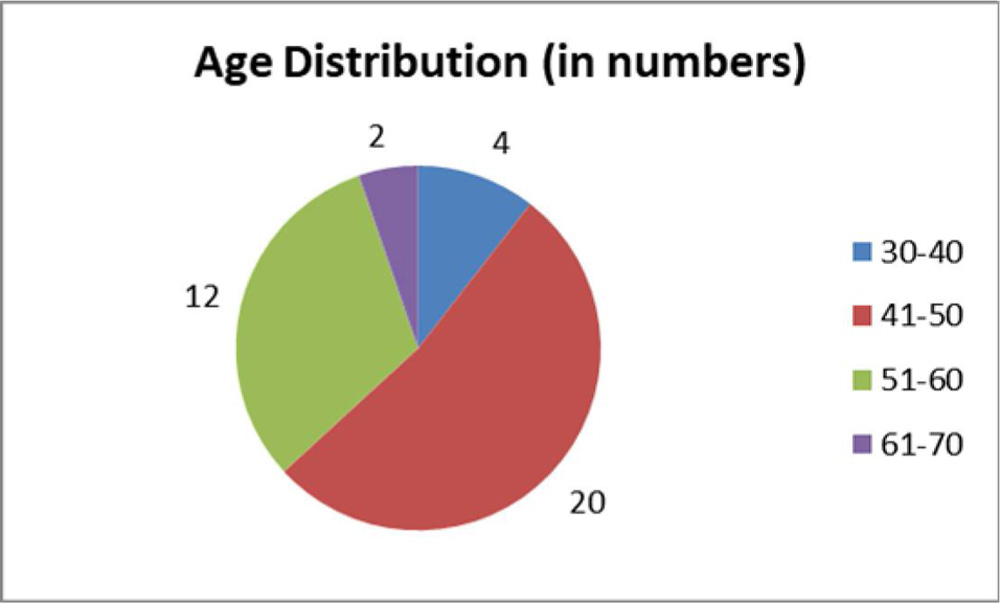 Figure 1. Pie chart representing age distribution among the drivers
Figure 1. Pie chart representing age distribution among the drivers
Symptomatology
| Presenting complaints | Number |
| Sudden decrease of vision/field | 7 |
| Intermittent squinting | 1 |
| Drooping eyelids | 1 |
| Diplopia | 1 |
| Glare | 1 |
| Issuance /Renewal of license | 27 |
Table 1: Number of drivers presenting with specific complaints
Out of these, 13 patients were found to have ocular pathology which can prove to be hazardous while driving.
| Chief complaint | BCVA | CV | CF | BSV | Diagnosis | Systemic Co-morbidity | Special investigations | ||
| RE | LE | ||||||||
| 1 | Sudden defective vision | 6/60 | 6/60 | D | N | + | BE Toxic neuropathy (Ethambutol) | TB | MRI- Non compressive optic neuropathy
VEP- Prolonged P100 latency |
| 2 | Intermittent squinting | 6/6 | 6/6 | N | N | + | Ocular Myasthenia | Nil | Ice Pack test +ve |
| 3 | Drooping of lids | 6/6 | 6/6 | N | N | + | Ocular Myasthenia | DM | Ice Pack test +ve |
| 4 | License renewal | 6/9 | 1/60 | N | LE Peripheral constriction * | + | LE Aphakia | DM
HTN |
Nil |
| 5 | Diplopia on left gaze | 6/6 | 6/6 | N | N | Diplopia | Left LR palsy | DM
HTN |
Nil |
| 6 | Defective Field of vision | 6/6 | 6/9p | N | Right
Homonymous Hemianopia ** |
+ | Right
Homonymous Hemianopia |
HTN
IHD |
CT Brain- Sub acute lacunar infarct in optic radiation |
| 7 | Sudden defective vision, trauma | 5/60 | 6/6 | D | D | + | Traumatic optic neuropathy | Nil | CT orbits- Intraconal hematoma |
| 8 | License issuance | 6/6 | 3/60 | N | N | Left suppression | Left High Myopia, Anisometropic amblyopia | Nil | Nil |
| 9 | Glare | 6/6 | 6/60 | N | N | + | LE corneal scar with ALC tear | Nil | Nil |
| 10 | Inability to move hand to a specific object | 6/18 | 6/36 | N | D | + | Optic Ataxia | DM
HTN IHD |
MRI Brain- B/L Occipito-parietal infarct |
| 11 | Sudden defective vision | 2/60 | 6/6 | D | D | + | Optic Neuritis (Multiple Sclerosis) | Nil | MRI-Brain- Paraventricular demyelinating plaque |
| 12 | Sudden defective vision | HM | 6/6 | D | D | NA | NAION | DM | Nil |
| 13 | Sudden defective vision | 6/6 | 1/60 | D | D | NA | NAION | HTN | Nil |
Table 2: Case-wise details. N: Normal, D: Defective, NA: Not Assessable, +:Present, DM: Diabetes Mellitus, HTN: Hypertension, IHD: Ischemic Heart Disease.* without glass ** with HFA
DISCUSSION
DISCUSSION
In our study, we specifically report the incidence of neuro-ophthalmological diseases in professional drivers. We believe that as compared to ocular diseases like glaucoma, diabetic retinopathy which receive wide awareness and frequent screening camps, neuro-ophthalmological disorders are hardly screened for or recognised. But the symptoms caused by these diseases like diplopia can prove to be very dangerous while driving.
Several studies have concluded that there is no significant association between eye diseases like cataract, glaucoma, macular degeneration, diabetic retinopathy and motor vehicle collision involvement rates1,2,3,4. However, the neurological impairment (multiple sclerosis, Parkinson disease or a stroke) is associated with increased risk for all types of road accidents1,2,4.
In India, there are no well-defined rules for the practitioner in the contentious issue of reporting unsafe drivers to a public health authority. In our study, we report 13 such patients with ocular pathology which can severely impair driving function. Shouldn’t there be mandatory reporting laws for any unsafe driver with a pathology that can risk the life of the individual as well as the public? The practitioner may be conflicted in a situation where he or she suspects the individual is driving against advice.5 However, there are several concerns that need to be addressed regarding reporting, particularly involving trust between physician and patient. Whether to violate the trust that is an essential and moral feature of the doctor-patient relationship or to protect the society from risk of serious harm is a sensitive issue.
The ethical shades of grey become even more blurred in instances where the reporting means snatching the livelihood from an individual even though he is not involved in a direct crime. Adequate compensation for lost working days or rehabilitation should be available to drivers who suffer from ocular disorders that restrict them from driving. This will not only aid in increasing the involvement of a physician but also encourage the self-reporting to the licensing bureau by the drivers of their disabilities.
Also, in a country like India, where mandatory reporting is not required, there is little protection for the doctor who chooses to report any such event out of concerns for public safety. Perhaps anonymous reporting or legal protection of the reporting physician could help the situation as concerns over the potential for litigation likely leads to underreporting to authorities.
Various manifestations of vision impairment have been identified that place older drivers at higher risk for accidents, most notably including severe visual-field loss and a restricted useful field of view (UFOV).6,7 Some research suggests that diabetes8 or anti-diabetic medication use9 is associated with an increased motor vehicle collision risk, while other studies have documented increased accident involvement among those with heart disease10 or those with greater orthostatic systolic blood pressure drop.11
In our study, we observed that the incidence of neurological diseases was more in the age group above 50 and in patients with associated co-morbidities like diabetes, hypertension, ischemic heart disease etc. These middle aged drivers with possibilities of co morbidities can have any acquired ocular disease at any point of their driving career. The licencing bureau should take these facts into consideration and hence, the follow up and the time interval for renewal of licence should be customised for drivers based on their age and systemic profile.
Both primary care and subspecialty physicians often lack basic knowledge and formal training to make a recommendation on who can safely operate a motor vehicle12. Furthermore, despite published guidelines for assessing driving competency, many physicians are often unaware of the laws in their state13. Certifying physicians should be adequately trained to assess the fitness based on rules and regulations of their region.
Furthermore, all health care reports should be available to every treating surgeon or physician so as to enable a tailored assessment for every person.
The limitation of this study includes small sample size and time period. However, the aim of the study is to give an insight to the fact that we need a thorough knowledge, examination standards and protocols and better co-ordination among physician, ophthalmologists and the state to determine whether an individual is functionally fit to drive or not.
BIBLIOGRAPHY
- Sims RV, McGwin G Jr, Allman RM, et al. Exploratory study of incident vehicle crashes among older drivers. J Geron 2000;55:22–7M.
- McGwin G Jr, Sims RV, Pulley L, et al. Relations among chronic medical conditions, medications, and automobile crashes in the elderly: a population-based case-control study. Am J Epidemiol 2000;152:424–31.
- Margolis KL, Kerani RP, McGovern P, et al. Risk factors for motor vehicle crashes in older women. J Geront 2002;57A:186–91M.
- Cross JM, McGwin G, Rubin GS, et al Visual and medical risk factors for motor vehicle collision involvement among older drivers British Journal of Ophthalmology 2009;93:400-404.
- Steven H. Yale, et al. Neurologic Conditions: Assessing Medical Fitness to Drive. Clinical Medicine & Research Vol 1 2003; 3: 177-188 Various manifestations of vision impairment
- Insurance Institute for Highway Safety. Status report: special issue: older drivers.8 September 2001;36:1–7.
- Owsley C, McGwin G. Vision Impairment and Driving. Surv Ophthal1999;43:535–50.
- Koepsell TD, Wolf ME, McCloskey L, et al. Medical conditions and motor vehicle collision injuries in older adults. J Am Geriatr Soc 1994;42:695–700.
- Hemmelgarn B, Le´vesque LE, Suissa S. Anti-diabetic drug use and the risk of motor vehicle crash in the elderly. Can J Clin Pharmacol 2006;13:112–20.
- McGwin G Jr, Sims RV, Pulley L, et al. Relations among chronic medical conditions,medications, and automobile crashes in the elderly: a population-based case-control study. Am J Epidemiol 2000;152:424–31.
- Margolis KL, Kerani RP, McGovern P, et al. Risk factors for motor vehicle crashes in older women. J Geront 2002;57A:186–91M.
- King D, Benbow SJ, Barrett JA. The law and medical fitness to drive–a study of doctors’ knowledge. Postgrad Med J 1992;68:624-628.
- Drickamer MA, Marottoli RA. Physician responsibility in driver assessment. Am J Med Sci 1993;306:277-281.
Leave a Comment